Rapid Sequence Intubation
Ron M. Walls
INTRODUCTION
Definition
Rapid sequence intubation (RSI) is the administration, after preoxygenation, of a potent induction agent followed immediately by a rapidly acting neuromuscular blocking agent (NMBA) to induce unconsciousness and motor paralysis for tracheal intubation. The technique is predicated on the fact that the patient has not fasted before intubation and, therefore, is at risk for aspiration of gastric contents. The preoxygenation phase begins before drug administration and permits a period of apnea to occur safely between the administration of the drugs and intubation of the trachea, without the need for positive-pressure ventilation. In other words, the purpose of RSI is to render the patient unconscious and paralyzed and then to intubate the trachea without the use of bag-mask ventilation, which may cause gastric distention and increase the risk of aspiration. Sellick maneuver (posterior pressure on the cricoid cartilage to occlude the esophagus and prevent passive regurgitation) formerly was recommended, but it has been shown to impair glottic visualization in some cases, and the evidence supporting its use is dubious, at best. We no longer recommend routine use of this maneuver during emergency intubation.
Indications and Contraindications
RSI is the cornerstone of emergency airway management and is the technique of choice when emergency intubation is indicated, and the patient does not have difficult airway features felt to contraindicate the use of an NMBA (see Chapters 2 and 3). When a contraindication to succinylcholine is present, rocuronium is recommended as the NMBA (see Chapter 22). Some practitioners eschew the use of succinylcholine and routinely use rocuronium for all intubations; this is a matter of preference, for there are both pros and cons to this approach.
TECHNIQUE
RSI can be thought of as a series of discrete steps, referred to as the seven Ps. These are shown in Box 19-1.
1. Preparation
Before initiating the sequence, the patient is thoroughly assessed for difficulty of intubation (see Chapter 2). Fallback plans in the event of failed intubation are established, and the necessary equipment is located. The patient is in an area of the emergency department that is organized and equipped for resuscitation. Cardiac monitoring, BP monitoring, and pulse oximetry should be used in all cases. Continuous capnography provides additional valuable monitoring information, particularly after intubation. The patient has at least one, and preferably two, secure, well-functioning intravenous (IV) lines. Pharmacologic agents are drawn up in properly
labeled syringes. Vital equipment is tested. If a video or fiberoptic laryngoscope is to be used, it is turned on and image quality is verified. If a direct laryngoscope is to be used, the blade of choice is affixed to the laryngoscope handle and clicked into the “on” position to ensure that the light functions and is bright. The endotracheal tube (ETT) of the desired size is prepared, and the cuff tested for leaks. If difficult intubation is anticipated, a tube 0.5 mm less in internal diameter (ID) should also be prepared. Selection and preparation of the tube, as well as the use of the intubating stylet and bougie, are discussed in Chapter 12. Throughout this preparatory phase, the patient is receiving preoxygenation as described in the next section.
labeled syringes. Vital equipment is tested. If a video or fiberoptic laryngoscope is to be used, it is turned on and image quality is verified. If a direct laryngoscope is to be used, the blade of choice is affixed to the laryngoscope handle and clicked into the “on” position to ensure that the light functions and is bright. The endotracheal tube (ETT) of the desired size is prepared, and the cuff tested for leaks. If difficult intubation is anticipated, a tube 0.5 mm less in internal diameter (ID) should also be prepared. Selection and preparation of the tube, as well as the use of the intubating stylet and bougie, are discussed in Chapter 12. Throughout this preparatory phase, the patient is receiving preoxygenation as described in the next section.
Box 19-1. The Seven Ps of RSI
1. Preparation
2. Preoxygenation
3. Pretreatment
4. Paralysis with induction
5. Positioning
6. Placement with proof
7. Postintubation management
2. Preoxygenation
Preoxygenation is essential to the “no bagging” principle of RSI. Preoxygenation is the establishment of an oxygen reservoir within the lungs, blood, and body tissue to permit several minutes of apnea to occur without arterial oxygen desaturation. The principle reservoir is the functional residual capacity in the lungs, which is approximately 30 ml per kg. Administration of 100% oxygen for 3 minutes replaces this predominantly nitrogenous mixture of room air with oxygen, allowing several minutes of apnea time before hemoglobin saturation decreases to <90% (Fig. 19-1). Similar preoxygenation can be achieved much more rapidly by having the patient take eight vital capacity breaths (the greatest volume breaths the patient can take) while receiving 100% oxygen.
Obese patients are best preoxygenated when placed approximately 25° to 30° upright, and oxyhemoglobin desaturation is significantly delayed if oxygen is continuously administered at 5 L per minute by nasal cannula throughout the intubation sequence. In nonobese patients, desaturation also is delayed and reduced by continuous administration of oxygen at 5 L per minute during apnea.
The time to desaturation for an individual patient varies, depending on particular patient attributes, with children, morbidly obese patients, chronically ill (especially cardiopulmonary) patients, and late-term pregnant women desaturating significantly more rapidly than an average healthy adult does.
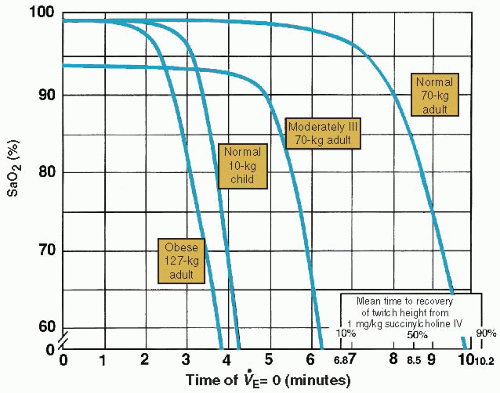 Figure 19-1 • Time to Desaturation for Various Patient Circumstances. (From Benumof J, Dagg R, Benumof R. Critical hemoglobin desaturation will occur before return to an unparalyzed state following 1 mg/kg IV succinylcholine. Anesthesiology. 1997;87:979.) |
Note the bars indicating recovery from succinylcholine paralysis on the bottom right of Figure 19-1. This demonstrates the fallacy of the oft-cited belief that a patient will quite likely recover sufficiently from succinylcholine-induced paralysis to breathe on his or her own before sustaining injury from hypoxemia, even if intubation and mechanical ventilation are both impossible. Although many patients will recover adequate neuromuscular function to breathe on their own before catastrophic desaturation, many others, including almost all children, will not, and even those who do are dependent on optimal preoxygenation before paralysis.
A healthy, fully preoxygenated 70-kg adult will maintain oxygen saturation at >90% for 8 minutes, whereas an obese adult will desaturate to 90% in <3 minutes. A 10-kg child will desaturate to 90% in <4 minutes. The time for desaturation from 90% to 0% is even more important and is much shorter. The healthy 70-kg adult desaturates from 90% to 0% in <120 seconds, and the small child does so in 45 seconds. A late-term pregnant woman is a high oxygen user, has a reduced functional residual capacity, and has an increased body mass, so she desaturates quickly in a manner analogous to that of the obese patient. Particular caution is required in this circumstance because both the obese patient and the pregnant woman may also be difficult to intubate and to bag-mask ventilate.
Most emergency departments do not use systems that are capable of delivering 100% oxygen. Typically, emergency department patients are preoxygenated using the “100% nonrebreather mask,” which delivers approximately 65% to 70% oxygen (see Chapter 5). In physiologically well patients in whom difficult intubation is not anticipated, this percentage is often sufficient and adequate preoxygenation is achieved. However, higher inspired fractions of oxygen are often desirable and can be delivered by active breathing through the demand valve of bag-mask systems equipped with a one-way exhalation valve, or by specially designed high-concentration oxygen delivery devices. Oxygen delivery is discussed in detail in Chapter 5. The use of pulse oximetry throughout intubation enables the physician to monitor the level of oxygen saturation eliminating guesswork.
3. Pretreatment
Pretreatment is the administration of drugs to mitigate adverse effects associated with the intubation or the patient’s underlying comorbidities. These adverse effects include bronchospastic reactivity of the airways to the ETT in patients with reactive airways disease, the intracranial pressure (ICP) response to airway manipulation in patients with elevated ICP, and systemic release of sympathetic adrenergic amines (the reflex sympathetic response to laryngoscopy [RSRL]). The pretreatment drugs are shown in Box 19-2 and discussed in detail in Chapter 20. Because there are three classes of patients for whom pretreatment is indicated, the mnemonic “ABC” can be used: Asthma (representing reactive airways disease), Brain (representing elevated ICP), and Cardiovascular (representing those at risk from RSRL; i.e., patients with ischemic heart disease, vascular disease [especially cerebrovascular disease], hypertension, and vascular events, such as aortic dissection, intracranial hemorrhage, etc.). The two drugs, fentanyl and lidocaine, and their relationship to the ABC conditions can be represented in a Venn diagram (Fig. 19-2). The pretreatment agents, when indicated, are administered 3 minutes before the induction and neuromuscular blocking agents.
4. Paralysis with induction
In this phase, a rapidly acting induction agent is given in a dose adequate to produce prompt loss of consciousness (see Chapter 21). Administration of the induction agent is immediately followed by the NMBA, usually succinylcholine (see Chapter 22). If succinylcholine is
contraindicated, rocuronium is used. Both the induction agent and the NMBA are given by IV push. RSI involves neither the slow administration of the induction agent nor a titration-to-end point approach. The sedative agent and dose are selected with the intention of rapid IV administration of the drugs. Although rapid administration of the induction agent can increase the likelihood and severity of side effects, especially hypotension, the entire technique is predicated on rapid loss of consciousness, rapid neuromuscular blockade, and a brief period of apnea without interposed assisted ventilation before intubation. Therefore, the induction agent is given as a rapid push followed immediately by a rapid push of the NMBA. Within a few seconds of the administration of the induction agent and NMBA, the patient will begin to lose consciousness, and respiration will decline, and then cease.
contraindicated, rocuronium is used. Both the induction agent and the NMBA are given by IV push. RSI involves neither the slow administration of the induction agent nor a titration-to-end point approach. The sedative agent and dose are selected with the intention of rapid IV administration of the drugs. Although rapid administration of the induction agent can increase the likelihood and severity of side effects, especially hypotension, the entire technique is predicated on rapid loss of consciousness, rapid neuromuscular blockade, and a brief period of apnea without interposed assisted ventilation before intubation. Therefore, the induction agent is given as a rapid push followed immediately by a rapid push of the NMBA. Within a few seconds of the administration of the induction agent and NMBA, the patient will begin to lose consciousness, and respiration will decline, and then cease.
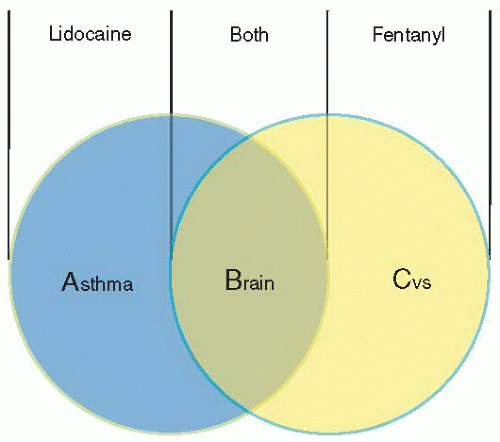 Figure 19-2 • Pretreatment Agents for RSI—the ABC Approach. CVS, cardiovascular system. |
5. Positioning
After 20 to 30 seconds, the patient is apneic and becoming flaccid. If succinylcholine has been used as the NMBA, fasciculations will be observed during this time. The oxygen mask used for preoxygenation remains in place to prevent the patient from acquiring even a partial breath of room air. At this point, the patient is positioned optimally for intubation, with consideration for cervical spine immobilization in trauma. Some patients, as discussed in Section VIII of this manual, will be sufficiently compromised that they require assisted ventilation almost continuously throughout the sequence to maintain oxygen saturations over 90%. Such patients, especially those with profound hypoxemia, are ventilated with bag and mask at all times except when laryngoscopy is occurring. Morbidly obese patients will maintain high oxygen saturations longer if they receive oxygen at 5 L per minute through nasal cannula throughout laryngoscopy. It is likely that this benefit pertains also to other patients. When bag-mask ventilation is performed on an unresponsive patient, the application of Sellick maneuver may minimize the volume of gases passed down the esophagus to the stomach, possibly decreasing the likelihood of regurgitation.
6. Placement with proof
At 45 seconds after the administration of the succinylcholine, or 60 seconds if rocuronium is used, test the patient’s jaw for flaccidity and intubate. Because preoxygenation endows most patients with several minutes of safe apnea time, the intubation can be performed gently and carefully and multiple attempts, if needed, often are possible without any need to provide additional
oxygenation by bag and mask. Tube placement is confirmed as described in Chapter 12. End-tidal carbon dioxide (ETCO2) detection is mandatory. A capnometer, such as a colorimetric ETCO2 detector, is sufficient for this purpose. Continuous capnography provides additional and ongoing information.
oxygenation by bag and mask. Tube placement is confirmed as described in Chapter 12. End-tidal carbon dioxide (ETCO2) detection is mandatory. A capnometer, such as a colorimetric ETCO2 detector, is sufficient for this purpose. Continuous capnography provides additional and ongoing information.
7. Postintubation management
After placement is confirmed, the ETT is secured in place. Mechanical ventilation should be initiated as described in Chapter 7. A chest radiograph should be obtained to assess pulmonary status and ensure that mainstem intubation has not occurred. Hypotension is common in the postintubation period and is often caused by diminished venous blood return as a result of the increased intrathoracic pressure that attends mechanical ventilation, exacerbated by the hemodynamic effects of the induction agent. Although this form of hypotension often is self-limited and responds to IV fluids, more ominous causes should be sought. BP should be measured, and if significant hypotension is present, the management steps in Table 19-1 should be considered.
Long-term sedation almost always is indicated. Long-term paralysis, however, generally is avoided, except when necessary. Use of a sedation scale, such as the Richmond Agitation Sedation Scale, to optimize patient comfort helps guide decision making regarding the necessity of neuromuscular blockade (Box 19-3




Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
