Noninvasive Positive-Pressure Ventilation: Introduction
Noninvasive ventilation (NIV) refers to the provision of mechanical ventilation without the need for an invasive artificial airway. Many different approaches to assisting ventilation noninvasively have been used in the past, including negative-pressure ventilators, pneumobelts, and rocking beds (see Chapters 16 and 17).1 By virtue of its effectiveness and convenience compared with other noninvasive approaches, however, noninvasive positive-pressure ventilation (NIPPV) using a mask (or interface) that conducts gas from a positive-pressure ventilator into the nose or mouth has become the predominant means of administering NIV throughout the world. NIPPV has long been used to treat chronic respiratory failure caused by chest wall deformities, slowly progressive neuromuscular disorders, or central hypoventilation.2 In more recent years, NIPPV has been increasingly used to treat patients with various forms of acute respiratory failure.3 For the purposes of this discussion, NIPPV refers to active ventilator assistance achieved by the noninvasive provision of a mechanical positive-pressure breath during inhalation, and continuous positive airway pressure (CPAP) refers to the provision of a nonfluctuating positive-pressure. This chapter discusses the rationale for use, evidence for efficacy of noninvasive positive-pressure techniques in both acute and chronic settings, selection of appropriate patients, techniques for administration, and pitfalls and complications.
Why Use Noninvasive Ventilation and How Does It Work?
NIV has become an integral component of ventilator support in both acute and chronic settings because it avoids the complications of invasive ventilation. Invasive mechanical ventilation is highly effective and reliable in supporting alveolar ventilation, but endotracheal intubation carries well-known risks of complications that have been described elsewhere in detail (see Chapter 39).4,5 These complications have been lumped into three main categories: complications related to insertion of the tube and mechanical ventilation, those caused by loss of airway defense mechanisms, and those that occur after removal of the endotracheal tube.4
In the first category, aspiration of gastric contents; trauma to the teeth, hypopharynx, esophagus, larynx, and trachea; arrhythmias; hypotension; and barotrauma may occur during placement of a translaryngeal tube.6,7 Tracheostomy tube placement incurs risks of hemorrhage, stomal infection, intubation of a false lumen, mediastinitis, and acute injury to the trachea and surrounding structures, including tracheal rupture,8 and esophageal and vascular injury.6 In the second category, endotracheal tubes serve as a source of continual irritation, interfere with airway ciliary function, and require frequent suctioning that contributes to airway injury, patient discomfort, and mucus hypersecretion. They also provide a direct channel to the lower airways for microorganisms and other foreign materials, leading to biofilm formation, chronic bacterial colonization, and ongoing inflammation. As a consequence, health care–acquired pneumonias are seen in up to 20% of mechanically ventilated intensive care unit (ICU) patients (see Chapter 46),9 and sinusitis is seen in 5% to 25% of nasally intubated patients, related to blockade of the sinus ostia and accumulation of infected secretions in the paranasal sinuses (see Chapter 47).10 In the third category, hoarseness, sore throat, cough, sputum production, hemoptysis, upper airway obstruction secondary to vocal cord dysfunction or laryngeal swelling, and tracheal stenosis all may follow extubation.11
In addition, from the point of view of the patient, translaryngeal intubation is uncomfortable and compromises the ability to eat and communicate, contributing to feelings of powerlessness, isolation, and anxiety.12 This increases the need for sedation, delaying weaning, prolonging the duration of invasive mechanical ventilation, and potentiating the risks of further complications. If tracheostomy placement becomes necessary, sophisticated equipment including suctioning paraphernalia and a high level of technical expertise among caregivers are required. Tracheostomies promote upper airway colonization with gram-negative bacteria, increasing the risk of pneumonias.7 Furthermore, long-term tracheostomies are complicated by tracheomalacia, granulation tissue formation, and tracheal stenoses that sometimes obstruct the airway, chronic pain, and tracheoesophageal or even tracheoarterial fistulas.11 These considerations and potential complications may limit the options for chronic care placement, add substantially to the costs of care,13 and even preclude home discharge in patients with limited caregiver and financial resources.
NIV can avoid many of these complications if candidates are selected properly using guidelines that are discussed in detail later. NIV leaves the upper airway intact, preserves airway defense mechanisms, and allows patients to eat, drink, verbalize, and expectorate secretions. NIPPV reduces the infectious complications of mechanical ventilation, including nosocomial pneumonia and sinusitis.14,15 It also enhances patient comfort, convenience, and mobility at no greater16 or even less13 cost than endotracheal intubation. NIV can be administered outside the ICU setting as long as adequate nursing and respiratory therapy support can be provided, allowing for more rational use of acute care beds, and it greatly simplifies care for patients with chronic respiratory failure in the home.
NIPPV improves the respiratory status of failing patients via a number of mechanisms. Most important, NIPPV reduces the work of breathing by the same mechanism as invasive positive-pressure ventilation: By applying supra-atmospheric pressure intermittently to the airways, it increases transpulmonary pressure, inflates the lungs, augments tidal volume, and unloads the inspiratory muscles. Exhalation is achieved by passive lung recoil. Studies in patients with severe stable chronic obstructive pulmonary disease (COPD) or restrictive thoracic disorders show that NIPPV reduces or, if inflation pressure is sufficient, even eliminates diaphragmatic work.17,18 In patients with severe COPD exacerbations, the addition of positive end-expiratory pressure (PEEP) to inspiratory pressure support further reduces the work of breathing by counteracting the effects of auto-PEEP. This combination (pressure support plus PEEP) lowers diaphragmatic pressure swings even more than with either pressure support or PEEP alone.19 These actions lead to a prompt reduction in respiratory rate, sternocleidomastoid muscle activity, dyspnea, and carbon dioxide (CO2) retention.
Other beneficial actions include an increase in functional residual capacity that opens collapsed alveoli, reducing shunt and enhancing ventilation–perfusion ratios in certain forms of respiratory failure, such as acute cardiogenic pulmonary edema. These effects improve oxygenation and may further reduce the work of breathing because the respiratory system is shifted to a more compliant position on its pressure-volume curve. In addition, CPAP alone (and with NIPPV) may improve left-ventricular function by virtue of an afterload-reducing effect of increased intrathoracic pressure.20 This effect occurs mainly in patients with dilated, hypocontractile left ventricles whose heart function is more dependent on afterload than on preload. The increased intrathoracic pressure reduces both preload and afterload, but the latter effect predominates, lowering transmyocardial pressure and enhancing cardiac output.21
A major effect of NIPPV that appears to be responsible for benefits reported in many studies, including reduced complication rates, mortality, and hospital lengths of stay, is a reduction in health care–acquired infections. Two prospective surveys14,15 observed roughly a fourfold reduction in the risk of health care–acquired pneumonia compared with physiologically matched endotracheally intubated patients, even after controlling for severity of illness. Patients treated with NIPPV also tend to receive fewer other invasive interventions, such as urinary bladder catheters or central intravenous lines,15 and this also likely contributes to a lower rate of health care–acquired infections and episodes of sepsis.
Despite the advantages of NIPPV related to the avoidance of airway invasion, the lack of a direct connection to the lower airway also poses a number of challenges. The patient must be able to protect his or her airway and clear secretions adequately, or failure is inevitable. The patient’s upper airway must permit airflow into the lungs, so NIPPV cannot be used in patients with high-grade, fixed, upper-airway obstructions. In addition, air leaks around the interface seal or via other routes are nearly ubiquitous with NIPPV and may interfere with the efficacy of ventilation. Furthermore, the patient must be able to cooperate and synchronize breathing with the ventilator, or no reduction in the work of breathing can be achieved, but the patient cannot be heavily sedated or paralyzed to achieve synchrony. Thus, patients who are to receive NIPPV must be selected carefully and managed with an eye to these limitations in ways that differ from the approach used for invasive mechanical ventilation.
Long-term NIPPV is used mainly nocturnally during sleep, when intermittent air leaking through the mouth or under the mask seal is universal, but sufficient air usually enters the lungs to assist ventilation.22 The adaptations that permit air entry into the lungs while NIPPV is administered during sleep are poorly understood, but resistance to airflow in the upper airway is undoubtedly an important factor. In one study, large amounts of air leaking through the mouth during nasal CPAP increased nasal resistance,23 an effect that was countered by provision of heated, humidified air, consistent with the idea that nasal mucosal cooling was responsible. Increases in nasal resistance secondary to this mechanism, upper airway infection, or allergy is likely to reduce delivered tidal volumes during nasal NIPPV. Passive positioning of the soft palate is also important in maintaining patency of the upper airway,24 as underlined by the observation that patients treated with nasal CPAP experience increased air leaking through the mouth after uvulopharyngoplasty.25
Glottic aperture is also important in determining the flow of gas into the lower airways during NIPPV. Compared with the awake state, the glottic aperture narrows and delivered tidal volume falls when NIPPV is administered during stage 1 or 2 sleep.26,27 In deeper sleep (stage 3 or 4), the glottic aperture widens, permitting more ventilation; if minute volume is increased excessively, however, the glottic aperture narrows once again, partly related to the reduction in the partial pressure of arterial carbon dioxide (PaCO2). These findings indicate that both sleep stage and the amount of ventilator assistance influence glottic aperture, which is a potentially important determinant of the efficacy of NIV. They also apply mainly to controlled modes of ventilation;28 glottic aperture is not as important when NIPPV is administered via a pressure-limited “bilevel” ventilator in the spontaneous mode.29
Three theories have been proposed to explain the mechanism by which stabilization of daytime gas exchange is achieved in patients with chronic respiratory failure who are receiving ventilator assistance for as little as 4 to 6 hours nightly. One postulates that NIV rests chronically fatigued respiratory muscles, thereby improving daytime respiratory muscle function.30,31 Supporting this theory are studies demonstrating that respiratory muscles do indeed rest during NIV;32–34 also, indices of respiratory muscle strength and endurance may improve in patients with chronic respiratory failure after varying periods of noninvasive ventilatory assistance.32–35 Conversely, chronic respiratory muscle fatigue has never been defined adequately or demonstrated convincingly; other studies have failed to demonstrate improvement in respiratory muscle function after initiation of NIV,36 and some studies have demonstrated that patients with neuromuscular disease have stable PaCO2 values for years despite a progressive decline in pulmonary function.37
A second theory proposes that NIV improves respiratory system compliance by reversing microatelectasis of the lung, thereby diminishing daytime work of breathing.38 This theory derives from studies showing improvements in forced vital capacity (FVC) without changes in indices of respiratory muscle strength after periods of positive-pressure ventilation. Once again, however, data are conflicting, with a number of studies showing no changes in vital capacity after periods of NIV.35,36 In addition, computed tomographic scanning of the chest indicates that microatelectasis is not an important contributor to chest wall restriction in patients with respiratory muscle weakness.
A third theory proposes that NIV lowers the respiratory center “set point” for CO2 by reversing chronic hypoventilation.30,39 During deeper stages of sleep, particularly rapid eye movement sleep, upper airway muscle tone and the activity of nondiaphragmatic inspiratory muscles diminish.40 This response may be exaggerated in patients with ventilatory impairment, leading to progressive nocturnal hypoventilation. Repeated episodes of nocturnal hypoventilation are thought to lead to a gradual accumulation of bicarbonate, desensitization of the respiratory center to CO2, and worsening of daytime hypoventilation.39 Nocturnal ventilator assistance reverses nocturnal hypoventilation and allows excretion of bicarbonate and a gradual downward resetting of the respiratory center set point for CO2, thereby reducing daytime hypercarbia. In addition, NIPPV may improve the quantity and quality of sleep by preventing hypoventilation-related arousals that lead to sleep fragmentation,41 reducing fatigue, and improving daytime function. Evidence for this theory derives from studies showing that when ventilator assistance is discontinued for a night in patients with chronic respiratory failure who have been using nightly NIV, the degree of nocturnal hypoventilation is less than before initiation, suggesting a resetting of respiratory center sensitivity for CO2.42 Also, nocturnal ventilation, oxygen (O2) saturation, sleep quality, and daytime symptoms deteriorate without reductions in respiratory muscle strength or vital capacity when nocturnal NIPPV is discontinued temporarily in patients with restrictive thoracic disease and improve promptly when NIPPV is resumed.35,41 Moreover, in sixteen patients with chronic respiratory failure secondary to restrictive thoracic disorders followed prospectively for 3 years after starting NIPPV, PaCO2 improved in association with an increase in the slope of the ventilatory response curve, whereas the maximal inspiratory pressure remained unchanged.43 These studies suggest that amelioration of nocturnal hypoventilation with resetting of respiratory center CO2 sensitivity and improved sleep quality may be the most important mechanisms contributing to the efficacy of long-term NIPPV. The three theories, however, are not mutually exclusive, and all could contribute more or less, depending on the patient.
Clearly, much remains to be learned regarding specific mechanisms of action of NIV. Understanding of these mechanisms is complicated by the application of NIV in both acute and chronic settings using many different techniques for patients with varying etiologies of respiratory failure. The ability to unload respiratory muscles appears to be key, particularly in the acute setting. Mechanisms controlling upper airway responses and respiratory center adaptations are less well understood but appear to be critical to success in the long-term setting.
Epidemiology of Noninvasive Positive-Pressure Ventilation
Acute care applications of NIPPV are increasing in Europe and North America.44,45 An observational study of NIV utilization for COPD and cardiogenic pulmonary edema patients in acute respiratory failure in a single twenty-six-bed French ICU revealed an increase from 20% of ventilator initiations in 1994 to nearly 90% in 2001.45 In association with this increase, the occurrence of health care–acquired pneumonias and ICU mortality fell from 20% and 21% to 8% and 7%, respectively. In an Italian study examining outcomes of NIPPV in two different time periods during the 1990s, success rates remained steady despite an increase in acuity of illness scores, suggesting that sicker patients in the later time period were being managed as successfully as less ill patients in the earlier period. Both groups of authors speculated that increased experience and skill of the caregivers was responsible for the increased use and improved outcomes.44,45
Sequential surveys of European (mainly French) ICUs demonstrated an increase in the use of NIV as a percentage of total initiations of ventilations from 16% in 1997 to 23% in 2002, with utilization in patients with COPD and cardiogenic pulmonary edema increasing from 50% to 66% and from 38% to 47%, respectively.46 Esteban et al conducted a worldwide survey in more than twenty countries that compared the trends of mechanical ventilation use and demographics between 1998 and 2004, enrolling more than 1600 patients and showing an increase in NIPPV use from 4.4% to 11.1%47 The differences in rates between the French ICU survey and the worldwide survey may reflect lower utilization rates in some countries as well as the differing methodologies between the two surveys. The French survey examined use in terms of incidents whereas the worldwide survey focused on prevalence of use. Considering that NIPPV is used for shorter periods of time on average than invasive ventilation, prevalence will accordingly be lower.
Some hospital units lend themselves well to NIPPV applications and have very high utilizations rates. In Italy, Confalonieri et al48 reported high utilization rates of NIV in specialized respiratory intensive care units, which are similar to “intermediate” or “step-down” units in the United States, where a large proportion of patients have COPD either as an etiology of acute respiratory failure or as a comorbidity. In that setting, 425 of 586 (72.5%) patients requiring mechanical ventilation were treated initially with NIV (374 using NIPPV and fifty-one using an “iron lung”).48
In a 2003 national audit of COPD exacerbations in the United Kingdom, however, NIV was unavailable in nineteen of 233 hospitals and 39% of ICUs, 36% of “high-dependency units,” and 34% of hospital wards.49 Similar results were seen in a North American survey of use of NIV in seventy-one hospitals in Massachusetts and Rhode Island.50 Overall use of NIPPV was estimated to be 20% of total ventilator initiations, but 30% of hospitals had estimated rates of less than 15%. Reasons for low utilization were mostly attributed to lack of physician knowledge of NIPPV, inadequate equipment, and lack of staff training. Most disturbingly, estimated use of NIV for COPD exacerbations and cardiogenic pulmonary edema was only 29% and 39% of ventilator initiations, respectively.50 A follow-up study in Massachusetts using data collected prospectively from 2005 to 2007 revealed an overall 38.7% NIV utilization rate, with 80% and 69% of COPD and cardiogenic pulmonary edema patients, respectively, receiving NIV as the initial mode.51 More recently, clear evidence for the dramatic increase in NIPPV use derived from a Nationwide Inpatient Survey constituting more than 7 million hospital admissions from 1998 to 2008. NIPPV use increased from 1% to 4.5% of total admissions while there was a concomitant fall in invasive mechanical ventilation from 6% to 3.5%. Mortality rates improved in most groups, but the authors raised concerns about a small subgroup of patients who were transitioned from initial NIPPV to invasive ventilation and had a 29% mortality, higher than in patients who were treated with invasive ventilation from the start.52
A national survey of U.S. Veterans Affairs hospitals showed that despite wide availability of NIV, its perceived use was low.53 Almost two-thirds of respiratory therapists responding to the survey thought that NIV was used less than half of the time when its use was indicated. The survey also revealed that wide variations in the perception of NIV use was dependant partly on the size of the ICUs, with larger ones reporting more frequent use.53 Along these lines, a Canadian study reported that between 1998 and 2003, only 66% of patients meeting criteria for NIPPV actually received it.54
Suboptimal utilization has been reported in non-Western countries as well. A Korean survey reported that NIV was used in just two of twenty-four university hospitals and comprised only 4% of ventilator initiations. A majority of the physician staff (62%) and 42% of the nurses expressed a desire for additional educational programs on NIV.55 In an Indian survey of 648 physicians, perceived NIV use was mostly limited to the ICU (68.4%), and COPD was the most common indication for its use.56 Findings of this survey were similar to those of the Korean, European, and North American surveys in that rates of NIV use varied widely between centers, with a substantial portion reporting low rates. Thus, although overall use of NIV is clearly increasing, these findings underline the need for NIV educational programs at individual hospitals that permit caregivers to develop the requisite expertise in administering NIV.
Noninvasive Positive-Pressure Ventilation in the Acute Care Setting
Numerous acute applications of NIPPV have been described, but only a few are supported by strong evidence (Table 18-1). The following sections discuss important applications according to the type of respiratory failure.
| References | |
|---|---|
| A. Strong Evidence—Recommended | |
| Exacerbation of COPD | 17, 59 to 64, 66 to 70 |
| Acute cardiogenic pulmonary edema | 104 to 126 |
| Immunocompromised (hematologic malignancy, bone marrow or solid-organ transplantation, AIDS) | 140 to 144 |
| Facilitation of weaning/extubation patients with COPD | 168 to 180 |
| B. Intermediate Evidence—Guideline | |
| Asthma | 66 to 83 |
| Community-acquired pneumonia in patients with COPD | 134 |
| Extubation failure in patients with COPD | 175, 177 to 180 |
| Hypoxemic respiratory failure | 96 to 100 |
| Do-not-intubate patients (COPD and CHF) | 150 to 157 |
| Postoperative respiratory failure (lung resection, bariatric, CABG) | 158 to 167 |
| C. Weaker Evidence—Optional | |
| Acute respiratory distress syndrome (ARDS) with single-organ involvement | 144 to 147 |
| Community-acquired pneumonia (non-COPD) | 135 to 140 |
| Cystic fibrosis | 84 to 86 |
| Facilitation of weaning/extubation failure (non-COPD) | 174, 176 |
| Neuromuscular disease/chest wall deformity | 79, 83, 84 |
| Obstructive sleep apnea/obesity hypoventilation | 88, 89 |
| Trauma | 148, 149 |
| Upper airway obstruction | |
| D. Not Recommended | |
| Acute deterioration in end-stage interstitial pulmonary fibrosis | 94, 95 |
| Severe ARDS with multiple organ dysfunction | |
| Postoperative upper airway or esophageal surgery | |
| Upper airway obstruction with high risk for occlusion |
Patients with exacerbations of COPD usually are good candidates for NIPPV because they respond to partial ventilator support, hypoxemia is usually mild to moderate, and the condition is most often reversible within a few days. Thus numerous earlier uncontrolled studies have reported that NIPPV avoids intubation in patients with COPD, with success rates ranging from 58% to 93%. Some studies have reported the use of CPAP alone to treat acute exacerbations of COPD,57,58 based on the rationale that by counterbalancing auto-PEEP, it will reduce the work of breathing.59 In these studies, relatively low levels of nasal CPAP (5 to 9.3 cm H2O) were associated with improvements in PaCO2 and arterial oxygen tension (PaO2), and few patients required intubation. The lack of controls, however, renders these studies inconclusive.
Kramer et al60 randomized thirty-one patients with various etiologies for respiratory failure, twenty-one of whom had COPD, to receive NIPPV or conventional therapy. Among COPD patients who received NIPPV in their study, respiratory rate and PaCO2 fell more rapidly during the first hour of therapy than among controls, and intubation rates were reduced to 9% compared with 67% in controls. In a multicenter European trial17 of eighty-five patients with COPD randomized to receive face-mask pressure-support ventilation (PSV) or conventional therapy, respiratory rate but not PaCO2 fell significantly in the NIPPV group during the first hour; intubation (26% vs. 74%), complication (16% vs. 48%), and mortality (9% vs. 29%) rates and hospital lengths of stay (35 vs. 23 days) all were significantly lower in the NIPPV than in the control group.
Another randomized, controlled trial compared the efficacy of standard medical therapy with NIPPV in thirty patients with acute hypercapnic respiratory failure caused by exacerbations, pneumonia, or congestive heart failure.61 Those randomized to NIPPV had greater improvements in pH and respiratory rate within 6 hours, higher success rate (93%), and shorter hospital lengths of stay (11.7 vs. 14.6 days, p < 0.05) than controls. The largest study to date on NIPPV for exacerbations of COPD randomized 236 patients to receive NIPPV or standard therapy at fourteen British centers.62 NIPPV was administered in general respiratory wards by nurses who had a few hours of in-service training with the technique. Patients treated with NIPPV had lower intubation (15% vs. 27%) and mortality (10% vs. 20%) rates than controls, but the benefit was seen only in patients with pH values of 7.3 or greater. The authors concluded that although NIPPV proved to be effective in their study, these sicker patients probably should have been treated in an ICU.
In addition to the favorable findings regarding the use of NIPPV for acute exacerbations of COPD, some studies have found that 1-year survival rates are better and the need for rehospitalization and consumption of ICU beds over the next year are less for patients treated with NIPPV as opposed to conventional therapy.63,64 Although these latter studies were not randomized, so the results could have reflected a selection bias favoring less ill patients in the NIPPV group, it is also possible that NIPPV avoids late complications of invasive ventilation, such as sustained muscle weakness or swallowing dysfunction.10
Among the many controlled and uncontrolled studies examining the efficacy of NIPPV in exacerbations of COPD, only two have obtained unfavorable results. In one,65 twenty-five of forty-nine consecutive COPD patients with acute exacerbations were treated with nasal NIPPV, and twenty-four were intolerant and served as the “control” group. Blood gases in both groups improved at similar rates, and no differences in outcome were apparent between the two groups. In the second, Barbe et al66 randomized twenty-four patients with acute exacerbations of COPD to receive nasal NIPPV or standard therapy. Four of fourteen patients randomized to NIPPV were intolerant; among the remaining patients, blood-gas improvements and hospital lengths of stay were similar, and no differences in intubation or mortality rates were apparent, leading the authors to conclude that NIPPV is ineffective in COPD. Both studies, however, enrolled consecutive patients who, on average, had less-severe blood-gas abnormalities than patients enrolled in favorable studies; none of the patients in the study of Barbe et al66 required intubation, as did almost three-quarters of the controls in the studies of Kramer et al60 and Brochard et al.17 These observations support the contention that the patients in the two unfavorable studies were less ill than those in the favorable studies, and argue that NIPPV should be reserved for sicker patients with COPD who are at risk of requiring intubation.
Multiple randomized, controlled trials lend themselves to meta-analysis. An earlier meta-analysis by Keenan et al67 concluded that NIPPV significantly reduces mortality and reduces the cost of hospitalization by an average of $3244 (Canadian) compared with conventional therapy. Peter et al68 examined both COPD and non-COPD causes of acute respiratory failure in their meta-analysis, and concluded that NIPPV significantly reduces the need for intubation as well as mortality. Meta-analyses by Keenan et al69 and Lightowler et al70 (Cochrane analysis) observed absolute and relative risk reductions of 28% and 0.42 for intubation, 10% and 0.41 for mortality, and 4.57 and 3.21 hospital days, respectively (all p < 0.05) (Fig. 18-1). The analysis of Keenan et al also concluded that there is little evidence to support NIPPV use in milder COPD, although they analyzed only two studies of mild patients. The analysis of Lightowler et al also found that PaCO2, heart rate, and dyspnea scores improved more rapidly than in conventionally treated patients. A more recent metaanalysis by Quon et al71 derived similar findings, observing reductions of 65% in intubations, 55% in mortality, and 1.9 days in hospital length of stay among COPD patients admitted with exacerbations and treated with NIPPV. These studies lend strong support to the use of NIPPV for patients with COPD in the acute care setting, leading consensus groups to recommend that the modality “be considered” in selected patients,72 and the Canadian Thoracic Society Guideline committee to recommend that NIV be considered the ventilatory modality of first choice for patients with acute respiratory failure secondary to exacerbations of COPD.73 The need for careful patient selection cannot be overemphasized (see “Selection Guidelines” below). NIPPV is best used to avoid intubation, not to replace it. Although NIPPV should be viewed as the ventilator therapy of first choice for appropriate COPD patients, those with contraindications to NIPPV should be intubated and ventilated without delay.
Figure 18-1
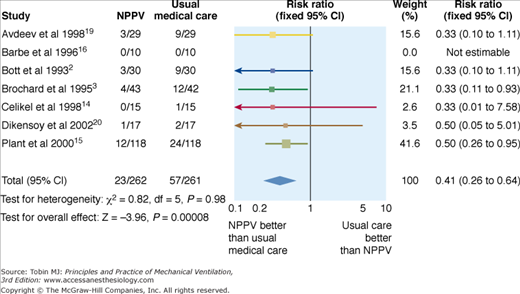
Forest plot of eight randomized, controlled studies on NPPV in patients with acute respiratory failure secondary to COPD. The reduction in mortality rate was consistent among studies. (Used, with permission, from Lightowler. Noninvasive positive pressure ventilation to treat respiratory failure resulting from exacerbations of chronic obstructive pulmonary disease: Cochrane systematic review and meta-analysis. Br Med J. 185–189, 2003.)
In view of the idea that NIPPV is best used to avoid intubation, Squadrone et al74 asked whether it can serve as an alternative to intubation in patients with COPD and advanced acute hypercapnic respiratory failure (pH ≤ 7.25, PaCO2 ≥ 70 mm Hg, respiratory rate ≥ 35 breaths/min). Sixty-four such patients had similar mortality rates and hospital lengths of stay but fewer serious complications (mainly infectious) and a trend toward a higher weaning rate at 30 days compared with a historically matched control group of invasively ventilated patients. The authors concluded that NIPPV can be used as an alternative to invasive mechanical ventilation in severely ill patients with COPD, but considering that the failure rate approached two-thirds in the NIPPV group and that the more recent report by Chandra et al52 raised concerns about this approach, NIPPV should be applied with great caution in such patients. As pointed out previously, the use of historical controls is a serious design limitation that may favor the treatment group.
Few data provide guidance on selecting patients who might benefit from continued use of NIPPV after hospital discharge. In an uncontrolled retrospective study, Tuggey et al75 found that patients treated with NIV during their acute admissions and sent home with it had many fewer hospital days per year (25 vs. 78 days; p = 0.004) and incurred much lower costs per year ($7407 vs. $23,065) after starting domiciliary NIV than before. Despite the small number of patients and uncontrolled design, these results support the idea that domiciliary NIV should be considered in “revolving-door patients” who require repeated hospital admissions and highlight the need for more definitive studies addressing this question.
Although acute asthma would be anticipated to respond favorably to NIPPV because it shares pathophysiologic features with COPD, much less evidence supports this application. One early report described seventeen patients with asthma who had an average initial pH of 7.25, a PaCO2 of 65 mm Hg, and were treated with face-mask PSV.76 Only two required intubation (for increasing PaCO2), average duration of ventilation was 16 hours, and no complications occurred.
More recently, Fernandez et al77 reported on fifty-eight patients with status asthmaticus, thirty-three of whom were retrospectively deemed candidates for NIPPV because of persisting CO2 retention (PaCO2 > 50 mm Hg) and because they met other clinical criteria.77 Of these, eleven were intubated according to clinician preference, and twenty-two were managed noninvasively. The noninvasively and invasively treated groups had similar initial PaCO2 values, which improved less rapidly in the noninvasive group. Only 14% of the NIPPV-treated patients eventually required intubation, and they had shorter ICU and hospital lengths of stay than the intubated group. Thus far, four randomized, controlled trials have been reported. Holley et al78 were able to enroll only one-tenth of the roughly 350 patients their power analysis had projected. Not surprisingly, their major outcome variable—intubation rate—was not reduced significantly in their NIPPV group (one of nineteen versus two of sixteen in controls), and they observed no deaths. Their major finding was that physicians who a priori believed that NIPPV was effective were less likely to enroll patients in the trial because of concern that the patients might require intubation if randomized to the control group. Soroksky et al79 randomized thirty-three patients with severe acute asthma (average initial forced expiratory volume in 1 second [FEV1] roughly 33%) to receive NIPPV or sham therapy via a face mask. The NIPPV group had a significantly greater increase in FEV1 within the first hour (53.5% vs. 28.5%) and fewer hospitalizations (three of seventeen versus ten of sixteen) compared with the sham group. Both groups received aerosolized bronchodilators via a nebulizer, not the ventilator. The authors speculated that the greater improvement in airflow in the NIPPV group might be related to a bronchodilator effect of positive-pressure.
The third randomized trial80 supports the notion that NIPPV may have an initial bronchodilator effect in acute asthma. In this study, forty-four patients with status asthmaticus (mean FEV1 33% predicted) received “low” NIPPV (inspiratory and expiratory pressure 6 and 4 cm H2O, respectively), “high” NIPPV (inspiratory and expiratory pressure 8 and 6 cm H2O, respectively), or oxygen supplementation in controls. For the first hour, they received hydrocortisone but no bronchodilators. After the initial hour, the “high” NIPPV group had an improvement in FEV1 over baseline of 20%, compared to no improvement in controls (P < 0.05).
In the fourth trial,81 undoubtedly underpowered, fifty-three patients with severe asthma were randomized to NIPPV (inspiratory pressure 12 cm H2O, expiratory pressure 5 cm H2O) plus standard therapy or standard therapy alone. The NIPPV group spent less time in the ICU and used less bronchodilation, but no other significant differences were observed, including rate of improvement in FEV1 or gas exchange, or rate of intubation.
These studies suggest that NIPPV may be effective at improving airflow, correcting gas-exchange abnormalities, avoiding intubation, and reducing the need for hospitalization in patients with acute severe asthma. Published studies, however, are either uncontrolled or underpowered or the findings have not been replicated. A Cochrane analysis concluded that evidence for use of NIPPV for acute asthma was “very promising” but “controversial” and that more controlled studies are needed.82 Furthermore, medical therapy alone may be quite effective.83 Lacking more evidence, no firm conclusions can be drawn regarding the relative effectiveness of NIPPV versus conventional therapy in exacerbations of asthma. The British Thoracic Society Standards of Care Committee opined that NIPPV should not be used routinely for acute asthma.84 Nonetheless, an empiric trial of NIPPV might be considered in patients not responding promptly to standard medical therapy if selected according to commonly used criteria (see “Selection Guidelines” below). Also, more research into the role of positive-pressure in enhancing acute bronchodilation seems warranted.
NIPPV has been used to treat acutely deteriorating patients with end-stage cystic fibrosis. In one study, six patients with FEV1 ranging from 350 to 800 mL and severe acute-on-chronic CO2 retention (initial PaCO2 ranging from 63 to 112 mm Hg) were treated with NIPPV for periods of 3 to 36 days; four survived until a heart-lung transplantation could be performed.84 The same investigators reported more recently on 113 patients with cystic fibrosis treated with NIPPV for acute deteriorations.85 Ninety of these patients (median FEV1/FVC ratio of 0.5) were listed for lung transplantation, twenty-eight survived to transplantation, ten remained on the list at the time of reporting, and the remainder expired. NIPPV improved hypoxia but not hypercapnia. These case series suggest that NIPPV may serve as a rescue therapy to provide a “bridge to transplantation” for patients with acutely deteriorating cystic fibrosis, but control of airway secretions is still a big challenge and mortality is high if the wait for an organ is prolonged beyond a few months.86
The inappropriate use of NIPPV in patients with tight, fixed upper airway obstruction should be avoided so as not to delay the institution of definitive therapy. In my experience, however, NIPPV can be used to treat patients with reversible upper airway obstruction, such as that caused by glottic edema following extubation, sometimes in combination with aerosolized medication and/or helium–oxygen gas mixture. Although no controlled trials demonstrate the efficacy of this approach in adults, a controlled trial in ten infants with respiratory failure showed that NIPPV87 and CPAP were equally efficacious in lowering respiratory rate, but NIPPV contributed to patient–ventilator asynchrony. If used, NIPPV should be administered cautiously and monitored closely because these patients are at risk for precipitous deteriorations.
Patients with acute-on-chronic respiratory failure caused by sleep apnea syndrome, often in combination with obesity hypoventilation, have been treated successfully with NIPPV and transitioned to CPAP once stabilized,88 but no controlled trials have evaluated this application. Sturani et al89 described the successful use of nasal NIPPV administered with the biphasic intermittent positive airway pressure (BiPAP) device (18 cm H2O inspiratory and 6 cm H2O expiratory pressures) in five morbidly obese patients (mean body mass index of 50 kg/m2) with severe sleep apnea. Anecdotally, high inflation pressures, sometimes necessitating use of volume-limited ventilators that have greater pressure-generating capabilities than portable pressure-limited ventilators, may be needed because of high respiratory system impedance.
Although NIPPV to treat patients with chronic respiratory failure secondary to restrictive thoracic diseases is well accepted (see “Chronic Respiratory Failure” above), it is used for only a small portion of patients admitted to acute care hospitals with respiratory failure. Accordingly, few studies on the management of acute respiratory failure in these patients have been reported. Small uncontrolled series have reported success using NIPPV to alleviate gas-exchange abnormalities and to avoid intubation in patients with acute respiratory failure secondary to neuromuscular disease90 and kyphoscoliosis.91 Despite the lack of evidence, the British Thoracic Society Standards of Care Committee considers that NIPPV “is indicated” in patients with acute or acute-on-chronic respiratory failure secondary to restrictive thoracic diseases.92
A regimen for managing acute deteriorations in patients with chronic respiratory failure secondary to neuromuscular disease, reported by Bach et al,93 requires that patients receive NIV at home 24 hours a day during the exacerbation. When O2 saturation falls below 90% as determined by continuous pulse oximetry, airway secretions are removed aggressively using manually assisted coughing and mechanical aids such as the cough insufflator–exsufflator until O2 saturation returns to the 90% range. In this small series of patients, the need for hospitalization was reduced dramatically after institution of the regimen.79
Limited information is available on NIPPV therapy for patients with acutely deteriorating restrictive lung diseases such as idiopathic pulmonary fibrosis. Such patients usually fare poorly with mechanical ventilation.94 On the other hand, in a recent retrospective cohort of eleven patients with idiopathic pulmonary fibrosis and acute respiratory failure treated with NIPPV,95 five survived the hospitalization and lived for more than 3 months. Thus, some such patients could be considered for NIPPV if they have a possible reversible superimposed condition and are otherwise good NIPPV candidates.
Hypoxemic respiratory failure is defined as a PCO2/FIO2 ratio of less than 200 and a respiratory rate greater than 35 breaths/min; contributing diagnoses include acute pneumonia, acute pulmonary edema, acute respiratory distress syndrome (ARDS), and trauma.96 It is an extremely broad category of acute respiratory failure. Hence, perhaps not surprisingly, studies of NIPPV to treat it have yielded conflicting results. Meduri et al97 were the first to report the successful application of NIPPV in such patients. In a randomized trial,98 the same authors found no benefit of NIPPV over conventional therapy among all entered patients. Initial hypercapnia predicted a favorable outcome: Patients with an initial PaCO2 of greater than 45 mm Hg had significantly lower intubation and ICU mortality rates and shorter ICU lengths of stay than normocapnic patients. The authors concluded that hypoxemic respiratory failure without CO2 retention responds poorly to NIPPV.
Conversely, Antonelli et al96 randomized sixty-four patients with hypoxemic respiratory failure to NIPPV or immediate intubation. Improvements in oxygenation were similar in the two groups, and only 31% of the NIPPV-treated patients required intubation. NIPPV-treated patients had significantly fewer septic complications such as pneumonia or sinusitis (3% vs. 31%), and there were trends toward decreased mortality and ICU length of stay (27% vs. 45% and 9 vs. 15 days, respectively) compared with intubated controls. Another randomized, controlled trial of sixty-one patients with various forms of acute respiratory failure found a significantly reduced intubation rate when patients with acute hypoxemic respiratory failure were treated with NIPPV as opposed to conventional therapy (7.5 vs. 22.6 intubations per 100 ICU days); mortality rates, however, were not significantly different.99
More recently, Ferrer et al100 randomized patients with severe hypoxemia (defined as a PCO2 of less than 60 mm Hg or an arterial oxygen saturation [SaO2] of less than 90% on 50% FIO2 for at least 6 to 8 hours) to receive NIPPV or conventional therapy. Intubation rate was decreased from 52% to 25%, the incidence of septic shock was reduced, and both ICU (39% vs. 18%) and 90-day mortality were lower in the NIPPV group than in controls. In contrast to some previous studies, substantial benefit was observed in patients with severe pneumonia, whereas patients with cardiogenic pulmonary edema had no reduction in intubation rate.
The favorable results of these latter studies might be interpreted to show broad support for the use of NIPPV in patients with hypoxemic respiratory failure. In fact, a recent survey of European pulmonologists and anesthesiologists showed that 48% (more pulmonologists than anesthesiologists) considered acute hypoxemic respiratory failure as a preferred indication for NIPPV.101 A systematic review, however, noted that although intubations in patients with acute hypoxemic respiratory failure seem to be reduced by NIPPV, the heterogeneity between studies precluded any firm conclusions and recommended against the routine use of NIPPV in these patients.102 Also, when overall results are favorable in a heterogeneous group of patients, it cannot be assumed that each subgroup benefits equally. It is possible that harm to a particular subgroup could be obscured by benefit in other subgroups. The following subsections examine evidence regarding the use of NIPPV in specific subgroups of patients with acute hypoxemic respiratory failure that may be more appropriate to apply to individual patients.
CPAP, although not a form of mechanical ventilatory assistance per se, was described as a treatment for acute pulmonary edema dating back to the 1930s.103 Over the past 15 years, a number of studies have demonstrated that CPAP (10 to 12.5 cm H2O) is effective in treating acute pulmonary edema. Rasanen et al194 randomized forty patients with cardiogenic pulmonary edema to either face-mask CPAP or standard medical therapy, and demonstrated that CPAP more rapidly improves oxygenation and respiratory rate. In a study of fifty-five patients with pulmonary edema, Lin and Chang105 found that those randomized to face-mask CPAP (adjusted to maintain a PaO2 of 80 mm Hg or greater) had a lower intubation rate (17.5% vs. 42.5%, p < 0.05) than conventionally treated controls. Bersten et al106 and Lin et al92 subsequently performed randomized studies on thirty-nine and 100 patients, respectively, demonstrating more rapid improvements in respiratory rates and oxygenation and a reduced need for intubation in patients treated with CPAP. The study of Bersten et al106 also showed a significant reduction in the length of ICU stay among CPAP-treated patients, and the study of Lin et al107 showed a trend for a lower hospital mortality rate. The average absolute reduction in intubation rate among these studies was 28% (from 47% in controls to 19% for CPAP). These studies provide strong evidence to support the use of CPAP to treat acute cardiogenic edema.
As discussed earlier, the combination of increased inspiratory pressure and positive expiratory pressure (i.e., pressure support plus PEEP or NIPPV) might be expected to reduce work of breathing more effectively than CPAP alone, bringing about more rapid relief of dyspnea and improvement in gas exchange. Thus, more recent studies have focused on the use of NIPPV to treat acute cardiogenic pulmonary edema. One prospective, uncontrolled study found that face-mask PSV improved pulse oximetry, pH, and PaCO2 within 30 minutes in twenty-nine patients with acute pulmonary edema, only one of whom required intubation.108 A second prospective, uncontrolled study109 reported similar effects on gas exchange, but five of twenty-six patients required intubation, and successfully treated patients had higher PaCO2 (54 vs. 32 mm Hg) and lower creatine phosphokinase levels (176 vs. 1282 IU) (both p < 0.05) than failure. Furthermore, four patients died in the first study and five in the second, three and four, respectively, with myocardial infarctions. The authors concluded that NIPPV is a “highly effective technique.” The accompanying editorialist, however, cautioned about applying NIPPV to patients with acute myocardial infarctions.110
Several randomized, controlled trials have been performed subsequently comparing NIPPV with conventional O2 therapy to treat patients with acute cardiogenic pulmonary edema. Masip et al111 found that inspiratory and expiratory pressures of 15 and 5 cm H2O, respectively, lowered the intubation rate from 33% in eighteen controls to 5% among twenty-two patients randomized to NIPPV (p = 0.037). NIPPV also improved oxygenation more rapidly, but hospital lengths of stay and mortality rates were similar in the two groups. Sharon et al112 randomized forty patients to receive NIPPV plus low- or high-dose nitroglycerin. The NIPPV group had higher rates of intubation (80% vs. 20%), myocardial infarction (55% vs. 10%), and death (10% vs. none) compared with the nitroglycerin controls (all p < 0.05), leading the authors to conclude that NIPPV was less effective and potentially harmful compared with high-dose nitroglycerin. This inference, however, is suspect because the treatments were not comparable, and the inordinately high intubation rate in the NIPPV group (80%) is difficult to explain. In a larger study, Nava et al113 randomized 130 patients with acute pulmonary edema to receive NIPPV (average: 14.5 cm H2O of pressure support and 6.1 cm H2O of PEEP) or O2 therapy; hypercapnic and normocapnic patients were prospectively distributed equally between groups. As in the earlier studies, NIPPV improved oxygenation, respiratory rate, and dyspnea more rapidly than conventional therapy, but mortality and hospital lengths of stay did not differ between the groups. Overall, the rates of intubation were not significantly different (25% in controls vs. 20% for NIPPV); in the hypercapnic subgroup, however, the intubation rate was lower in the NIPPV group than in controls (6% vs. 29%, p = 0.015). These studies suggest that NIPPV is effective therapy for acute pulmonary edema, but whether this is true only for hypercapnic patients awaits further evaluation.
The question of whether NIPPV (the combination of pressure support and PEEP) is superior to CPAP alone is important because CPAP can be delivered more simply and less expensively. An earlier randomized trial comparing the two to treat acute pulmonary edema showed significantly more rapid reductions in respiratory rate, dyspnea scores, and hypercapnia in the NIPPV group compared with the CPAP-treated group.114 The study was stopped prematurely after enrollment of twenty-seven patients, however, because of a greater myocardial infarction rate in the NIPPV group (71% vs. 31% in controls). This difference may have been attributable to unequal randomization because more patients in the NIPPV group presented with chest pain. The results nonetheless raise concerns about the safety of ventilator techniques used to treat acute pulmonary edema.
More recent randomized, controlled trials comparing NIPPV with CPAP have not detected differences in the myocardial infarction rate. Crane et al115 randomized sixty patients with cardiogenic pulmonary edema to three different therapies: conventional, CPAP (10 cm H2O), or bilevel ventilation (15 cm H2O inspiratory and 5 cm H2O expiratory pressures). Treatment success was 15% in the control group, 35% in the CPAP group, and 45% in the bilevel group (p = 116). Although myocardial infarction rate did not differ among the groups, hospital mortality was 30% in the control group, 0% in the CPAP group, and 25% in the bilevel group (p = 0.029). The difference in mortality was not statistically significant until after the first week of hospitalization, after patients had stopped using the devices.
Several additional studies have randomized patients with acute cardiogenic pulmonary edema to CPAP or noninvasive PSV plus PEEP and have found no differences in myocardial infarction rates.116,119 Physiologic variables improved equally in both groups, intubation and mortality rates were similar, and troponin I levels and the speed of clinical resolution were nearly identical. In addition to finding no increase in the myocardial infarction rate in NIV-treated patients, these latter studies also found no clear advantage of NIPPV over CPAP alone. These findings must be interpreted with caution, however, because patients with myocardial infarction or acute ischemia were excluded.
In the largest study reported to date, Gray et al120 randomized 1069 patients with cardiogenic edema to receive CPAP (5 cm H2O) alone, NIPPV (inspiratory and expiratory pressures 8 and 4 cm H2O, respectively) or oxygen plus routine therapy in controls. No differences were noted between the CPAP and NIPPV groups, so they were combined in the analysis. Although dyspnea and pH improved more rapidly in the positive-pressure groups than in controls, no differences were apparent in intubation or mortality rates. The authors concluded that noninvasive positive-pressure treatment of cardiogenic pulmonary edema was useful to alleviate symptoms, but not to improve other outcomes. The very low intubation rate in this study (roughly 3% in all groups), however, was much lower than in most previous studies despite the use of low positive-pressures, suggesting that the patients had relatively mild respiratory compromise. Thus, the study may not be comparable to the earlier studies showing significant avoidance of intubations or even mortality.
A number of meta-analyses121–126 have concluded that CPAP alone is effective in reducing dyspnea, improving vital signs and gas exchange, and reducing intubation and mortality rates, without any significant effect on myocardial infarction rates. Similar benefits have been attributed to NIPPV, except that improved mortality has been found in only a few,124–126 probably because there have been fewer studies of NIPPV than on CPAP. These meta-analyses have also compared NIPPV and CPAP, finding no differences between the two modalities with respect to intubation and mortality rates as well as occurrence of myocardial infarction. These findings have held up, even when meta-analyses were performed after publication of the Gray study.125,126
Deciding which patients with acute cardiogenic pulmonary edema should receive NIPPV can be challenging because they may respond rapidly to conventional therapy. Using their single-center registry, Masip et al127 obtained data on eighty conventionally treated patients with cardiogenic pulmonary edema to identify those at risk for intubation. Patients with a pH of less than 7.25 or hypercapnia and a systolic blood pressure of less than 180 mm Hg were found to be at high risk. The authors recommended that such patients should be “promptly considered” for NIV. Because studies have not shown definitively that NIV is more effective than CPAP, however, the most sensible current recommendation is to use CPAP (10 cm H2O) initially, and consider switching to NIPPV if the patient has unrelenting dyspnea or persisting tachypnea or hypercapnia. Furthermore, either CPAP or NIPPV should be used with great caution, if at all, in patients with acute myocardial infarction or active ischemia. These recommendations are in line with those of a Cochrane analysis that deemed NIV, especially CPAP, as “safe and effective” for the treatment of cardiogenic pulmonary edema in adults.128
An important trend in the application of CPAP for acute cardiogenic pulmonary edema has been the use in the field by ambulance crews to treat patients before hospitalization. The experience with this practice has been favorable thus far. Plaisance et al129 observed a strong trend for reduced intubation and mortality rates among 124 patients with cardiogenic pulmonary edema randomized to “early” (started immediately on site) versus “late” (delayed by 15 minutes) CPAP (7.5 cm H2O). In another randomized, controlled trial, Thompson et al130 observed an absolute reduction of 30% in intubation rate (seventeen of thirty-four patients [50%] vs. seven of thirty-five [20%]) and absolute mortality fell by 21% among patients with cardiogenic pulmonary edema treated with CPAP compared to usual therapy with oxygen, including intubation and bag-valve-mask-ventilation if needed.
A pilot study by Duchateau et al131 reported an improved respiratory status in twelve “do not intubate” patients when offered NIPPV out-of-hospital by emergency medical services. Respiratory rate decreased from 34 to 27 breaths/min (p = 0.009) and pulse oximetry improved from 86% to 94% (p < 0.01) with only one intolerant patient. These studies suggest that outcomes of patients with cardiogenic pulmonary edema can be improved by very early initiation of noninvasive positive-pressure therapy in the field and adoption of this as a routine practice for emergency medical services seems likely. A recent Cochrane analysis concluded that prehospital NIV “appears to be a safe and feasible therapy” that may lower the need for intubation compared to initiation in the emergency department.132 The authors of the Cochrane analysis cautioned, however, that the evidence is preliminary and that cost-effectiveness analyses have not been performed.
An earlier retrospective study found that acute severe pneumonia is a predictor of NIV failure, perhaps because NIPPV does little to facilitate the clearance of secretions.133 Confalonieri et al134 randomized fifty-six patients with severe community-acquired pneumonia to receive NIPPV or standard O2 therapy. The NIPPV group had fewer intubations (21% vs. 50%) and shorter ICU lengths of stay (1.8 vs. 6 days) than controls (both p < 0.05). In addition, NIPPV-treated patients with COPD had significantly better survival at 2 months, thought to be related to fewer late complications of intubation. The most important observation, though, was that all the benefit was attributable to the subgroup with COPD, and no clear benefit of NIPPV was seen in patients without COPD patients. More recently, a prospective study on NIPPV to treat patients with severe community-acquired pneumonia but without COPD found that oxygenation and respiratory rates improved initially in twenty-two of twenty-four patients after starting NIPPV, but 66% eventually required intubation.135 Based on the preceding evidence, initiation of NIPPV is justifiable in appropriate patients with pneumonia and COPD. The benefit of NIPPV in patients with pneumonia but without COPD has not been established. As such, NIPPV should be used selectively and with caution in such patients.
The severe acute respiratory syndrome epidemic was characterized by a high rate of respiratory failure among afflicted individuals, many of whom were otherwise healthy health care workers. Initially, use of NIPPV was discouraged because of concerns about aerosolization and transmission of the highly contagious coronavirus to other health care workers. Two retrospective studies, however, one from Beijing on twenty-eight patients treated with NIPPV139 and the other from Hong Kong on twenty patients,140 suggest that NIPPV is effective in avoiding intubation in some patients. Intubation was required in only 33% and 30% of NIPPV-treated patients in the two studies, respectively. Stringent infection-control measures, including the use of a face mask, an inline viral/bacterial filter in the bilevel ventilator tubing, and a high-efficiency particulate accumulator mask by all health care workers having contact with the patients, prevented transmission of severe acute respiratory syndrome to any caregivers. Both studies reported high rates of barotraumas, 22% and 20%, respectively; it was unclear that this was related to NIPPV. Given the lack of controls, these studies cannot be used to assess the efficacy of NIPPV in severe acute respiratory syndrome, although the lack of transmission to health care workers should allay fears about NIPPV spreading the virus so long as stringent isolation and prevention measures are employed.
More recently, the use of NIPPV to treat influenza pneumonia during the H1N1 epidemic was controversial.138 Based on the 1 m dispersion of aerosol beyond the mask demonstrated during NIPPV applied to a human-like mannequin,139 some advised against use of NIPPV for influenza pneumonia, although actual transmission by this route was never demonstrated, nor was it compared to dispersion occurring during invasive mechanical ventilation or even spontaneous breathing.
The use of NIPPV to avoid endotracheal intubation in immunocompromised patients is appealing because, by assisting ventilation without having to invade the airway, it reduces infectious and hemorrhagic complications. Encouraging results derived from an uncontrolled series that reported NIPPV success rates as high as 67% (in forty-eight patients with AIDS and Pneumocystis carinii pneumonia).140 Conti et al141 avoided intubation in fifteen of sixteen patients treated with NIPPV with acute respiratory failure complicating hematologic malignancies, although patients were excluded if they had more than two organ-system failures or were responding poorly to antineoplastic therapy. More recently, Antonelli et al142 randomized forty patients with acute respiratory failure of various etiologies following solid-organ transplantation to receive NIPPV or standard therapy. NIPPV reduced the need for intubation and lowered ICU mortality rate (both 20% vs. 50% in controls, p < 0.05), but total hospital mortality was similar. Trends for fewer health care–associated pneumonias and episodes of severe sepsis also were apparent among NIPPV-treated patients. In a subsequent study of fifty-two immunocompromised patients with respiratory failure, 58% with hematologic malignancies, randomized to receive NIPPV for at least 2 hours three times daily or standard O2 therapy, those treated with NIPPV had fewer intubations (46% vs. 77%) and mortalities (50% vs. 81%, both p < 0.05).143
The sizable reductions in mortality among these high-risk patients strongly supports the use of NIV as the ventilatory modality of first choice in selected immunocompromised patients with acute respiratory failure. Patients developing respiratory insufficiency should be started on NIPPV relatively early,133 before progression to severe respiratory failure, watched closely, and intubated without delay if needed. The need to perform invasive diagnostic procedures sometimes requires intubation in these patients although NIPPV can be used to support patients during fiber-optic bronchoscopy (see below).
The use of NIPPV to treat ARDS has been controversial, some considering it the “last frontier.” One early cohort series reported that NIPPV maintained adequate oxygenation and averted intubation in six of twelve episodes of ARDS in ten patients.144 In an observational cohort of seventy-nine patients with acute lung injury, Rana et al145 found that shock, metabolic acidosis, and profound hypoxemia were predictors of NIV failure and cautioned against use in such patients. A more recent study used NIPPV as a “first-line” therapy of ARDS.146 Of 479 patients presenting with ARDS, 147 had not been intubated upon admission to the ICU. These were begun on NIPPV and 54% avoided intubation. Not unexpectedly, outcomes were much better in those who avoided intubation than in those who failed NIPPV and required intubation: 2% versus 20% rate of ventilator-associated pneumonia and 6% versus 53% mortality rate, respectively. A simplified acute physiology score of equal to or less than 34 at baseline and a PaO2/FIO2 greater than 175 after the first hour of NIPPV predicted success. Although not controlled, the trial suggests that a small minority (15% in this trial) of patients with ARDS can be managed successfully with NIPPV, but they must be chosen carefully and monitored very closely in an ICU. If their oxygenation fails to improve substantially within the first hour, urgent intubation should be considered.
Recently, a randomized controlled trial of NIPPV in patients with acute lung injury (200 > PaO2/FIO2 < 300 showed reductions in the need for intubation one of twenty on NIPPV pts and seven of 19 control patients) and actual intubations (one of twenty-one versus four of nineteen) as well as occurrence of organ failure (three of twenty-one versus fourteen of nineteen) (all p < 0.05), with a trend toward reduced mortality.147 These studies suggest that NIPPV may have a role in the management of some patients with acute lung injury and ARDS, but it should be avoided in those with multiorgan system failure and very severe oxygenation defects who are likely to require prolonged ventilator support using sophisticated modes. If a trial of NIPPV is initiated, patients should be intubated without undue delay if they deteriorate or even fail to improve sufficiently.
Traumatic chest wall injuries such as flail chest or mild acute lung injury might respond favorably to NIPPV, but other etiologies might not. In a retrospective survey on forty-six trauma patients with respiratory insufficiency treated with NIPPV, Beltrame et al148 found rapid improvements in gas exchange and a 72% success rate, but burn patients responded poorly. More recently, a controlled trial that randomized thoracic trauma patients with PaO2/FIO2 < 200 to NIPPV or high-flow oxygen was stopped early after enrollment of fifty patients because of significant reductions in intubation rate (12% vs. 40%) and hospital length of stay (14 vs. 21 days) in the NIPPV group.149 These results support the use of NIPPV for hypoxemic respiratory failure in postthoracic trauma cases, but it is well to remember that these were carefully selected patients.
Noninvasive Positive-Pressure Ventilation for Categories of Patients with Acute Respiratory Failure
Some argue that there is little to lose by using NIPPV in almost any terminal patient. NIPPV could be used to lessen dyspnea, preserve patient autonomy, and permit verbal communication with loved ones during a terminal patient’s final hours.150 Some patients might be salvaged in the near term who otherwise would die without ventilatory assistance. This application is controversial, however, with some arguing that it could merely prolong the dying process, diminish patients’ comfort in their waning hours, and promote excessive resource utilization.151
Among reports on NIPPV to treat patients who have declined or are reluctant to undergo intubation, Benhamou et al152 retrospectively studied thirty such patients, mostly elderly men (mean age: 76 years) with COPD. Despite severe respiratory failure (mean PAO2 of 43 mm Hg and PaCO2 of 75 mm Hg), NIPPV was successful initially in 60% of patients. The authors considered NIPPV to be preferable to endotracheal intubation because short-term prognosis was better, and the modality appeared to be more comfortable with fewer complications. In another uncontrolled series, Meduri et al153 observed a similar response to NIPPV among twenty-six patients with acute hypercapnic and hypoxemic respiratory failure who refused intubation.
In a prospective survey of 113 do-not-intubate patients treated with NIV,154 amounting to 10% of all patients treated with NIPPV, survival to hospital discharge was 72% and 52% for patients with acute pulmonary edema and COPD, respectively, whereas it was less than 25% for patients with pneumonia or cancer. In addition, the absence of an effective cough and the inability to be awakened were significantly associated with hospital mortality. Similar findings were reported by Schettino et al.15 Thus, the use of NIV may be justifiable in do-not-intubate patients who have a high likelihood of surviving the hospitalization. Longer-term survival of these hospital survivors, however, is poor; Chu et al156 found a 30% 1-year survival for do-not-intubate patients with COPD as compared with 65% for patients desiring intubation. Also, no studies have yet assessed effects on patient comfort or family satisfaction.
NIV can also be used for palliation in patients whose prognosis is poor for surviving an admission to hospital, with the possible aims of alleviating dyspnea or prolonging survival long enough to enable a patient time to settle affairs or say goodbye to loved ones. As recommended by a consensus statement by a task force of the Society of Critical Care Medicine on NIV,157 it is necessary for the patient, family, and caregivers to agree on these goals and to cease NIPPV promptly if it seems to be adding to suffering (via mask discomfort, for example) rather than alleviating it.
Several early case series on the use of NIPPV to treat respiratory insufficiency in postoperative patients with PaCO2 values of greater than 50 mm Hg, PAO2 values of less than 60 mm Hg, or evidence of respiratory muscle fatigue reported prompt reductions in respiratory rate and dyspnea scores, improvement in gas exchange, and high success rates (roughly 75%) in avoiding the need for reintubation.158,159 Subsequent studies found that NIPPV was more effective than CPAP or chest physiotherapy in improving lung mechanics and oxygenation after coronary artery bypass surgery,160 and better than O2 therapy alone in improving oxygenation after lung-resection surgery.161 NIPPV also ameliorated postgastroplasty pulmonary dysfunction in morbidly obese patients.162
These earlier studies heightened interest in the prophylactic use of CPAP or NIPPV after high-risk surgeries such as major abdominal surgery162–165 or thoracoabdominal aneurysm repair.166 These studies, using CPAP (10 cm H2O) for 24 hours postoperation, observed reductions in the incidence of hypoxemia, pneumonia, atelectasis, and intubations compared with standard treatment.
Few studies have examined the postoperative role of NIPPV in patients with frank respiratory failure, but a randomized trial of NIPPV in forty-eight post–lung-resection patients with acute respiratory insufficiency, most with COPD, showed significant improvements in oxygenation and reductions in the need for intubation (21% vs. 50%) and mortality rate (13% vs. 38%) compared with conventionally treated controls (both p < 0.05).167
These studies strongly support the idea that both CPAP and NIPPV should be considered to prevent and treat postoperative respiratory complications and failure, especially in high-risk surgeries, but only a few studies have examined each of the various surgeries and positive-pressure techniques possible, so more specific recommendations cannot currently be made.
Nava et al168 tested the hypothesis that NIPPV could be used to shorten the duration of invasive ventilation and reduce the occurrence of associated complications in a randomized, controlled trial of fifty patients intubated for acute respiratory failure secondary to COPD. If they failed a T-piece weaning trial performed 48 hours after intubation, patients were randomized to extubation followed by face-mask PSV or continued intubation and routine weaning. The NIPPV patients had higher overall weaning rates (88% vs. 68%), shorter durations of mechanical ventilation (10.2 vs. 16.6 days), briefer stays in the ICU (15.1 vs. 24 days), and improved 60-day survival rates (92% vs. 72%) (NIPPV-treated versus controls, all p < 0.05). In addition, no NIPPV-treated patients had nosocomial pneumonia compared with seven pneumonias among the controls. In a similar trial, Girault et al169 randomized thirty-three patients with acute-on-chronic respiratory failure to remain intubated or to be extubated to NIPPV after failure of a 2-hour T-piece trial. The NIPPV group had a shorter duration of endotracheal intubation (4.6 vs. 7.7 days, p = 0.004), but the total duration of mechanical ventilation was longer in the NIPPV group, and weaning and mortality rates and ICU and hospital lengths of stay were similar between the groups.
More recently, Ferrer et al170 randomized forty-three patients with “persistent” weaning failure (three consecutive failed T-piece trials) to be extubated to NIV or to remain intubated and be weaned using conventional methods. Patients randomized to NIV had shorter periods of intubation (9.5 vs. 20.1 days), shorter ICU (14 vs. 25 days) and hospital stays (14.6 vs. 40.8 days), a lower rate of nosocomial pneumonia (24% vs. 59%), and improved ICU and 90-day survivals (roughly 80% vs. 50%, all p < 0.05). This study lends strong support to the use of NIV to facilitate extubation, but it is worth noting that two-thirds of the patients had COPD or congestive heart failure.
In the most recent randomized (VENISE) trial that included 208 patients who had failed a spontaneous breathing trial, 69% of whom had COPD, the investigators included not only invasively ventilated and NIV groups, but also a group extubated early to oxygen therapy alone.171 There were no differences in the main outcome variable: reintubation within 7 days (around one-third of patients in each group), or in most secondary outcome variables including mortality and lengths of stay in the ICU and hospital, complications and need for tracheostomy. Duration of intubation, however, was 1.5 days longer in the invasively ventilated group by design and the rate of postextubation acute respiratory failure was significantly less in the NIV group because NIV rescue was used after extubation in 57% and 45% of the oxygen therapy and invasively ventilated patients (p > 0.05), respectively, with an overall NIV rescue success rate of 52%. The authors concluded that, based on the reduction in postextubation acute respiratory failure, their results should “support the implementation of NIV” in difficult-to-wean patients, but recommended further study.
Thus, overall, the evidence favors the use of NIPPV to facilitate weaning and extubation in difficult-to-wean patients with COPD, mainly to reduce the occurrence of postextubation respiratory failure. In the absence of overwhelmingly favorable evidence, however, the following caveats should be borne in mind: (a) This approach should be reserved mainly for patients with COPD; (b) patients should be selected carefully, ascertaining that they are good candidates for NIPPV (see “Selection Guidelines” below); (c) patients should not have been difficult intubations; and (d) patients should be comfortable on levels of PSV that can used via mask after extubation.
Another potential application of NIPPV in the weaning process is to avoid reintubation in patients who fail extubation. Epstein et al172 reported that extubation failure is associated with much higher morbidity and mortality rates (43%) than successful extubations (approximately 10%). Some investigators have used NIPPV prophylactically to see if extubation failure can be avoided. Jiang at al173 randomized consecutive extubated patients to receive NIPPV or conventional therapy and found a trend for a higher reintubation rate in the NIPPV group (28% vs. 15%), suggesting that indiscriminate use of NIPPV is not effective for preventing extubation failure. Other investigators have attempted to prevent extubation failure by initiating NIPPV when patients develop risk factors for extubation failure. Esteban et al174 tried this approach in a multicenter, multinational randomized trial of 221 patients developing risk factors for respiratory failure within 48 hours after they were extubated, including hypercapnia, tachypnea, or hypoxemia. Reintubation rates (48%) and ICU lengths of stay (18 days) were identical in both groups, and the study was terminated prematurely because of a significantly increased ICU mortality in the NIV group (25% vs. 15%, p = 0.048). The mortality difference was attributable to a higher mortality in the reintubated NIV patients, reintubation occurring almost 10 hours later than in the standard-therapy group. The authors concluded that NIV is not effective in unselected patients at risk for extubation failure and speculated that the greater delay in reintubation was responsible for the higher mortality rate. It is worth noting, however, that twenty-eight patients in the control group crossed over to NIPPV when they met failure criteria. Thus, the controls likely would have had a substantially higher reintubation rate had they not crossed over to NIPPV. Also, only 10% of patients enrolled in the study had COPD.
Another approach to treating extubation failure is to await the development of overt respiratory failure before initiating NIPPV. Hilbert et al175 found that NIPPV used in this fashion lowered reintubation rate (20% vs. 67%) and shortened ICU lengths of stay in thirty patients with COPD and postextubation hypercapnic respiratory insufficiency compared with thirty historically matched controls. Keenan et al176 randomized eighty-one patients to receive NIPPV or conventional therapy if they developed respiratory failure within 48 hours of extubation. The reintubation rate in this trial was roughly 70% in both the NIPPV group and controls, and no significant differences were found in hospital length of stay or survival. Patients with COPD, however, were excluded after the first year for ethical reasons, and only 12% of the patients had COPD. Furthermore, the pressures used (10 cm H2O inspiratory and 5 cm H2O expiratory) may have been insufficient to provide adequate ventilatory assistance.
Two subsequent randomized trials (consisting of ninety-seven and 162 patients, respectively,177,178 approximately 30% to 40% of whom had COPD or congestive heart failure [CHF]) enrolled patients deemed to be at “high risk” for extubation failure. Both studies found that NIV reduced the need for reintubation, ICU mortality, and hospital length of stay, but hospital mortality was decreased only in the hypercapnic subgroup of the second study.178 A more recent randomized trial of 106 patients with postextubation hypercapnia (PaCO2 > 45 mm Hg) showed a significant reduction in postextubation respiratory failure as well as 90-day mortality in the group randomized to NIPPV compared to oxygen-treated controls.179 The main effect of NIPPV in this study was to prevent greater retention of CO2. The reason for the reduced 90-day mortality when mortality was not significantly reduced at earlier time points was not apparent.
These more recent studies support the use of NIV for patients who are at “high risk” for extubation failure, particularly if they have COPD, CHF, and/or hypercapnia. A Cochrane systematic review concluded that for patients who mainly have COPD, the evidence “demonstrated a consistent, positive effect on mortality and ventilator-associated pneumonia.”180 Based on the Esteban study,174 however, NIPPV to prevent extubation failure should be used very cautiously in at-risk patients who do not have COPD or other favorable characteristics because of the higher risk of NIPPV failure and its attendant morbidity and mortality. Such patients failing to improve promptly with NIPPV should be reintubated without delay.
Use of NIPPV in the pediatric population has been increasingly reported in the medical literature,181 but most studies are retrospective and very few randomized controlled trials have been performed. For more detailed assessments of this literature, the reader is referred elsewhere.181,182 Pediatric applications of NIPPV parallel those in the adult, but the etiologies of respiratory failure, of course, reflect those encountered in children. In earlier reports, Fortenberry et al183 found that respiratory rate, PaCO2, and oxygenation improved promptly after initiation of nasal bilevel NIPPV in a retrospective series of twenty-eight children with acute hypoxemic respiratory failure, only three of whom required intubation. Padman et al184 subsequently reported similar results in a prospective series of thirty-four pediatric patients with both hypoxemic and hypoventilatory respiratory insufficiency, again with only three patients requiring intubation. More recent applications have been reported in children with status asthmaticus185 and atelectasis186 and randomized, controlled trials have been performed in children with bronchiolitis187 and tracheomalacia.188 These studies consistently show more rapid improvements in vital signs and gas exchange with NIPPV compared to controls.
These favorable responses to NIPPV in children are not surprising, particularly when they are suffering from conditions reported to be treated successfully by NIPPV in adults. Concerns have been raised, however, about treating very young children and infants with NIPPV because of increased nasal resistance189 and inability to cooperate.182 In the series of Fortenberry et al183 of twenty-eight patients, NIPPV was successful in avoiding intubation in the ten children who were younger than 5 years of age. More recently, a retrospective trial observed successful application of NIPPV in infants following liver transplantation.190 In a randomized, prospective trial on infants (median age: 9.5 months) with various causes of upper airway obstruction, CPAP and BiPAP proved to be equally efficacious in reducing respiratory rate and breathing effort; both were well tolerated, although BiPAP was associated with more asynchrony.188 The lack of controlled trials makes it difficult to formulate specific guidelines for NIPPV in children, although reported success rates appear to be comparable to those in adults, and tentative guidelines have been proposed182 that are based on those used for adults.
Noninvasive Ventilation for Patients Undergoing Procedures
NIPPV administered via T connector attached to a face mask can be used to assist ventilation and enhance oxygenation during fiber-optic bronchoscopy in high-risk patients. First reported to improve oxygenation and be well tolerated in a small series of immunocompromised hypoxemic patients, NIPPV was shown subsequently to improve and sustain oxygenation better than conventional O2 supplementation in a randomized, prospective trial in twenty-six patients with PaO2/FIO2 ratios of 200 or less and suspected nosocomial pneumonia.191 More recently, NIPPV to assist ventilation during fiber-optic bronchoscopy was administered successfully using a “helmet” device (see techniques section below).192 NIPPV also has been used to assist ventilation during upper endoscopy for gastric tube placement in patients with neuromuscular disease193 and during performance of transesophageal echocardiography.194
NIPPV can be used to improve O2 saturation during and after intubation and decrease the incidence of O2 desaturations below 80% during intubation according to a randomized trial in critically ill patients with hypoxemic respiratory failure.195 This approach is promising but needs further evaluation before routine use can be recommended. This also begs the question whether, if NIV improves oxygenation substantially, intubation could be avoided in some of these patients.
Selection of Patients for Noninvasive Positive-Pressure Ventilation in the Acute Care Setting
Retrospective133,196 and prospective197–199 studies have identified predictors of NIPPV success (Table 18-2). Patients with baseline hypercapnia fare better than those with hypoxemia alone, but successful patients have lower baseline PaCO2 values (79 vs. 98 mm Hg) and higher pH values (7.28 vs. 7.22) than failure patients.105 Pneumonia predisposes to failure whether alone or in combination with COPD (odds ratio [OR] 5.63 for COPD).197,199 The strongest predictor of success, though, is prompt improvement in gas exchange and heart and respiratory rates within 1 to 2 hours of NIPPV initiation.133,196–199 Confalonieri et al198 have incorporated some of these predictors (Acute Physiology and Chronic Health Evaluation [APACHE] II score ≥ 29, pH < 7.25, Glasgow Coma Score ≤ 11, and respiratory rate ≥ 35 breaths/min) into two risk charts for NIPPV failure, one to be used at baseline and the other at 2 hours (Fig. 18-2). If these abnormalities were all present at baseline, the likelihood of failure was 82% and rose to 99% if they persisted at 2 hours.
| Younger age |
| Lower activity of illness (APACHE score) |
| Able to cooperate, better neurologic score |
| Able to coordinate breathing with ventilator |
| Less air leaking, intact dentition |
| Tachypnea, but not excessively rapid (> 24 but < 35 breaths/min) |
| Hypercarbia, but not too severe (PaCO2 > 45 but < 92 mm Hg) |
| Acidemia, but not too severe (pH < 7.35 but > 7.10) |
| Improvements in gas exchange, heart and respiratory rates within first 2 hours* |
Figure 18-2
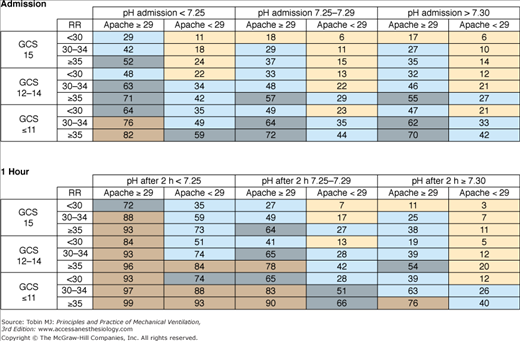
Charts showing percentage likelihood of noninvasive positive-pressure ventilation (NIPPV) failure in patients with chronic obstructive pulmonary disease (COPD) based on pH and Acute Physiology and Chronic Health Evaluation (APACHE) score and Glasgow coma score (GCS). Chart on top refers to values at the time of admission, and bottom chart is at 2 hours. Numbers in boxes are percentages for likelihood of failure. At 2 hours, the combination of an APACHE score of less than 11, APACHE score of 29 or greater, and a Glasgow coma score of less than 11 predicts failure with a likelihood of 99%. Based on 1033 patients with COPD treated with NIPPV in thirteen different experienced units. (Used, with permission, from Antonelli, et al. Predictors of failure of noninvasive positive pressure ventilation in patients with acute hypoxemic respiratory failure: a multi-center study. Intensive Care Med. 2001;27:1718–1728. With kind permission from Springer Science and Business Media.)
Timing of initiation is another determinant of success. Ambrosino et al133 advised that NIPPV “should be instituted early in every patient before a severe acidosis ensues.” Initiation of NIPPV should be viewed as taking advantage of a “window of opportunity.” The window opens when acute respiratory distress occurs and shuts when the patient deteriorates to the point of necessitating immediate intubation. In this context, it should be emphasized that NIPPV is used as a way of preventing intubation, not replacing it.
The preceding predictors of success and failure and the entry criteria used for enrollment of patients into the many studies have served as a basis for consensus guidelines on the selection of patients to receive NIPPV for acute respiratory failure.200 These guidelines use a simple three-step approach outlined in Table 18-3. The first step asks whether the patient needs ventilator assistance. Patients with mild or no respiratory distress are excluded from consideration because they should do well without ventilator assistance. Those needing ventilator assistance are identified using clinical indicators of acute respiratory distress and gas-exchange derangement, as listed in Table 18-3. These criteria are most applicable to patients with COPD but can be used to screen those with other forms of expiratory failure, although some modifications are advisable. For example, studies on NIPPV in acute pulmonary edema and acute hypoxemic respiratory failure have used higher respiratory rates as enrollment criteria (> 30 to 35 instead of > 24 breaths/min) and a PCO2/FIO2 ratio of less than 200.111–114
|
The second step is to screen out patients in whom use of NIPPV is contraindicated (see Table 18-3). Most are relative contraindications, and judgment should be exercised in implementing them. Also, some conditions that have been listed as contraindications in the past no longer preclude the use of NIPPV. For example, patients with coma, if related to hypercapnia, may be managed successfully with NIPPV. Diaz et al201 demonstrated that patients (mainly with COPD) with hypercapnic coma (Glasgow coma scores ≤ 8) had outcomes just as good as those with higher Glasgow coma scores. In another report,152 nearly half the patients were obtunded or somnolent initially, yet most were managed successfully with NIPPV.
The underlying etiology and potential reversibility of acute respiratory failure are also important considerations in patient selection. As discussed previously, the strongest evidence supports the use of NIPPV for COPD and either NIPPV or CPAP for acute cardiogenic pulmonary edema. As illustrated in Figure 18-3, a reversible etiology permits the use of NIPPV as a “crutch” that assists the patient through a critical interval, allowing time for other therapies such as bronchodilators, steroids, or diuretics to reverse the underlying condition. More severe, less easily reversed forms of respiratory failure that will require prolonged periods of ventilatory support, such as status asthmaticus requiring controlled hypoventilation, complicated pneumonias, or ARDS, are best managed using invasive ventilation. Marginal patients might be considered for a trial of NIPPV but should be watched closely for further deterioration so that needed intubation is not delayed unduly.
Figure 18-3
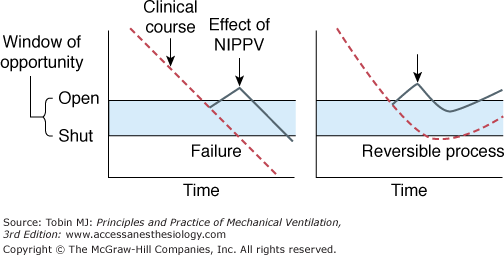
Schema to illustrate importance of reversibility in success of noninvasive positive-pressure ventilation (NIPPV) for acute respiratory failure. Left: Relentless downhill clinical course of underlying process (severe acute respiratory distress syndrome). NIPPV initiated when window of opportunity opens still fails because it is not sufficient to support the patient when the underlying process has progressed too far. Right: NIPPV succeeds when medical therapy reverses the underlying process (chronic obstructive pulmonary disease exacerbation).
Noninvasive Positive-Pressure Ventilation for Chronic Respiratory Failure
Restrictive thoracic disorders limit expansion of the thoracic cage either because of increased elastance (as with chest wall deformity), muscle weakness (as with neuromuscular diseases), or both. Experience gained during the polio epidemics of the 1930s through 1950s and subsequently with other neuromuscular disorders demonstrated that “body ventilators,” even when used intermittently, were effective at stabilizing or even reversing chronic respiratory failure secondary to restrictive thoracic disorders.202,203
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


