Fig. 25.1
The first baboon-to-human liver xenotransplantation recipient painted by Sir Roy Calne (with the generous permission of Sir Roy Calne)
Proliferation Stage
In the following 16 years, liver transplantation became a manageable procedure in most major medical centers. Hepatectomy is performed using venovenous bypass, piggyback technique, or simple cross-clamping technique depending on surgeon’s preference and anatomy of the patient. Organ allocation practice became more objective by utilizing medical ESLD score (MELD) and pediatric ESLD score (PELD), developed by Wiesner et al. in 2001 [27]. This scoring system, derived from serum creatinine level, international normalization ratio of prothrombin time, and serum bilirubin, predicts the probability of death in patients with ESLD, and has been accepted as an organ allocation guide by the United Network of Organ Sharing (UNOS). The number of living-donor liver transplantation and small bowel transplantation increased dramatically during this period. Rejection is more controllable with the introduction of newer immunosuppressants (basiliximab, sirolimus, and mycophenolate mofetil) as an induction agent or adjunct to cyclosporine or tacrolimus.
Anesthesiology and Perioperative Care
Experimental Stage
Dr. Jorge Antonio Aldrete was the first anesthesiologist involved in the care of most, if not all, patients at the University of Colorado (Fig. 25.2). He was praised by Starzl as a premier anesthesiologist who “could keep stones alive” and “one of few anesthesiologists who had the skills or determination to handle these difficult cases.” His contribution to liver transplantation was extraordinary, although understanding of physiologic care was limited at that time: arterial blood gas analysis was not readily available, and pulmonary artery catheterization was introduced in the 1970s. Aldrete et al. described their clinical experience in liver transplantation in detail [28, 29]. Awake intubation or “crash” induction was used in patients with full stomach, and thiopental and succinylcholine were used in patients with presumably empty stomach. Fluoroxene and nitrous oxide were maintenance agents, and non-depolarizing agents (d-tubo curare or pancuronium) were used for muscle relaxation. Intraoperative monitoring consists of blood pressure, heart rate, central venous pressure, and body temperature. They observed arterial hypotension in practically all patients. Massive blood transfusion was required by many patients (50–350 ml/kg), and blood was replaced based on blood pressure, central venous pressure, and hematocrit values. They noted potential myocardial depression and acidosis associated with transfusion-induced citrate intoxication, metabolic acidosis after hepatectomy, reperfusion hypotension, hypothermia, and altered electrolyte and acid-base balance. They published several more important articles investigating dynamics of body temperature, lidocaine clearance, serum electrolytes, and choline esterase [30–33].
Fig. 25.2
Photos with Dr. Jorge Antonio Aldrete in 1999 at the fifth International Transplantation Society Congress (Pittsburgh, PA). From the left, Andre De wolf (Northwestern University), Jorge Antonio Aldrete, William Merritt (John Hopkins University), and Yoogoo Kang (University of Pittsburgh)
On one weekend, Aldrete and Andres Zahler Mayanz, another anesthesiologist, climbed to a mountain to study high-altitude respiratory physiology. On way back home, Mayanz was involved in fatal car accident and became the first physician organ donor in 1968. After his contribution to liver transplantation, Aldrete developed postanesthesia recovery score [34] and is enjoying his pain management practice in Florida.
At the same period, Pappas et al. published their investigation on hemodynamic alterations during liver transplantation in six patients using dye dilution technique to measure cardiac output [35]. They observed a reduction in cardiac index (by 39 %), stroke volume index, and mean arterial pressure (by 18 %), and a rise in peripheral vascular resistance (by 71 %) during the anhepatic stage.
John Farman and Michael Lindop led the liver transplantation anesthesia and intensive care unit at Cambridge, and published their experience of 25 liver transplantations in 1974 [36]. In their report, main anesthetics were nitrous oxide, narcotics, and muscle relaxants. Monitoring consists of ECG, arterial pressure, central venous pressure, and analysis of arterial blood gas and electrolytes. They also observed severe hypotension during the anhepatic stage and on reperfusion of the grafted liver, and reperfusion hyperkalemia. They encountered a significant mortality: two intraoperative deaths (one by excessive bleeding, and another one possibly by air embolism), one by cardiac arrest, one by septic shock, and three by irreversible hemorrhage. Dr. Dagmar Schaps led the anesthesia group in the Hannover program and published her experience in liver transplantation in 1978 [37].
During this period, clinical hemostatic defects were intensively investigated. Von Kaulla, a German hematologist, investigated coagulation using coagulation profiles and thromboelastography (TEG) [38]. They observed a profound defect in coagulation. In a 3-year-old child, uncontrollable bleeding was followed by severe fibrinolysis, which was reversed by the administration of ɛ-aminocaproic acid (EACA , 0.1 g/kg). In the second patient, severe fibrinolysis was reversed by EACA. Postoperatively, however, he became thrombophilic and died of multiple arterial thrombosis and pulmonary emboli. In the third patient, fibrinolysis was treated by EACA. Two hours later, he became hypercoagulable, and died of pulmonary embolism in 2 days after surgery. In the fourth patient, fibrinolysis was normalized spontaneously, but he died of pulmonary embolism in the sixth postoperative day. The coagulation defect was not remarkable in the fifth patient, but she died of liver necrosis in the postoperative 23rd day. They suggested that pathologic fibrinolysis was a common occurrence, and it might be caused by anoxia which activated the plasmin-plasminogen system. Additionally, they suggested that the provision of a well-functioning homograft for the anhepatic recipients led to a very rapid correction of the clotting defects. Groth et al. made a similar observation in 1969 [39]. They suggested that moderate bleeding should not be regarded with alarm nor treated pharmacologically since spontaneous improvement can be expected. Further, avoidance of pharmacologic manipulation of hemostasis and omission of an external venous bypass might be helpful in preventing postoperative thromboembolism.
Development Stage
During this period, anesthesia and perioperative care were developed in several centers, namely University of Pittsburgh, Cambridge and King’s College of London, University of Minnesota, University of Hannover, and Hospital Cochin of Paris.
At the University of Pittsburgh, the beginning of the liver transplantation program was extremely challenging: Anesthesia care of patients for liver transplantation was relatively unknown at that time, and patients were cared for by the anesthesiologist on call, which diluted the clinical experience of liver transplantation. At the same time, infrastructure of the medical center required a learning period to adapt to the new surgical procedure. Specifically, the need for massive blood transfusion was a major challenge: It was technically difficult, and management of its complications was a daunting task.
In the beginning of 1983, anesthesiologists of the University of Pittsburgh developed a liver transplantation anesthesiology group, and their objective was to develop a patient care guideline through clinical research. John Sassano, a cardiac anesthesiologist, developed a rapid infusion system with a specific goal of delivering up to 1.5 L of fluid per minute in a controlled fashion while maintaining normothermia (Fig. 25.3) [40]. His ingenious invention utilized readily available various parts. A cardiotomy reservoir (3 L) was attached to a roller pump of a cardiac bypass machine to deliver premixed blood in a rapid rate. A heat exchanger was incorporated to minimize hypothermia associated with massive transfusion. An air bubble detector from a hemodialysis machine was added to avoid accidental air delivery, and all disposable items were assembled at the hospital. This rapid infusion system helped most patients to avoid hypovolemia during liver transplantation as well as patients undergoing cardiac procedures and trauma surgery. The commercial version (Rapid Infusion System® by Haemonetics®, Braintree, MA) was adopted by many liver transplantation centers up to year 2000, and a smaller, improved version is being marketed as a Fluid Management System® (Belmont®, Watertown, MA) [41].
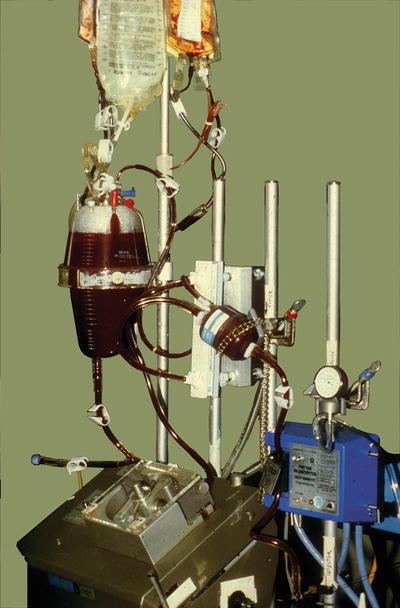
Fig. 25.3
A rapid infusion system designed by Dr. John J Sassano
Douglas Martin, an intensivist and cardiac anesthesiologist, led the research in hemodynamics and electrolyte balance using the pulmonary artery catheter and mixed venous oximetry [42]. They confirmed that the high cardiac output state was associated with low oxygen content secondary to anemia and a moderate decrease in arterial hemoglobin oxygen saturation. Oxygen delivery and oxygen consumption were relatively normal, but arterial-venous oxygen content difference (A-V DO2) was relatively low, suggesting that patients with ESLD may not be able to utilize oxygen, possibly by the loss of regional vasomotor control resulting in a maldistribution of peripheral flow. They postulated that two anatomically and probably pharmacologically distinct peripheral vascular circuits may exist in parallel; vessels with normal vasoreactivity supplying oxygen to tissues and vessels with a reduced vasoreactivity behaving as an arteriovenous shunt. They suggested that alpha agonist may increase systemic blood pressure, but may increase shunting by constricting normal nutrient vessels. Further, their studies in electrolyte and fluid balance were foundation of modern anesthesia care [43].
Citrate intoxication had been a well-recognized complication of massive transfusion in the absence of hepatic function. Jose Maquez took charge in the investigation of dynamic changes in ionized calcium level during liver transplantation [44]. The study revealed that ionized hypocalcemia develops in the early stage of liver transplantation, and ionized calcium level and serum citrate level are inversely related during the anhepatic stage. In addition, Dr. Marquez was able to demonstrate the relationship between ionized hypocalcemia and myocardial dysfunction.
Management of blood coagulation was another challenge for the new program. It was evident that patients with ESLD have bleeding tendency secondary to thrombocytopenia, generalized reduction in procoagulants, and activation of the fibrinolytic system. There were two dilemmas in coagulation management: Coagulation profile does not necessarily reflect blood coagulability in the surgical field, and replacement and pharmacologic therapy were guided by clinical impression rather than scientific facts. Yoogoo Kang, who had been in TEG research in obstetrics, reintroduced this technique in liver transplantation [45]. All patients undergoing liver transplantation were monitored by TEG and comprehensive coagulation factor assays. It should be noted that Jessica Lewis (Director, Coagulation Laboratory, University of Pittsburgh) and Franklin Bontempo (coagulation specialist, University of Pittsburgh) were very knowledgeable in TEG and eager supporters of the project. Patients were treated based on TEG findings and coagulation profiles, when available. The study in more than 80 patients demonstrated that all forms of coagulopathy develop during liver transplantation, and they are dilution, excessive activation, fibrinolysis, and heparin effect. Further, blood loss in patients with TEG monitoring was reduced by 50 % compared with that of historic controls [46], although this improvement could have been equally contributed by the use of venovenous bypass and improved anesthesia care.
Management of fibrinolysis was the next focus during this period. Kang et al. observed that severe fibrinolysis was a common occurrence, and it was readily treatable by EACA in vitro. However, EACA was not used clinically to avoid potential thrombotic complications reported by von Kaulla et al. In the first patient who received EACA, severe fibrinolysis, demonstrated on TEG, was treated easily by a small dose of EACA (1 g, IV bolus). Interestingly, the surgeon noticed that oozing stopped approximately 30 min after EACA administration. In their follow-up study, small doses of EACA (<1 g, IV) were found to be effective in treating fibrinolysis documented by a serial TEGs without thrombotic complications [47]. The mechanism of fibrinolysis was studied at the same period. Robert Porte, a medical student from the Dijkzigt university of Rotterdam, measured the level of tissue plasminogen activator (TPA) to investigate its relationship with fibrinolysis [48], and Mohamed Virji, a clinical chemist, measured the level of TPA and plasminogen activator inhibitor (PAI) to determine their role in fibrinolysis [49]. These two independent studies revealed that severe fibrinolysis is caused by an explosive increase in TPA, which overwhelms PAI on reperfusion of the grafted liver. This is followed by a gradual decrease in TPA and detectable levels of PAI as the grafted liver begins to function.
Several other drugs were tried to improve clot formation or to prevent fibrinolysis during this period. Boylan et al. demonstrated that high-dose tranexamic acid reduced blood loss and transfusion requirement by inhibiting fibrinolysis [50]. Aprotinin was introduced to liver transplantation arena by Neuhaus et al. and Mallett et al. [51, 52]. They reported that high-dose aprotinin reduced the blood loss by more than 50 % while surgical field was dry. It is noteworthy that Carl Groth suggested that aprotinin may be beneficial in treating fibrinolysis in liver transplantation in 1965. Thereafter, many European centers used aprotinin and reported improved coagulation and reduced blood transfusion requirement, although the beneficial effects of aprotinin were not clearly seen in follow-up studies. In the USA, Kang et al. showed that aprotinin inhibits coagulation by inhibiting serine esterase, and its antifibrinolytic activity is weaker than that of the equivalent dose of EACA [53]. They suggested that EACA is more specific toward plasmin and plasminogen, and more economical with less side effects compared with those of aprotinin. Aprotinin was used only in a limited number of liver transplantation centers in the USA. With the combined efforts of clinicians and scientists, blood transfusion requirement decreased from more than 50 units of red blood cells to less than 10 units in a span of 15 years (Fig. 25.4).
Fig. 25.4
Blood transfusion requirement in 50 years
Clinical application of venovenous bypass played a major role in minimizing surgical complications. Some forms of bypass or shunting techniques had been used in the 1960s, but results were disappointing owing to the need for systemic heparinization or thrombosis at the cannula site. Starzl and Byer Shaw, with the support of cardiac surgeons (Bart Griffith and Robert Hardesty), developed venovenous bypass utilizing heparinized Gott shunt tubings and Biomedicus centrifugal pump® (Medtronics®, Minneapolis, MN) without systemic heparinization [16]. This technique decompresses the portal vein and IVC by shunting the blood to the left axillary vein to minimize visceral and renal congestion. Consequently, bleeding aggravated by portal hypertension was reduced, and the anhepatic stage became more physiologic by minimizing hypovolemia.
Hypoglycemia expected to occur in patients with severe hepatocellular disease, particularly during the anhepatic stage. However, it was not a clinical concern owing to transfusion of blood products containing dextrose solution. On the contrary, hyperglycemia was a clinical concern after reperfusion of the grafted liver. De Wolf et al. compared blood glucose level of hepatic venous blood and systemic arterial blood in dogs and concluded that reperfusion hyperglycemia was caused by the release of glucose from the hypothermically preserved donor liver via glycogenolysis [54]. Altered glucose metabolism was further investigated by Mallett et al. They observed that persistent hyperglycemia after reperfusion was caused by impaired hepatic reuptake of glucose, and is an indication of the poorly functioning graft liver [55]. Their observation continued with an investigation on hormonal control of glucose metabolism [56].
A similar progress was made in pediatric liver transplantation at the Children’s Hospital of University of Pittsburgh led by David Ryan Cook and Lawrence Borland. Their report on the clinical experience of 50 children who underwent 68 liver transplantations has been considered the standard of care of pediatric patients for many years to come [57]. During this period, Goran Klintmalm of Dallas described the role of anesthesiologists in liver transplantation. “The anesthesiologist with specialized training is as important as transplant surgeon. He/she manipulates and corrects the various homeostatic mechanisms of the recipient: blood replacement, correction of coagulation defects and fluid and electrolyte imbalances, monitoring of gas exchange, and preservation of the hemodynamic stability” [58].
Postoperative care of liver transplantation recipients at the intensive care unit underwent a major evolution. The surgical intensive care unit of the Medical Center was primitive by the current standard. Sharing a relatively small intensive care unit by all types of critically ill surgical patients posed a potential for cross-infection, and knowledge base and experience of intensivists were mostly limited to general or cardiac intensive care. Ake Grenvik, an intensivist with surgical background from Sweden, modernized the facility, developed liver intensive care unit, and established the standard for postoperative care [59].
The Central Blood Bank of Pittsburgh, which supplied blood products to 32 regional hospitals, had to make a major adjustment in terms of the need for additional man power, resources and equipment, and development of communication channel not to disrupt blood supply to liver transplantation patients. They were very successful in meeting all challenges, and no patient suffered from hypovolemia and anemia [60]. Another major issue was donor organ procurement and preservation. Mr. Donald Denny, who was the director of procurement agency in Pittsburgh, played a major role in developing the standard for organ procurement [61].
About this time, liver transplantation programs were developed in many parts of the world, and it was necessary to develop a forum of all physicians and scientists involved in liver transplantation. In 1984, anesthesiologists of the University of Pittsburgh hosted the First Symposium on Anesthesia and Perioperative Care in Liver Transplantation. Its specific goal was to present clinical experience and research results of the Pittsburgh program to help others to jump-start their programs. Dr. Starzl began his lecture on “Liver Transplantation” with the following message. “I thought from time to time how really appropriate it was for anesthesiologists to be responsible for the organization of this Symposium. The anesthesiologists are the unsung heroes in the development of liver transplantation. There comes a moment in the life of these patients in which there is a throw of the dice, and their lives fall into the hands of the anesthesiologist. The way in which this group of modern day heroes has responded has really been remarkable. I don’t think we can see that illustrated any better than over at the University of Pittsburgh where this year more than 500 liver transplantation surgeries are going to be carried out, a truly staggering total, which I would have thought was the fantasy that cannot be achieved until a few years ago.” The symposium was very successful. More than 150 physicians participated in the symposium, and they included anesthesiologists, intensivists, surgeons, hepatologists, blood bankers, coagulation specialists, immunologists, infectious disease specialists, to name a few. The symposium was a media in which multidisciplinary leaders in liver transplantation met face to face to hear experiences and research activities of others. In the anesthesiology field, they were Jorge Estrin and Kruma Belani of University of Minnesota, Steven Rettke and David Plevak of Mayo Clinic, Simon Gelman of University of Alabama, James Chapin of University of Nebraska, William Merritt of Johns Hopkins, Lennard Eleborg of Stockholm, Denise Potter of Kings College of London, and Geroge Khoury of UCLA, to name a few. The proceedings of the symposium were published as a monograph, “Hepatic Transplantation: Anesthetic and Perioperative Management,” and it has been the major textbook for the following 30 years. The second symposium held in 1986 evolved into a scientific symposium with presentation of the state-of-the-art clinical and scientific information, together with presentation of research abstracts from all liver transplantation centers. The proceedings were published in Transplantation Proceedings [1987 Aug;19(4 Suppl 3)] with a generous support of Felix Rappaport who was the Editor of the journal. In 1987, Yoogoo Kang and John Farman communicated and agreed that it was the time to develop an international society related with liver transplantation (Fig. 25.5). The Symposium transformed to the International Society of Perioperative Care in Liver Transplantation, and John Farman developed the Liver Intensive Care Group of Europe. Unfortunately, John Farman passed away shortly after the letter without seeing the one international society. The LICAGE has flourished under the leadership of Michael Lindop, Gilbert Park, and John Klinck.
Fig. 25.5
A letter from John Farman to Yoogoo Kang in 1987 regarding the formation of the International Liver Transplantation Society
At the first International Society of Perioperative Care in Liver Transplantation held in Pittsburgh, the society transformed again into the International Liver Transplantation Society. The goal of the new multidisciplinary society was to raise the standard of care for patients requiring liver transplantation and to promote education and research by disseminating and exchanging information related to liver transplantation within the medical community, as well as to the public. Many physicians who shared the noble objectives became founding members of the Society: Yoogoo Kang (President, anesthesiology), Russell Wiesner (Vice President, hepatology), William Merritt (Treasurer/Secretary, anesthesiology), and Andre De Wolf (Newsletter, anesthesiology). Founding council members were Jorge Estrin from anesthesiology, Ake Grenvik and David Plevak from critical care medicine, David Van Thiel and Michael Sorrell from hepatology, and William Wall, John Fung, and Robert Gordon from surgery. In 1995, The Society and American Association of Studies in Liver Disease jointly published “Liver Transplantation and Surgery” and Byer Shaw, Michael Sorrell, and Russell Wiesner were instrumental in launching this major joint project. The journal was renamed to “Liver Transplantation” in 2000. The Society has grown leaps and bounds and has been a focal point of liver transplantation. Fortunately, the Society has kept its original goals for the past 25 years.
Maturation Stage
During this period, clinical research continued. In the cardiovascular system, severe reperfusion hypotension leading to cardiac arrest was a major concern. Shushma Aggarwal investigated the hemodynamic changes that occur on reperfusion of the grafted liver, by measuring cardiac output using the dye dilution technique to avoid errors associated with the acute change in blood temperature on reperfusion [62]. They defined the postreperfusion syndrome (PRS) as acute hypotension (<70 % of the baseline value) lasting longer than 1 min within 5 min after reperfusion. They observed that approximately 30 % of patients developed the PRS. Patients with the PRS had lower blood pressure by the study design, more pronounced bradycardia, and lower systemic vascular resistance. Cardiac output was not different between the two groups of patients with and without the PRS, and hyperkalemia, acidosis, and hypothermia were not contributing factors for the PRS. The investigation continued to identify the role of prostaglandin on the PRS by measuring its metabolite (6-keto PGF1 alpha) and thromboxane. The level of 6-keto PGF1 alpha and its relationship with thromboxane were variable in patients with and without the PRS, suggesting that the cause of the PRS is multifactorial and elusive [63].
In 1989, Ellis et al. reported that the PRS could be caused by right-heart dysfunction based on their observation of pulmonary embolism on transesophageal echocardiography [64]. This finding suggested that the PRS could be caused by mechanical derangement in addition to chemical and physical alterations. Right ventricular function on reperfusion of the grafted liver was investigated by De Wolf et al. by determination of right ventricular ejection fraction [65]. Their results indicated that right ventricular function was relatively well preserved in uncomplicated orthotopic liver transplantation.
In the 1990s, medically challenging patients who had been ruled out of transplantation candidacy were considered candidates for liver transplantation, and they were portopulmonary hypertension and hepatopulmonary syndrome. Hughes et al. reported that vasodilator therapy in patients with portopulmonary hypertension was ineffective or unpredictable, and suggested combined heart-lung transplantation for its treatment [66]. This was followed by a successful combined liver-heart-lung transplantation by the Cambridge group in 1987 [67]. In liver transplantation arena, Prager et al. reported a patient whose pulmonary hypertension persisted after liver transplantation [68], and De Wolf et al. reported 80 % mortality, although pulmonary hypertension was normalized in one survivor [69]. They suggested that patients with normal right ventricular function may survive as long as they do not suffer from other medical or surgical complications. Nitric oxide, the most promising drug at that time, was found not to be effective in lowering pulmonary arterial pressure [70, 71]. There had been several sporadic reports on portopulmonary hypertension, but it was not until Susan Mandell of Colorado and Michael Krowka of Mayo Clinic developed a national database to include a large number of patients for a comprehensive investigation [72]. Subsequent studies demonstrated that chronic pulmonary vasodilator therapy before liver transplantation is beneficial to increase survival and improve the course of the disease [73], and many centers developed their own guideline based on published reports [74].
Related posts:
 Preoperative Evaluation and Preparation for Lung Transplantation
Anesthesia and Intraoperative Management of Renal Transplantation
Preoperative Evaluation and Preparation for Lung Transplantation
Anesthesia and Intraoperative Management of Renal Transplantation
 Intensive Care of the Deceased Multiorgan Donor: One Donor, Nine Lives
Intensive Care of the Deceased Multiorgan Donor: One Donor, Nine Lives
 Acute Liver Failure: Perioperative Management
Acute Liver Failure: Perioperative Management
 Technical Innovation and Visceral Transplantation
Postoperative Care of Heart Transplant Patients
Technical Innovation and Visceral Transplantation
Postoperative Care of Heart Transplant Patients
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


