Podiatric (Foot and Ankle) Pain
This chapter presents the most common clinical causes of chronic pain in the foot and ankle. They include plantar fasciitis, hallux valgus (bunion), Morton’s neuroma, tarsal tunnel syndrome, and diabetic peripheral neuropathy. The focus of this chapter will be on pain that originates from the foot and ankle. Note, however, that pain originating from the lumbar spine can present as foot-and-ankle pain. Nerves come out of the lumbar spine and down into the legs, acting as the control center for both sensation and movement of the lower extremities. In the case of concurrent back and leg pain, it is important to image the lumbar spine with an MRI. This is covered in Chapter 2, Neuropathic Pain, in the section Lumbar Radiculopathy.
If the pain is located solely at the foot (pardon the pun) or ankle, then a proper history and examination will be key in securing a diagnosis.
Pain in the Heal and Bottom of the Foot
Plantar Fasciitis
The plantar fascia is a thick, fibrous tissue that runs along the plantar surface of the foot. Its function is to provide support for the longitudinal arch of the foot and act as a shock absorber. Pain is caused by inflammation of the plantar fascia at its insertion site on the medial aspect of the calcaneal tuberosity (heel; Fig. 6-1). Patients with pes
planus (low arch) or pes cavus (high arch) feet have an increased stress placed on the plantar fascia. There is a high incidence of plantar fasciitis in runners, which is possibly caused by repeated microtrauma. Pain is often most severe at the anterior aspect of the heel. It has been estimated that 1,000,000 patient visits per year are because of plantar fasciitis.
planus (low arch) or pes cavus (high arch) feet have an increased stress placed on the plantar fascia. There is a high incidence of plantar fasciitis in runners, which is possibly caused by repeated microtrauma. Pain is often most severe at the anterior aspect of the heel. It has been estimated that 1,000,000 patient visits per year are because of plantar fasciitis.
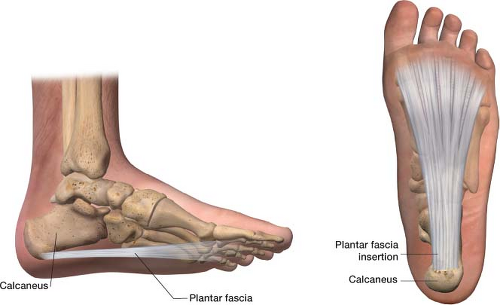 Figure 6-1 The plantar fascia at its insertion site on the medial aspect of the calcaneal tuberosity (heel). |
In plantar fasciitis there is an intensely sharp heel pain with the first few steps of the morning. Early in the morning the plantar fascia is constricted and tight—this is intensified in plantar fasciitis. The pain will decrease during the day as the plantar fascia becomes more flexible.
On physical examination, you can usually reproduce the pain by palpation of the medial anterior aspect of the heel (Fig. 6-2). In the windlass test, the patient puts weight on the heel while the examiner dorsiflexes the toes to reproduce the pain. Clinically, if there is more pain on the lateral aspect of the heel versus the medial aspect, a calcaneal stress fracture should be ruled out. If you suspect plantar fasciitis and the symptoms do not resolve with conservative treatment, an x-ray is warranted. Radiographs may show a plantar heel spur in 50% of patients with plantar fasciitis, but it is important to remember that many asymptomatic patients have heel spurs.
First-line treatment includes physical therapy (calf and Achilles tendon stretching), ice, and an anti-inflammatory medication (e.g., nonsteroidal anti-inflammatory drugs, NSAIDs). A patient’s shoes should also be replaced and proper arch support provided to match the patient’s feet.
Night splints may be very effective in treating plantar fasciitis. People naturally sleep with their feet in a plantar-flexed position, which causes the plantar fascia to be shortened. Night splints keep the ankles in a neutral position, which causes passive stretching of the plantar fascia overnight (Fig. 6-3). This allows the plantar fascia to heal in the elongated position, decreasing tension on the fascia with the first step in the morning. Studies have shown that 80% of patients using night splints had improvement of their plantar fasciitis.3
 Figure 6-2 Palpation of the medial anterior aspect of the heel reproduces the pain of plantar fasciitis. |
 Figure 6-3 Night splints allow for the lengthening of the plantar fascia at night which can help alleviate plantar fasciitis. |
A cortisone injection to decrease inflammation can be very helpful (Fig. 6-4). The physician identifies the medial aspect of the calcaneal bone and palpates the soft tissue, locating the point of maximal tenderness or swelling. This area is marked with a felt-tip marking pen. The area is prepped in standard sterile fashion. As a therapeutic agent I use 40 mg of Kenalog mixed with 3 mL of 0.25% bupivacaine in a 5-mL syringe. The needle is a 1.5-in, 22 gauge needle. The needle angle is perpendicular to the skin and introduced through the skin to the tendon sheath. The medication is then
injected at the heel. A cortisone injection can slightly increase the risk of plantar fascia rupture. In 95% of patients with plantar fasciitis, symptoms resolve within 12 to 18 months. In cases that are refractory to conservative treatment, a surgical release of the plantar fascia can be performed.
injected at the heel. A cortisone injection can slightly increase the risk of plantar fascia rupture. In 95% of patients with plantar fasciitis, symptoms resolve within 12 to 18 months. In cases that are refractory to conservative treatment, a surgical release of the plantar fascia can be performed.
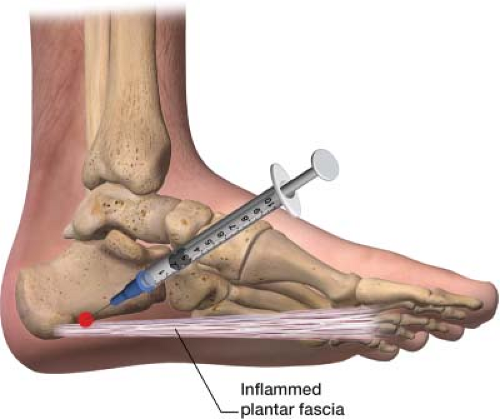 Figure 6-4 Plantar fasciitis injection at the incretion site of the plantar fascia to the medial aspect of the calcaneus bone. |
Pain on the Side of the Big Toe
Hallux Valgus (Bunion)
Hallux is the big toe and valgus is an abnormal displacement of a body part away from the midline of the body. The distal aspect of the first metatarsal deviates away from the midline of the body, away from the second toe so that it causes an outward bump (Fig. 6-5). The medial eminence of the first metatarsophalangeal joint becomes prominent, often referred to as a bunion. Bunion is the Greek word for turnip. The most common cause of hallux valgus is biomechanical instability. When we walk or run, roughly 65% of dorsiflexion is focused on the first metatarsophalangeal joint. This intense force makes the first metatarsal vulnerable for the development of hallux valgus. The more the big toe shifts into a valgus position the greater mechanical advantage it has, to a point. Patients present with complaints of pain over the medial eminence, made worse with tight shoes.
This condition affects roughly 1% of the North American population, but the incidence has been shown to be as high as 15% in those older than 60 years of age. Tight dress shoes worn by many women are more constraining than the shoes worn by men and are believed by many podiatrists to be a common factor in many cases of hallux valgus. This could explain the 10:1 female to male ratio seen with this disorder.
In hallux valgus (bunion), patients often present with pain at the first metatarsophalangeal joint during ambulation. Often the pain is relieved with removal of tight-fitting shoes. If the patient notes a burning pain in this area along with deep, achy pain, there may also be entrapment of the medial dorsal cutaneous nerve (Fig. 6-6). Medial dorsal cutaneous nerve pain is often described as burning and electric. While taking a history, determine how the pain affects the patient’s quality of life. Some patients with larger deformities have mild discomfort and are not particularly affected, whereas some patients with smaller deformities are severely affected. On examination evaluate: (1) Hallux (big toe) position, (2) medial prominence (how big the bump is), and (3) range of motion of the metatarsophalangeal joint. Normal range of motion is 65 degrees with dorsiflexion and 15 degrees with plantar flexion. Obtain x-rays of weight-bearing feet, including anteroposterior, lateral oblique, and lateral views.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


