Peripheral Neuropathy
Henry Cohen MS, PharmD
Dalia Abdelmacksoud PharmD
Joanne V. Hickey PhD, RN, CS, ACNP, CNRN, FAAN
Peripheral neuropathy (PN) is a serious complication that occurs in a myriad of clinical conditions treated by the primary care provider. PN is defined as deranged function and structure of peripheral motor, sensory, and autonomic neurons, involving either the entire neuron or selected levels. The disorders of the peripheral nervous system are clinically diverse and depend on the severity of the pathologic process, the rate of progression, the population of neurons or Schwann cells affected, the level within the neurons affected, and the subcellular pathologic events involved (Ziegler, 1996; Brew, 1994).
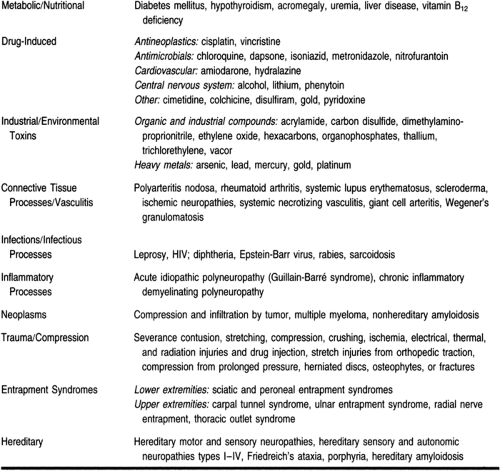
PN may manifest a wide variety of signs and symptoms, including burning sensations, paresthesias and dysesthesias, and a “pins and needles” sensation. Underlying disease states that may cause PN include diabetes mellitus (DM; Llewelyn, 1995; Ziegler, 1996), HIV infection, uremia, neoplasms, and chronic alcohol abuse. Nutritional deficits in thiamine, pyridoxine, or cyanocobalamin may cause PN (Kelly, 1994). Drugs have also been implicated in causing PN and are listed in Table 56-1. Environmental toxins, including heavy metals such as lead and mercury, have also been implicated.
 |
ANATOMY, PHYSIOLOGY AND PATHOLOGY
Each peripheral nerve has a well-defined anatomic course, supplies a dermatome (although there is some overlap), and innervates specific muscles. The proximity of some nerves to bony structures makes them particularly vulnerable to compression or entrapment injury. Although there are several etiologies for PN, the pathologic processes can generally be divided into four categories: wallerian degeneration, axonal degeneration, neuropathy, and segmental demyelination (Bosch & Mitsumoto, 1991).
An injury that causes interruption of the axon and myelin, as in a transection of a nerve, results in wallerian degeneration distal to the injury site. In this distal segment, the myelin and axon degenerate, resulting in a loss of electrical conduction. Proximal to the transection, regrowth may occur, but it is slow and often incomplete, and the recovery of the nerve is limited. Axonal degeneration refers to distal axonal breakdown resembling wallerian degeneration, but it is the result of metabolic derangement within neurons (eg, DM, toxins). This results in denervation of the muscle and muscle atrophy.
Neuropathy refers to primary loss or destruction of nerve cell bodies, along with degeneration of their entire peripheral and central processes. Inherited conditions such as spinal muscular atrophies (lower motor neurons) and hereditary sensory neuropathies (primary sensory neurons) may be affected. Toxins and organic compounds such as mercury and pyridoxine overdose can result in primary neuronal degeneration (Bosch & Mitsumoto, 1991). Segmental demyelination (eg, Guillaine Barrè syndrome) is an injury of the myelin sheath or the myelin-producing Schwann cells, resulting in breakdown of myelin with relative sparing of axons so that no atrophy occurs unless nerve fibers are affected, as can occur in severe cases.
There are two broad classes of peripheral nerve injury. Mononeuropathies are focal lesions of peripheral nerves (eg, traumatic or ischemic). Polyneuropathies are bilateral symmetric disturbances of function (eg, toxic, hereditary, inflammatory, or metabolic). Multifocal isolated lesions are termed “mononeuropathy multiplex” and most commonly affect peroneal, median, and ulnar nerves.
Most PNs are associated with a loss of function, either sensory, motor, or both, and are typically not painful. Pain is characteristic of diabetic, alcoholic, and nutritional deficiency neuropathies.
Diabetic PN
The exact etiology and pathogenesis of diabetic PN has not been well elucidated and may be multifactorial. Chronic hyperglycemia has been associated with diminished nerve conduction velocity and the clinical presentation of PN. Glucose is usually metabolized by hexokinase to glucose-6-phosphate. In the presence of constant hyperglycemia, saturation of the hexokinase enzymatic pathway occurs, and excess glucose is converted to sorbitol by the polyol pathway.
A likely mechanism for the pathogenesis of human diabetic neuropathy is increased polyol pathway activity secondary to diabetic hyperglycemia. During hyperglycemia, however, the cellular level of glucose increases in tissues such as the peripheral nerve, where glucose entry is independent of insulin.
In peripheral nerve tissues, the excess glucose is metabolized predominantly by aldose reductase. Increased flux of glucose through the polyol pathway may be associated with myoinositol depletion, decreased sodium-potassium ATPase activity, decreased nitric oxide synthetase, tissue hypoxia, and subsequent structural lesions.
Aldose reductase inhibitors block the flux of glucose through the pathway and prevent these abnormalities. Aldose reductase inhibitors are under clinical investigation for the treatment and prophylaxis of diabetic PN.
HIV PN
PNs are a common complication of HIV disease, occurring at all stages of infection. Acute PN in HIV disease may be an early feature of the infection, especially around the time of seroconversion
(Brew, 1993). HIV-related PN may manifest in a variety of forms: a predominantly sensory neuropathy, an autonomic neuropathy, a mononeuritis multiplex, or an inflammatory demyelinating polyneuropathy. One of the distinguishing features of the neuropathies that occur in HIV patients is the relative specificity of the individual neuropathic syndromes with the stages of infection.
(Brew, 1993). HIV-related PN may manifest in a variety of forms: a predominantly sensory neuropathy, an autonomic neuropathy, a mononeuritis multiplex, or an inflammatory demyelinating polyneuropathy. One of the distinguishing features of the neuropathies that occur in HIV patients is the relative specificity of the individual neuropathic syndromes with the stages of infection.
Neuropathies may be the result of immunopathogenic events, such as the inflammatory demyelinating polyneuropathies. During the early stages of infection, the immune system is relatively competent but is stimulated and has altered responsiveness. A vasculitic syndrome occurs mainly during the early symptomatic phase of infection and has been postulated to be the result of circulating immune complexes of HIV-1 antibody and antigen that are deposited in vessel walls.
Distal symmetric polyneuropathy occurs mainly in the late phase of HIV infection (AIDS), when there is severe immunosuppression. At this stage the mechanisms that have been proposed include productive infection of neural tissue with HIV-1 or cytomegalovirus or toxic or metabolic abnormalities as a result of advanced systemic disease.
Another possible mechanism for HIV PN is a dysregulation of macrophages within the peripheral nerve, resulting in excessive production of tumor necrosis factor and other interleukins. Additional factors that may damage the peripheral nerves in HIV patients include gp-120 (the coat protein of HIV virus) or a nutritional deficiency (eg, vitamin B12).
The most common neuropathy is a predominantly sensory neuropathy presenting distally and symmetrically with little functional weakness. Predominantly sensory neuropathies are a common feature of advanced HIV disease, with an estimated prevalence of 45% in AIDS patients.
Toxin-Induced PN
Exposure to environmental, biologic, and experimental toxins, metals, and drugs can produce neurologic manifestations resulting from impaired function of the central and peripheral nervous systems. Metals that are associated with PN include mercury, lithium, gold, and platinum. Sources of human exposure to neurotoxins include occupational exposure, environmental contamination, drug therapy, and food poisoning. Botulinum toxin, a potent neurotoxin, causes paralysis when ingested in contaminated foods.
Neoplasm PN
Neoplasm PN is most common in carcinoma of the lung, but it is also associated with carcinoma of the stomach, colon, rectum, and other organs. It is difficult to ascertain the prevalence
of PN in malignancy, because it depends on the pathologic type and site of the tumor, the stage and duration of the illness, the techniques for diagnosis used, and the criteria for diagnosis. Pathogenic mechanisms for neoplasm-associated PN include direct infiltration of roots and nerves by tumor cells, toxic factors released by the tumor, alterations in protein and fat metabolism as a result of the tumor, nutritional deficiencies, vascular causes, viral infections, and immunologic disturbances.
of PN in malignancy, because it depends on the pathologic type and site of the tumor, the stage and duration of the illness, the techniques for diagnosis used, and the criteria for diagnosis. Pathogenic mechanisms for neoplasm-associated PN include direct infiltration of roots and nerves by tumor cells, toxic factors released by the tumor, alterations in protein and fat metabolism as a result of the tumor, nutritional deficiencies, vascular causes, viral infections, and immunologic disturbances.
Alcoholic PN
Despite the observation that chronic excessive alcohol ingestion is associated with peripheral nerve disease, there is still controversy about whether the neuropathy is the result of a direct toxic effect of alcohol, malnutrition, or both. Human studies have not been able to differentiate a direct toxic action of alcohol on the peripheral nervous system from the effects of poor nutrition. The neuropathy observed may be the result of a deficiency in vitamin B1, niacin, vitamin B6, vitamin B12, or vitamin E.
Neuropathy Associated With Renal Failure
PN became clearly established as a complication of chronic renal failure in the early 1960s. In progressive chronic renal failure, slowing of nerve conduction tends to occur when creatinine clearance is approximately 10% of normal. Nerve conduction continues to worsen as renal function deteriorates. The diminished nerve conduction occurs proximally and distally to the same degree. Uniform generalized slowing of conduction tends to occur subclinically and does not predict the appearance of clinical signs and symptoms of neuropathy.
The subclinical diminished nerve conduction in chronic renal failure is functional and is not accompanied by evident renal morphologic change; thus, it is readily reversible by restoration of normal renal function. Chronic dialysis may prevent, stabilize, or improve uremic neuropathy, but dialysis has relatively little effect on nerve conduction velocity. Other observations suggest widespread axonal dysfunction in chronic renal failure (Aminoff et al, 1996).
EPIDEMIOLOGY
An accurate accounting of the epidemiology of PN is unknown because, in most instances, the neuropathy is part of a clinical presentation or a complication associated with a long-term, chronic condition (eg, DM, alcoholism, or exposure to toxins). DM is the most common human metabolic disease (5 million cases in the United States), and diabetic neuropathy is the most common complication of DM.
Forty percent of patients with insulin-dependent DM for greater than 20 years and 5% to 10% of patients with noninsulin-dependent DM develop neuropathies. The incidence is declining, perhaps as a result of improved glycemic control (Greene, 1994).
Neuropathies associated with toxic substances used in industries such as farming or the oil industry are seen in such workers (Table 56-2). The incidence of toxin-related neuropathies is not known, partly because of the long delay (often more than 20 years) between exposure and development of symptoms.
 |
Thirty percent of all cases of PN are attributed to alcoholic neuropathy. A close association between alcoholic neuropathy and nutritional deficiency has also been noted (Bosch & Mitsumoto, 1991).
Entrapment syndromes are more common in persons who use their hands in repetitive motions, such as musicians, hairdressers, and computer users. The risk of developing carpal tunnel syndrome is more than doubled in persons with DM.
Although a few conditions produce mononeuropathy and mononeuropathy multiplex, there are many etiologies of polyneuropathy. Diagnosis often depends on obtaining a thorough history (eg, alcohol abuse or occupational exposures and risk factors), identifying systemic conditions associated with neuropathies (eg, DM, systemic lupus erythematosus), and conducting a careful physical and neurological exam.
DIAGNOSTIC CRITERIA
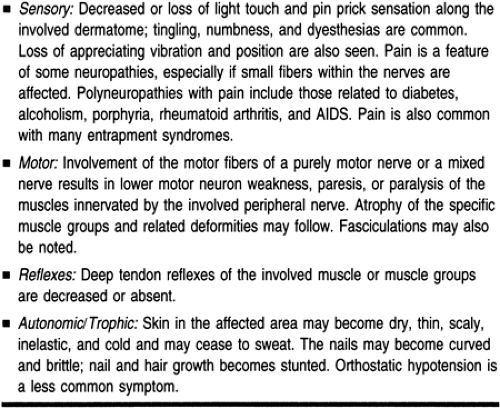
Disorders of one or more peripheral nerves cause various signs and symptoms that correspond to the anatomic distribution and normal function of the peripheral nerve. Some peripheral nerves are purely motor, some are purely sensory, and others are mixed. Diagnostic accuracy depends on a thorough knowledge of specific sensory dermatomes, muscle innervations, reflexes, and autonomic function related to a particular nerve. The signs and symptoms of a peripheral nerve disorder may include sensory, motor, reflex, or autonomic/trophic disturbances (Table 56-3) (Brazis et al, 1990; Aminoff et al, 1996):
 |
Classification of Neuropathies
PNs are classified based on the number of peripheral nerves involved and the pattern of involvement (eg, symptoms may be confined to one side or both). The classification includes:
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


