Pulseless Cardiac Arrest
Peter J. Kudenchuk
The most critical interventions during the first minutes of a cardiac arrest are immediate bystander cardiopulmonary resuscitation (CPR) providing high-quality chest compressions with minimal interruption.
Primary emphasis on high quality uninterrupted chest compressions and CPR
Immediate defibrillation for ventricular fibrillation (VF)/pulseless ventricular tachycardia (VT)
Secondary emphasis on vasoactive agents and endotracheal intubation
Coordinated team approach with defined team leader
Pulseless Arrest Due to Ventricular Fibrillation or Pulseless VT
Pulseless cardiac arrest is caused by four rhythms: VF, pulseless VT, asystole, or pulseless electrical activity (Fig. 21-1). The basic life support (BLS) algorithm is followed (see Chapter 11, Fig. 11-2); an automatic electrical defibrillator (AED) or manual defibrillator is placed as soon as possible and the rhythm determined (Fig. 21-1, Box 2). Based upon rhythm analysis, a shockable or nonshockable rhythm is determined to be present and further interventions are based on the type of rhythm (Boxes 3 and 9).
The 2005 AHA ECC guidelines gave renewed emphasis to the importance of high-quality, minimally interrupted CPR during the course of resuscitation. A single-shock strategy with subsequent shocks separated by 2 minutes (five cycles) of CPR also displaced the former algorithm of three serial “stacked” shocks. This was recommended in part because it was recognized that serial AED analyses and repeated shocks have limited yield and can deprive patients in cardiac arrest of needed CPR for protracted periods of time.1,2 For similar reasons, it is now recommended that 2 minutes (five cycles) of CPR be interposed before rhythm and pulse checks following all interventions, including shock. In the current AHA ECC guidelines, pharmacologic therapies (epinephrine or vasopressin) to bolster coronary perfusion pressure are recommended after failure of one or more shocks, and antiarrhythmic therapies for recurrent or resistant VF/VT are recommended after failure of two or more shocks to restore an organized perfusing rhythm. In particular, patients in whom a perfusing rhythm can be transiently restored but not successfully maintained between repeated shocks (recurrent VF/VT) are appropriate candidates for early treatment with antiarrhythmic medications. In such patients the antiarrhythmics may facilitate and stabilize the return of circulation that shock alone has failed to accomplish. As is true for virtually all interventions, the likelihood of benefit from antiarrhythmic drug therapies declines rapidly with the lengthening duration of cardiac arrest.
Defibrillation
The optimal number of attempted defibrillatory shocks that should be administered for refractory VF/VT before initiating pharmacologic therapy is unknown. Traditionally, given the established efficacy of early defibrillation, pharmacologic therapy was recommended after at least three precordial shocks failed to restore a stable perfusing rhythm.
If VF/pulseless VT is present (Fig. 21-1, Box 3), providers should deliver one shock (Box 4) and then resume CPR immediately, beginning with chest compressions. If a biphasic defibrillator is available, providers should use the dose at which that defibrillator has been shown to be effective for terminating VF (typically a selected energy of 120–200 J). If the provider is unaware of the effective dose range of the device, a dose of 200 J for the first shock may be used and an equal or higher shock dose for the second and subsequent shocks. If a monophasic defibrillator is used, providers should deliver an initial shock of 360 J and use that dose for subsequent shocks. If VF is initially terminated by a shock but then recurs later in the arrest, subsequent shocks may be delivered at the previously successful energy level.
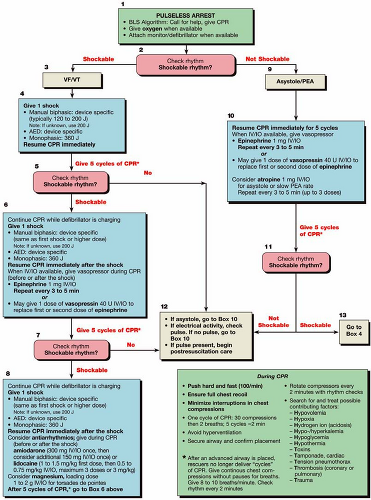 Figure 21-1 • Pulseless cardiac arrest algorithm. |
Intravenous Access, Pharmacologic Therapy, and Endotracheal Intubation
Establishing IV access is important (see below), but it should not interfere with CPR and the delivery of shocks. The pulseless arrest algorithm (Fig. 21-1
 Emergency Department Management of Acute Coronary Syndromes
Emergency Department Management of Acute Coronary Syndromes
 Heart Failure and Acute Pulmonary Edema in the Emergency Department
Heart Failure and Acute Pulmonary Edema in the Emergency Department
 Circulatory Adjuncts to Improve Coronary Perfusion Pressure
Circulatory Adjuncts to Improve Coronary Perfusion Pressure
 Basic Life Support: Science to Survival
Basic Life Support: Science to Survival
 Endotracheal Intubation and Management of the Difficult Airway
Endotracheal Intubation and Management of the Difficult Airway
 Oxygen Administration and Supraglottic Airways
Oxygen Administration and Supraglottic Airways




Related posts:
Emergency Department Management of Acute Coronary Syndromes
Heart Failure and Acute Pulmonary Edema in the Emergency Department
Circulatory Adjuncts to Improve Coronary Perfusion Pressure
Endotracheal Intubation and Management of the Difficult Airway
Oxygen Administration and Supraglottic Airways
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
