Fig. 58.1
Anatomy. (1) Aorta and inferior vena cava, (2) superior hypogastric plexus, (3) pelvic (inferior hypogastric plexus), (4) lumbosacral sympathetic ganglia (5) lumbosacral plexus (Reproduced with permission from Danilo Jankovic)
Fig. 58.2
Peripheral pain pathways during labor (Reproduced with permission from Danilo Jankovic)
Indications
Paracervical block has a limited role in modern obstetric practice, except in cases where central neural blockade is not feasible or is unavailable.
Surgical
1.
Bilateral block may be used for dilatation of the cervix and uterine curettage.
2.
Occasionally, it may be combined with pudendal nerve block and local infiltration to perform a vaginal hysterectomy.
Vaginal Delivery
Bilateral paracervical block alleviates the pain of the first stage of labor, and this is the most frequent use of this block.
Avoid: in prematurity, fetal distress, and uteroplacental insufficiency.
Therapeutic
1.
Relief of severe dysmenorrhea
2.
Endometritis and parametritis
Diagnostic
Differentiation of severe dysmenorrhea from other similar complaints which may be associated with menstruation.
Materials
The IOWA trumpet, Kobak instrument, is used as a guide for the placement of the needle (20-gauge, 12–14 cm needle) (S. Chap. 56, Pudendal nerve block).
Technique
Paracervical and uterosacral blocks are identical procedures and the local anesthetic solution bathes the same plexus and ganglia. If the solution is deposited at the 3 and 9 o’clock positions, the block is termed paracervical, and if the solution is deposited at the 4 and 8 o’clock positions, the block is termed uterosacral (Fig. 58.4). The pelvic (inferior hypogastric) ganglia and plexus are anesthetized when this block is performed.
Position and Landmarks
The patient is placed in the supine position with her legs apart and partially in the lithotomy position. The injection is made in the lateral fornices of the vagina.
1.
Vaginal examination should be performed immediately before the block to determine the precise position of the presenting part.
2.
Maternal and fetal vital signs should be determined immediately before the block.
Procedure
1.
Get Clinical Tree app for offline access

The needle is introduced through the submucosa into the lateral vaginal fornix (Fig. 58.3).
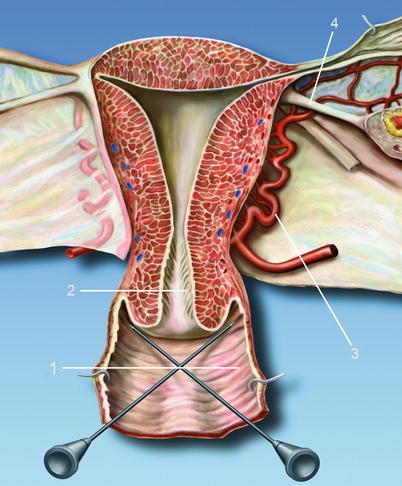
Fig. 58.3




The needle is introduced through the submucosa into the lateral vaginal fornix. (1) Lateral vaginal fornix, (2) ostium uteri, (3) uterine artery, (4) round ligament of uterus (Reproduced with permission from Danilo Jankovic)
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree