Identification of the Difficult and Failed Airway
Ron M. Walls
Michael F. Murphy
DEFINITION OF THE DIFFICULT AND FAILED AIRWAY
Although both difficult and failed airways are discussed in this chapter, the two concepts are distinct. A difficult airway is one for which a preintubation examination identifies attributes that are likely to make laryngoscopy, intubation, bag-mask ventilation (BMV), the use of an extraglottic device (EGD; e.g., Combitube and laryngeal mask airway [LMA]), or surgical airway management more difficult than would be the case in an ordinary patient without those attributes. Identification of a difficult airway is a key component of the approach to airway management for any patient and is a key branch point on the main airway algorithm (see Chapter 3). The key reason for this is that, in general, one should not administer a neuromuscular blocking medication to a patient unless one has a measure of certainty that oxygenation can be maintained if laryngoscopy and intubation fail. Accordingly, if a difficult airway is identified, the difficult airway algorithm is used.
A failed airway situation occurs when a provider has embarked on a certain course of airway management (e.g., rapid sequence intubation [RSI]) and has identified that intubation by that method is not going to succeed, requiring the immediate initiation of a rescue sequence (the failed airway algorithm, see Chapter 3). Certainly, in retrospect, a failed airway can be called a difficult airway because it has proven to be difficult or impossible to intubate, but the terms “failed airway” and “difficult airway” must be kept distinct because they represent different situations, require different approaches, and arise at different points in the airway management sequence. One way of thinking about this is that the difficult airway is something one anticipates and plans for; the failed airway is something one experiences.
Airways that are difficult to manage are fairly common in emergency practice, with some estimates being as high as 20% of all emergency intubations. However, the incidence of overall intubation failure is quite low, generally approximately 1% or less. Intubation failure can occur in a setting where the patient can be oxygenated by an alternative method, such as by BMV or using an EGD, or in a setting where the patient neither can be intubated nor oxygenated. The true incidence of the “can’t intubate, can’t oxygenate” (CICO) situation is unknown in emergency intubations but is estimated to represent between 1 in 5,000 and 1 in 20,000 operating room intubations.
This chapter explores the concepts of the failed and the difficult airway in the setting of emergency intubation. Recognizing the difficult airway in advance and executing an appropriate and thoughtful plan, guided by the difficult airway algorithm (see Chapter 3) will minimize the likelihood that airway management will fail. Furthermore, recognizing the failed airway promptly allows use of the failed airway algorithm to guide selection of a rescue approach.
THE FAILED AIRWAY
A failed airway exists when any of the following conditions is met:
1. Failure to maintain acceptable oxygen saturation during or after one or more failed laryngoscopic attempts (CICO) or
2. Three failed attempts at orotracheal intubation by an experienced intubator, even when oxygen saturation can be maintained or
3. The single “best attempt” at intubation fails in the “Forced to Act” situation (see below).
Clinically, the failed airway presents itself in two ways, dictating the urgency created by the situation:
1. Can’t Intubate, Can’t Oxygenate: There is not sufficient time to evaluate or attempt a series of rescue options, and the airway must be secured immediately because of an inability to maintain oxygen saturation by BMV or with an EGD.
2. Can’t Intubate, Can Oxygenate: There is time to evaluate and execute various options because the patient is oxygenated.
The most important way to avoid airway management failure is to identify in advance those patients for whom difficulty can be anticipated with intubation, BMV, insertion of an EGD, or cricothyrotomy. In the “Forced to Act” scenario, airway difficulty is apparent, but the clinical conditions (e.g., combative, hypoxic, and deteriorating patient) force the operator’s hand, requiring administration of RSI drugs in an attempt to create the best possible circumstances for tracheal intubation, with immediate progression to failed airway management if that one best attempt is not successful (see Chapter 3).
THE DIFFICULT AIRWAY
The emergency airway algorithms are discussed in Chapter 3. According to the main emergency airway management algorithm, RSI is the method of choice for any non-crash airway when airway management difficulty is not anticipated. This requires a reliable and reproducible method for identifying the difficult airway. This evaluation must be expeditious, easy to remember, and complete.
In clinical practice, the difficult airway has four dimensions:
1. Difficult laryngoscopy
2. Difficult BMV
3. Difficult EGD
4. Difficult cricothyrotomy
A distinct evaluation is required for difficult laryngoscopy, difficult BMV, difficult EGD, and difficult surgical airway management, and each evaluation must be applied to each patient before airway management is undertaken (Fig. 2-1).
Difficult Laryngoscopy: LEMON
The concept of difficult laryngoscopy and intubation is inextricably linked to poor glottic view; the less adequate the glottic view, the more challenging the intubation. This concept, developed during an era when almost all intubations were done by direct laryngoscopy, appears to hold true even in the era of video laryngoscopy. Almost all research relating certain patient characteristics
to difficult or impossible intubation is based on studies of direct laryngoscopy. It is not possible to determine, based on current information, whether these same characteristics predict difficult video laryngoscopy, and, if so, to what degree. Video laryngoscopy almost invariably produces an excellent glottic view, independently of the need to align the various airway axes, as must occur during direct laryngoscopy (see Chapters 12 and 13.) Difficult laryngoscopy and intubation are uncommon, even rare, when certain video laryngoscopes are used. It follows that evidence-based guidelines for prediction of difficult video laryngoscopy may be challenging, or even impossible, to develop. Pending further information, however, we recommend performing a difficult laryngoscopy assessment, using the LEMON mnemonic, on all patients for whom intubation is planned.
to difficult or impossible intubation is based on studies of direct laryngoscopy. It is not possible to determine, based on current information, whether these same characteristics predict difficult video laryngoscopy, and, if so, to what degree. Video laryngoscopy almost invariably produces an excellent glottic view, independently of the need to align the various airway axes, as must occur during direct laryngoscopy (see Chapters 12 and 13.) Difficult laryngoscopy and intubation are uncommon, even rare, when certain video laryngoscopes are used. It follows that evidence-based guidelines for prediction of difficult video laryngoscopy may be challenging, or even impossible, to develop. Pending further information, however, we recommend performing a difficult laryngoscopy assessment, using the LEMON mnemonic, on all patients for whom intubation is planned.
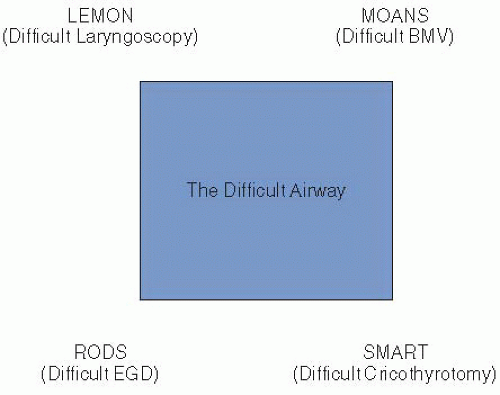 Figure 2-1 • Difficult Airway Box. Note that the four corners represent the four dimensions of difficulty. |
Cormack and Lehane introduced the most widely used system of categorizing the degree of visualization of the larynx during laryngoscopy, in which an ideal laryngoscopic view is designated grade 1 and the worst possible view grade 4 (Fig. 2-2). Cormack-Lehane (C-L) view grade 3 (epiglottis only visible) and grade 4 (no glottic structures at all visible) are highly correlated with difficult or failed intubation. C-L grade 1 (visualization of virtually the entire glottic aperture) and grade 2 (visualization of the posterior portion of the cords or the arytenoids) are not typically associated with difficult intubation. The C-L grading system does not differentiate precisely the degree to which the laryngeal aperture is visible during laryngoscopy: a grade 2 view may reveal little of the vocal cords, or none at all if only the arytenoids are visible. This has led some authors to propose a 2a/2b system, wherein a 2a shows any portion of the cords and a 2b shows only the arytenoids. Grade 2b accounts for only about 20% of grade 2 views. However, when a grade 2b view occurs, two-thirds of patients are difficult to intubate, whereas only about 4% of patients with grade 2a views are characterized as difficult intubations. A grade 1 view reveals virtually the entire glottis and is associated with almost universal intubation success.
Despite scores of clinical studies, no evidence to date reliably identifies which patient attributes predict successful laryngoscopy and intubation and which predict failure. Lists of anatomical features, radiologic findings, and complex scoring systems have been explored with only limited success. In the absence of a proven and validated system that is capable of predicting intubation difficulty with 100% sensitivity and specificity, it is important to develop an approach that will enable a clinician to quickly and simply identify those patients who might be difficult to intubate so an appropriate plan can be made using the difficult airway algorithm. In other words, when asking the question, “Does this patient’s airway warrant using the difficult airway algorithm, or is it appropriate and safe to proceed directly to RSI?” we value sensitivity (i.e., identifying all those
who might be difficult) more than specificity (i.e., always being correct when identifying a patient as difficult).
who might be difficult) more than specificity (i.e., always being correct when identifying a patient as difficult).
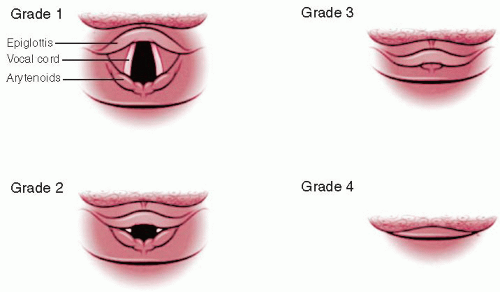 Figure 2-2 • C-L laryngeal view grade system. |
The mnemonic LEMON is a useful guide to identify as many of the risks as possible as quickly and reliably as possible to meet the demands of an emergency situation. The elements of the mnemonic are assembled from an analysis of the difficult airway prediction instruments in the anesthesia, emergency medicine, and critical care literature. The mnemonic, developed for The Difficult Airway CourseTM and the first edition of this book, has been externally validated and has been adopted as a recommended airway assessment tool in Advanced Trauma Life Support (ATLS). The mnemonic is as follows:
L—Look externally: Although a gestalt of difficult intubation is not particularly sensitive (meaning that many difficult airways are not readily apparent externally), it is quite specific, meaning that if the airway looks difficult, it probably is. Most of the litany of physical features associated with difficult laryngoscopy and intubation (e.g., small mandible, large tongue, large teeth, and short neck) are accounted for by the remaining elements of LEMON and so do not need to be specifically recalled or sought, which can be a difficult memory challenge in a critical situation. The external look specified here is for the “feeling” that the airway will be difficult. This feeling may be driven by a specific finding, such as external evidence of lower facial disruption and bleeding that might make intubation difficult, or it might be the ill-defined composite impression of the patient, such as the obese, agitated patient with a short neck and small mouth, whose airway appears formidable even before any formal evaluation (the rest of the LEMON attributes) is undertaken. This “gestalt” of the patient is influenced by patient attributes, the setting, and clinician expertise and experience, and likely is as valid for video laryngoscopy as for direct laryngoscopy.
E—Evaluate 3-3-2: This step is an amalgamation of the much-studied geometric considerations that relate mouth opening and the size of the mandible to the position of the larynx in the neck in terms of likelihood of successful visualization of the glottis by direct laryngoscopy. This concept originally was identified with “thyromental distance,” but has become more sophisticated over time. The thyromental distance is the hypotenuse of a right triangle, the two legs being the anteroposterior dimension of the mandibular space, and the interval between the chin-neck junction (roughly the position of the hyoid bone indicating the posterior limit of the tongue) and the top of the larynx, indicated by the thyroid notch. The 3-3-2 evaluation is derived from studies of the geometrical requirements for successful direct laryngoscopy, that is, the ability of the operator to create a direct line of sight from outside the mouth to the glottis. It is not known whether it has any value in predicting difficult video laryngoscopy, for which no straight line of sight is required. The premises of the 3-3-2 evaluation are as follows:
The mouth must open adequately to permit visualization past the tongue when both the laryngoscope blade and the endotracheal tube are within the oral cavity.
The mandible must be of sufficient size (length) to allow the tongue to be displaced fully into the submandibular space.
The glottis must be located a sufficient distance caudad to the base of the tongue that a direct line of sight can be created from outside the mouth to the vocal cords as the tongue is displaced inferiorly into the submandibular space.
The first “3,” therefore, assesses mouth opening. A normal patient can open his or her mouth sufficiently to accommodate three of his or her own fingers between the upper and lower incisors (Fig. 2-3A). The second “3” evaluates the length of the mandibular space by ensuring the patient’s ability to accommodate three of his or her own fingers between the tip of the mentum and chin-neck junction (hyoid bone) (Fig. 2-3B). The “2” assesses the position of the glottis in relation to the base of the tongue. The space between the chin-neck junction
(hyoid bone) and the thyroid notch should accommodate two of the patient’s fingers (Fig. 2-3C). Thus, in the 3-3-2 rule, the first 3 assesses the adequacy of oral access, and the second 3 addresses the dimensions of the mandibular space to accommodate the tongue on laryngoscopy. The ability to accommodate significantly more than or less than three fingers is associated with greater degrees of difficulty in visualizing the larynx at laryngoscopy: the former because the length of the oral axis is elongated and the latter because the mandibular space may be too small to accommodate the tongue, requiring it to remain in the oral cavity or move posteriorly, obscuring the view of the glottis. Encroachment on the submandibular space by infiltrative conditions (e.g., Ludwig angina) is identified during this evaluation. The final 2 identifies the location of the larynx in relation to the base of the tongue. If significantly more than two fingers are accommodated, meaning the larynx is distant from the base of the tongue, it may be difficult to reach or visualize the glottis on direct laryngoscopy. Fewer than two fingers may mean that the larynx is tucked up under the base of the tongue and may be difficult to expose. This condition is often imprecisely called “anterior larynx.”
(hyoid bone) and the thyroid notch should accommodate two of the patient’s fingers (Fig. 2-3C). Thus, in the 3-3-2 rule, the first 3 assesses the adequacy of oral access, and the second 3 addresses the dimensions of the mandibular space to accommodate the tongue on laryngoscopy. The ability to accommodate significantly more than or less than three fingers is associated with greater degrees of difficulty in visualizing the larynx at laryngoscopy: the former because the length of the oral axis is elongated and the latter because the mandibular space may be too small to accommodate the tongue, requiring it to remain in the oral cavity or move posteriorly, obscuring the view of the glottis. Encroachment on the submandibular space by infiltrative conditions (e.g., Ludwig angina) is identified during this evaluation. The final 2 identifies the location of the larynx in relation to the base of the tongue. If significantly more than two fingers are accommodated, meaning the larynx is distant from the base of the tongue, it may be difficult to reach or visualize the glottis on direct laryngoscopy. Fewer than two fingers may mean that the larynx is tucked up under the base of the tongue and may be difficult to expose. This condition is often imprecisely called “anterior larynx.”
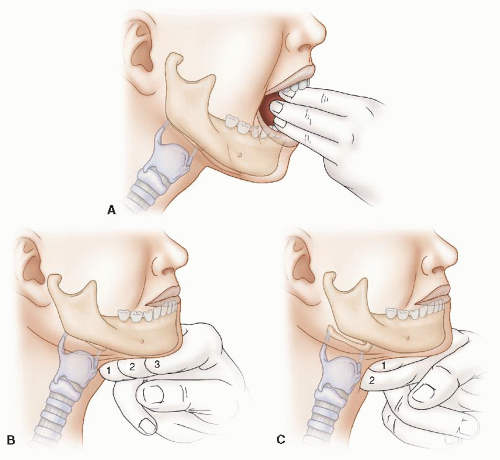 Figure 2-3 • A: The first 3 of the 3-3-2 rule. B: The second 3 of the 3-3-2 rule. C: The 2 of the 3-3-2 rule. |
M—Mallampati score: Mallampati determined that the degree to which the posterior oropharyngeal structures are visible when the mouth is fully open and the tongue is extruded reflects the
relationships among mouth opening, the size of the tongue, and the size of the oral pharynx, which defines access through the oral cavity for intubation, and that these relationships are associated with intubation difficulty. Mallampati’s classic assessment requires that the patient sit upright, open the mouth as widely as possible, and protrude the tongue as far as possible without phonating. Figure 2-4




relationships among mouth opening, the size of the tongue, and the size of the oral pharynx, which defines access through the oral cavity for intubation, and that these relationships are associated with intubation difficulty. Mallampati’s classic assessment requires that the patient sit upright, open the mouth as widely as possible, and protrude the tongue as far as possible without phonating. Figure 2-4
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
