Secondary Postpartum Hemorrhage and Endometritis | 30 |
In the postpartum period, secondary postpartum hemorrhage (SPPH) and endometritis are two conditions that frequently present to an obstetric triage unit. These complications may coexist and can occur from 24 hours postpartum to 6 weeks postdelivery. SPPH is typically not as severe as a primary bleeding episode. Only 10% of the time will the hemorrhage be significant enough to cause a change in vital signs (Neil & Thorton, 2002). Likewise, postpartum women ultimately diagnosed with endometritis are generally stable, but less commonly can present in septic shock. In the obstetric triage or emergency setting, continual monitoring of vital signs is essential as healthy, young women frequently maintain their vital signs, only to quickly decompensate as the hemorrhage or infection continues.
SECONDARY POSTPARTUM HEMORRHAGE
Secondary postpartum hemorrhage is diagnosed following 0.5% to 2% of deliveries in developed countries (Lu et al., 2005). There are no randomized controlled trials to guide the evaluation and treatment as in primary postpartum hemorrhage, but guiding principles for managing hemorrhage remain the same.
PRESENTING SYMPTOMATOLOGY
The postpartum woman often presents with a sudden increase in bleeding, after having experienced a tapering of normal lochia. Pain may or may not be present. Fever and uterine tenderness may be present if an infection coexists.
HISTORY AND DATA COLLECTION
The initial history includes quantifying the amount of bleeding. Symptoms of clinically significant anemia, such as shortness of breath, lightheadedness, heart racing, or syncope, are solicited. A determination of the specific cause of the hemorrhage may assist in forming the treatment plan. Therefore, a thorough history includes prior obstetric procedures, fertility treatments, and other surgeries that have been associated with specific conditions such as an 358intrauterine aneurysm or placental abnormalities (Kovo, Behar, Friedman, & Mailinger, 2007). Any history of bleeding in the initial postpartum period is significant since two-thirds of women with SPPH will have experienced a primary hemorrhage. In these cases, the pace of the evaluation must be prioritized, as significant anemia may already precede the second bleeding episode. Details about bleeding disorders are solicited as one-third of women who experience a SPPH have Von Willebrand’s disease (Barbarinsa, Hayman, & Draycott, 2011). The delivery record is reviewed and the following are noted: length of rupture of membranes, length of labor, augmentation of labor, any diagnosis of chorioamnionitis, and blood counts available prior to the time of initial discharge. In addition, there is a review of how the placenta was delivered, especially noting if manual removal of the placenta was required or if any abnormalities were observed on inspection of the placenta. The mode of delivery is another key piece of history, since retained products as a cause for the hemorrhage is less likely with cesarean birth. The mean time between delivery and SPPH was 13.4 days in a recent cohort study (Dossou, Debost-Legrand, Dechelotte, Lemery, & Vendittelli, 2015).
PHYSICAL EXAMINATION
In obstetric triage, vital signs need to be noted immediately. It is critical to remember that in a healthy woman, over 1 L of estimated blood loss can occur before there is a significant change in vital signs. Therefore, vital signs will need to be trended regularly and monitored for increasing tachycardia, hypotension, and decreasing oxygen saturation. A fever is suggestive of a coexisting infection. Skin color and capillary refill are helpful physical indicators of hemoglobin levels. Abdominal palpation of the postpartum uterus for tenderness and size is informative. An enlarged uterus may suggest that retained products of conception are a factor in the bleeding. A pelvic examination is performed to examine the vagina and cervix for lacerations. The presence of foul smelling lochia in the vagina and notation as to whether or not the woman is still actively bleeding are additional key findings on pelvic examination.
LABORATORY AND IMAGING STUDIES
Essential laboratory tests include a complete blood count, coagulation profile, type and screen, and/or cross match, if indicated. A radiology ultrasound is indicated if the woman is clinically stable. If there is hemodynamic instability, a bedside ultrasound can be useful in quickly determining a cause for the SPPH. If the uterine cavity is distended and full of heterogeneous material, especially if blood flow is seen when the color Doppler function is applied, then retained products of conception is the likely diagnosis. Figure 30.1 represents a sonographic image of retained products of conception, subsequently confirmed at the time of dilatation and curettage.
It may be normal to see fluid and mixed echogenicity within the uterine cavity while performing ultrasonography on an involuting, postpartum uterus, depending on how much time has elapsed since delivery. The maximum thickness of the intrauterine contents is noted. Hematometra and clots will not typically demonstrate blood flow on ultrasound color Doppler flow. If flow to the intrauterine contents is noted, it is more likely to represent retained products of conception (Multic-Lutvica & Axelsson, 2006). Additional pathologic findings that can be diagnosed by ultrasound include fibroids or intrauterine vascular malformations.
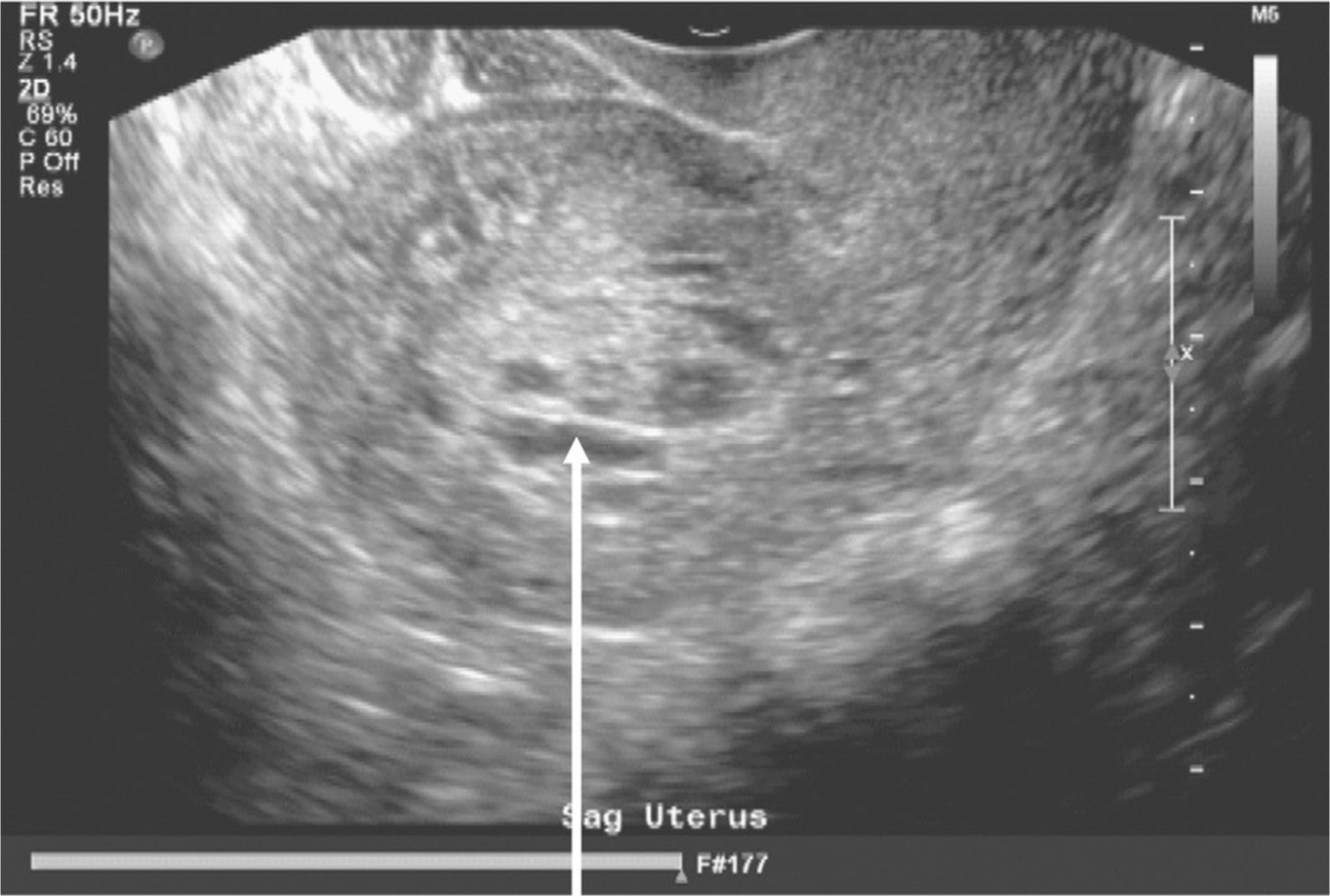
Figure 30.1 Retained products of conception
Source: Courtesy of Department of Radiology, Women & Infants Hospital, Providence, RI.
EXHIBIT 30.1
Causes of Secondary Postpartum Hemorrhage
• Idiopathic subinvolution of the uteroplacental vessels
• Retained placental tissue
• Endometritis
• Placenta accreta, increta, or percreta
• Von Willebrand’s disease
• Fibroids
• Vascular malformation of the uterus including A-V malformations and uterine artery aneurysms
Source: Adapted from Barbarinsa et al. (2011).
DIFFERENTIAL DIAGNOSIS
The primary differential in SPPH is menses and secondarily postpartum bleeding that is within the normal range, but bothersome to the woman. Rarely, cancers can present as late postpartum bleeding both with an acute bleed or persistent postpartum bleeding (Riggs, Zaghami, Najid, Haber, & Schreffler, 2010). If SPPH is diagnosed, the determination of the cause of the hemorrhage will assist in formulating an appropriate treatment plan. Exhibit 30.1 lists the causes of SPPH, appearing in order of decreasing incidence (Barbarinsa et al., 2011).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


