CHAPTER 46 Intra-Aortic Balloon Pump Counterpulsation
INTRA-AORTIC BALLOON PUMP (IABP) counterpulsation has emerged as one of the most effective and most frequently employed methods of mechanical circulatory support. Specifically, it relies on the twin concept of diastolic augmentation and afterload reduction to facilitate the functioning of an ischemic and failing myocardium. This concept was originally proposed by Moulopoulos and associates in 1962; subsequently, they documented improvement in hemodynamic parameters in experimental animal models.1 The first clinical report of human use by Adrian Kantrowitz appeared 6 years later.2 During the last 4 decades, IABP has experienced a technological evolution. With the advent of a percutaneous approach to insertion, the device has been used in an expanding array of clinical settings: managing cardiogenic shock; treating persistent and intractable angina; during weaning from cardiopulmonary bypass; during thrombolytic therapy in patients at high risk for occlusive rethrombosis; during complex and high-risk coronary angioplasty; and in the setting of severe stenosis of the left main coronary arterial trunk or critical aortic stenosis before surgical intervention.3 Due to its widespread usage, practitioners in the critical care setting need to be familiar with the fundamental principles of IABP counterpulsation therapy to effectively manage cardiac patients. As evidence of its prevalent usage, one report estimates that more than 70,000 IABP devices are annually placed in the United States.4
Physiologic Principles
The IABP has two main hemodynamic effects: during the diastolic phase of the cardiac cycle, a volume of blood is displaced to the proximal aorta following inflation; during the systolic phase, a vacuum effect is created in the proximal aorta following rapid deflation, thereby reducing the afterload experienced by the contracting left ventricle. To optimize these two hemodynamic effects, the IABP must inflate and deflate in synchrony to a patient’s cardiac cycle. Since 1970, observations have revealed that the single most important determinant of effective balloon-assisted circulation is the balloon pump’s timing to the cardiac cycle.5 Once proper timing has been established, an IABP will achieve three goals: an improvement in myocardial oxygen delivery via an increase in coronary perfusion pressure; a reduction in cardiac work by a decrease in systolic blood pressure (afterload); finally, an improvement in forward blood flow in patients with impaired cardiac contractile function.6 Following technological advancements during the past three decades, modern intra-aortic balloon pumps now use a closed-loop control system to automatically optimize pump timing.7–11
The principal objective of balloon counterpulsation is to enhance the balance between myocardial oxygen consumption and supply. Several factors affect the achievement of a favorable balance: the volume of the balloon; its position in the aorta; the underlying heart rate and rhythm; the compliance of the aorta; lastly, the systemic vascular resistance.12 For instance, an increase in arterial elastance (a property which is affected by compliance) is associated with a greater degree of hemodynamic improvement from an IABP.13 Despite the presence of multiple factors that can cause variability in the effects of an IABP, a majority of patients do exhibit a specific hemodynamic profile in the setting of cardiogenic shock (Table 46-1). This profile includes the following parameters: a decrease in systolic pressure by 20%; an increase in diastolic pressure by 30%, which may subsequently enhance coronary blood flow to a territory perfused by an artery with a critical stenosis; a reduction of heart rate by less than 20%; a decrease in the mean pulmonary capillary wedge pressure by 20%; and an elevation in the cardiac output by 20%.14 The reduction in aortic pressure, which is caused by the rapid deflation of the balloon, effectively decreases left ventricular afterload, and consequently diminishes myocardial workload.6 Afterload (pressure work) is significantly more costly in terms of myocardial oxygen consumption than cardiac output (volume work).15 In fact, many authorities in this field maintain that afterload reduction is the most beneficial aspect of balloon counterpulsation on a failing left ventricle.16,17 Two indices that are measured during IABP counterpulsation include the tension-time index (TTI), which is the time integral of left ventricular pressures during systole, and the diastolic pressure-time index (DPTI), which is the time integral of the proximal aortic pressures during diastole. Proper balloon inflation augments diastolic pressure (i.e., increases DPTI) whereas rapid balloon deflation decreases left ventricular afterload (i.e., decreases TTI). A ratio can be constructed from these two indices (DPTI:TTI ratio); this ratio has been termed the endocardial-viability ratio and illustrates the relationship between myocardial oxygen supply and demand. With IABP counterpulsation optimally synchronized to a patient’s cardiac cycle, the endocardial-viability ratio will be increased.6,18
Table 46–1 Effect of Intra-aortic Counterpulsation on Hemodynamic Parameters
| Hemodynamic Parameter | Effect |
|---|---|
| Aortic systolic pressure | Decrease |
| Aortic diastolic pressure | Increase |
| Mean aortic pressure | Increase |
| Left ventricular afterload | Decrease |
| Mean pulmonary capillary wedge pressure | Decrease |
| Cardiac output | Increase |
| Left ventricular ejection fraction | Increase |
| Diastolic pressure-time index (DPTI) | Increase |
| Tension-time index (TTI) | Decrease |
| Endocardial viability ratio (DPTI/TTI) | Increase |
Data abstracted from Scheidt S, Wilner G, Mueller H, et al: Intraaortic balloon counterpulsation in cardiogenic shock. N Engl J Med 1973;288:979.
Monitoring of IABP Counterpulsation
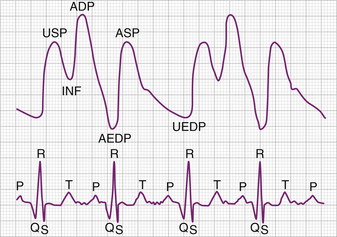
The appropriate timing of balloon counterpulsation to the mechanical events of the cardiac cycle is crucial to deriving optimal hemodynamic benefits (Fig. 46-1). To maximize diastolic augmentation, the balloon should inflate at end-systole, immediately after closure of the aortic valve. Balloon inflation augments coronary perfusion pressure, thereby providing greater myocardial oxygen delivery. Mean diastolic pressure (MDP) correlates well with coronary perfusion and hence oxygen delivery.6 Smith and colleagues confirmed the proposal that maximal coronary perfusion occurs when balloon inflation coincides with end-systole.9,19 The timing of balloon deflation, which best decreases left ventricular oxygen consumption, is less well defined. Deflation before the ventricular ejection of blood unequivocally creates a vacuum effect in the proximal aorta, which in turn reduces afterload and peak systolic pressure. The resultant net decrease in oxygen consumption is difficult to quantitate. However, peak systolic pressure is directly related to ventricular wall stress; a decrease in the latter parameter is associated with a reduction in myocardial oxygen consumption.6
The triggering of balloon counterpulsation requires the existence of a predictable, reproducible, and reliable event. The trigger marks a time point in which balloon inflation and deflation are planned. In most cases, the R wave of the surface ECG serves as the triggering event. The more sophisticated IABP systems do offer other triggering capabilities, such as arterial pressure waveforms, and ventricular or atrioventricular pacer spikes. The IABP can also function in an asynchronous pumping mode with a trigger rate set by the operator. Such a mode can be employed during cardiopulmonary resuscitation.6
Loss of optimal hemodynamic effect occurs when balloon counterpulsation is not appropriately timed to the mechanical events of a patient’s cardiac cycle. Mahaffey and colleagues have provided lucid descriptions of four different scenarios involving faulty coupling of balloon counterpulsation with the cardiac cycle.20
The two previously described scenarios dealt with inappropriate timing of balloon inflation. However, the following two scenarios involve faulty timing of balloon deflation.20
During late deflation, the balloon is deflated after the onset of systole and the opening of the aortic valve. The resultant hemodynamic profile is similar to the one observed with early inflation: afterload is increased, thereby leading to increased left ventricular work and myocardial oxygen consumption along with reduced stroke volume and cardiac output. Analysis of the arterial pressure tracing usually reveals the loss of a distinct valley representing the end-diastolic pressure before the central aortic systolic wave. To correct late deflation, the timing interval should be decreased gradually until the balloon deflates before the onset of cardiac systole.
Contraindications to the Use of IABP Counterpulsation
When intra-aortic counterpulsation therapy is being considered, the risks and benefits of this modality must be individually assessed for each patient (Table 46-2).
Table 46–2 Contraindications to Intra-aortic Balloon Pump Counterpulsation Therapy
| Absolute Contraindications | Relative Contraindications |
|---|---|
| Occlusion or severe stenosis of distal aorta | Severe peripheral vascular disease |
| Aortic aneurysm | Aortic or iliofemoral bypass grafts |
| Aortic dissection | Contraindication to intravenous anticoagulation |
| Severe aortic regurgitation | Moderate aortic regurgitationSustained tachyarrhythmias (with ventricular rate >160 beats/min) |
Data from Mahaffey KW, Kruse KR, Ohman EM: Perspective on the use of intraaortic balloon counterpulsation in the 1990s. In Topol EJ (ed): Textbook of Interventional Cardiology, Update Series, No. 21. Philadelphia, WB Saunders, 1996, pp 303-320.
Absolute Contraindications. These include the following situations: distal aortic occlusion or severe stenosis, suspected aortic dissection, documented abdominal or thoracic aortic aneurysm, and severe aortic regurgitation.21
Relative Contraindications. They are more frequent and must be taken into account when deciding to use intra-aortic counterpulsation therapy. These include the following scenarios: severe peripheral vascular disease (PVD), aortic or iliofemoral arterial grafts, a contraindication to the usage of heparin or other parenteral anticoagulation, moderate aortic regurgitation, and uncontrolled sustained tachyarrhythmias (heart rate exceeding 160 beats/min).21 Patients with vascular abnormalities such as distal aortic stenosis, aortic dissection, or aortic aneurysm have a significantly increased risk of catastrophic vascular complications. The presence of PVD or iliofemoral grafts increases the risk of complications associated with balloon insertion and removal. Aortic regurgitation can potentially lead to further cardiac decompensation. During balloon inflation, an increased regurgitant volume may be generated across the incompetent aortic valve, thereby resulting in increased left ventricular volumes. Data from animal studies have demonstrated increased regurgitant flow but also enhanced left ventricular stroke volumes, despite the increased diastolic volumes.22 Therefore, although patients with severe aortic valvular insufficiency should be excluded from IABP counterpulsation therapy, patients with lesser degrees of aortic regurgitation should be considered but with close monitoring during the initial phase of the therapy. Sustained tachyarrhythmias with heart rates exceeding 160 beats/min hamper the ability of the balloon drive system to accurately track the mechanical events of the cardiac cycle and provide hemodynamic support. A cardiac electrophysiologic evaluation can be considered before implementation of intra-aortic counterpulsation therapy in such patients.20
Insertion, Removal, Maintenance, and Complications
Placement of the IABP Is the First Step for Counterpulsation Therapy
The percutaneous route via cannulation of the femoral artery is most often employed. Once it is concluded that the patient no longer requires circulatory support, the removal of the IABP is also a straightforward process. Mahaffey and colleagues have devised a simple stepwise approach to device insertion and removal (see Appendix A).20
A thorough vascular physical examination should precede the insertion of the IABP. This examination should include palpation of all lower extremity pulses along with auscultation of the lower half of the abdomen and of the femoral arteries. The femoral artery with the best palpable pulsation should be selected to minimize any vascular complications.3 Early single-lumen balloons were inserted via a femoral artery cutdown or a large (11F) sheath. Newly available balloons (7.5F) are inserted percutaneously over a guidewire using a smaller sheath (8F to 9F) or sheathless. The downsizing of IABP catheters and sheathless insertion has significantly reduced the incidence of ischemic peripheral vascular complications, especially in patients with small or atherosclerotic arteries. In patients with severe peripheral atherosclerosis or distal abdominal aortic aneurysms, the IABP can be inserted through the axillary or the brachial arteries.
No conclusive data support the need for intravenous anticoagulation in the setting of IABP use. A trial involving 153 patients found no difference in vascular complications or laboratory end points in patients undergoing intra-aortic counterpulsation therapy, with and without continuous heparin anticoagulation.23 Industry guidelines do not require continuous anticoagulation therapy, especially when the device is set in a 1:1 assist ratio. Currently, it is reasonable to use intravenous heparin with the goal of maintaining an aPTT of 60 to 75 seconds in a patient without contraindications to anticoagulation and when IABP counterpulsation therapy is planned for greater than 24 hours or at lesser assist ratios.3
Although no conclusive data exist in the literature, some authorities recommend gradual weaning of the balloon pump before it is finally removed. Typically, a gradual reduction in the assist ratio from 1:1 to 1:2 and then to 1:3 over several hours is done. If hemodynamic stability is demonstrated at lesser assist ratios, the device can be safely removed. Another weaning protocol involves the gradual reduction of the balloon volume over the course of an hour. This latter method may provide a more gradual resumption of the demands of intrinsic hemodynamic support on the heart.20
Complications. Complications arising from IABP counterpulsation therapy can be categorized into vascular and nonvascular events. In the Benchmark Registry, which included almost 17,000 patients who had an IABP inserted between 1996 and 2000, major complications (defined as major limb ischemia, severe bleeding, balloon leak, and death related directly to device insertion or to device failure) occurred in 2.6% of the patients.24 In this registry, the overall in-hospital mortality rate was 21%, one half of which occurred while the IABP was in place. However, mortality directly stemming from usage of the IABP was only 0.5%.25
The true incidence of complications associated with placement of an IABP is difficult to determine because of differing definitions. However, the frequency of complications is most likely decreasing as techniques, equipment, and experience with the device improve.3 Studies citing complication rates are diverse in terms of the indications for intra-aortic counterpulsation therapy, the insertion technique (surgical or percutaneous), the duration of use, and the specific definitions of a complication.24,26–30 The most common reported complications are bleeding and arterial trauma.3
Vascular complications occur in 6% to 25% of cases. The most common types of vascular complications include limb ischemia; vascular laceration necessitating surgical repair; and major hemorrhage.25,31–33 Arterial obstruction and limb ischemia can occur when the IABP is inadvertently placed into either the superficial or profunda femoral artery, instead of the common femoral artery. The superficial and the profunda femoral arteries are usually too small to accommodate the IABP without compromising blood flow to the limb. In this scenario, prompt removal of the device and contralateral insertion (with avoidance of an excessively low needle puncture) is the best solution. Arterial dissection can occur with improper advancement of a guidewire with subsequent insertion of the IABP into a false lumen. Vascular complications of lesser frequency include spinal cord ischemia along with visceral organ ischemia. Less frequent but nevertheless feared complications of IABP counterpulsation include cholesterol embolization, stroke, sepsis, and balloon rupture.25
Related posts:
 Evolution of the Coronary Care Unit: Past, Present, and Future
Evolution of the Coronary Care Unit: Past, Present, and Future
 Elevated Cardiac Troponin in the Absence of Acute Coronary Syndromes: Mechanism, Significance, and Prognosis
Elevated Cardiac Troponin in the Absence of Acute Coronary Syndromes: Mechanism, Significance, and Prognosis
 Conduction Disturbances in Acute Myocardial Infarction
Conduction Disturbances in Acute Myocardial Infarction
 Pharmacologic Interactions in the CICU
Pharmacologic Interactions in the CICU
 Acute Aortic Syndromes: Diagnosis and Management
Acute Aortic Syndromes: Diagnosis and Management
 Pacemaker and Implantable Cardioverter-Defibrillator Emergencies
Pacemaker and Implantable Cardioverter-Defibrillator Emergencies
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


