Femoral Nerve Block

FIGURE 21-1. Needle insertion for femoral nerve block.
General Considerations
A femoral nerve block is a quintessential nerve block technique that is easy to master, carries a low risk of complications, and has significant clinical application for surgical anesthesia and postoperative pain management. The femoral block is well-suited for surgery on the anterior thigh and knee, quadriceps tendon repair, and postoperative pain management after femur and knee surgery. When combined with a block of the sciatic nerve, anesthesia of almost the entire lower extremity from the midthigh level can be achieved.
Functional Anatomy
The femoral nerve is the largest branch of the lumbar plexus, arising from the second, third, and fourth lumbar nerves. The nerve descends through the psoas muscle, emerging from the psoas at the lower part of its lateral border, and it runs downward between the psoas and the iliacus. The femoral nerve eventually passes underneath the inguinal ligament into the thigh, where it assumes a more flattened shape (Figure 21-2). The inguinal ligament is a convergent point of the transversalis fascia (fascial sac lining the deep surface of the anterior abdominal wall) and iliac fascia (fascia covering the posterior abdominal wall). As it passes beneath the inguinal ligament, the nerve is positioned lateral and slightly deeper than the femoral artery between the psoas and iliacus muscles. At the femoral crease, the nerve is on the surface of the iliacus muscle and covered by the fascia iliaca or sandwiched between two layers of fascia iliaca. In contrast, vascular fascia of the femoral artery and vein, a funnel-shaped extension of the transversalis fascia, forms a distinctly different compartment from that of the femoral nerve but often contains the femoral branch of the genitofemoral nerve lateral to the vessels (Figure 21-3). The physical separation of the femoral nerve from the vascular fascia explains the lack of spread of a “blind paravascular” injection of local anesthetic toward the femoral nerve.
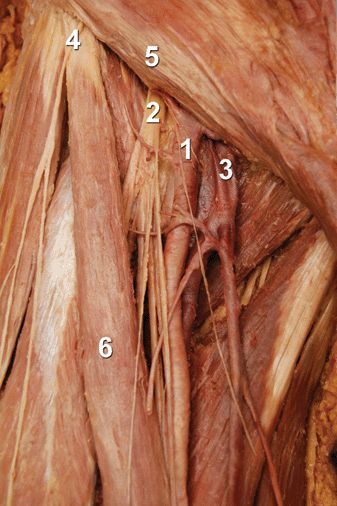
FIGURE 21-2. Anatomy of the femoral triangle. ![]() femoral artery.
femoral artery. ![]() femoral nerve.
femoral nerve. ![]() femoral vein.
femoral vein. ![]() anterior superior iliac spine.
anterior superior iliac spine. ![]() inguinal ligament.
inguinal ligament. ![]() sartorius.
sartorius.
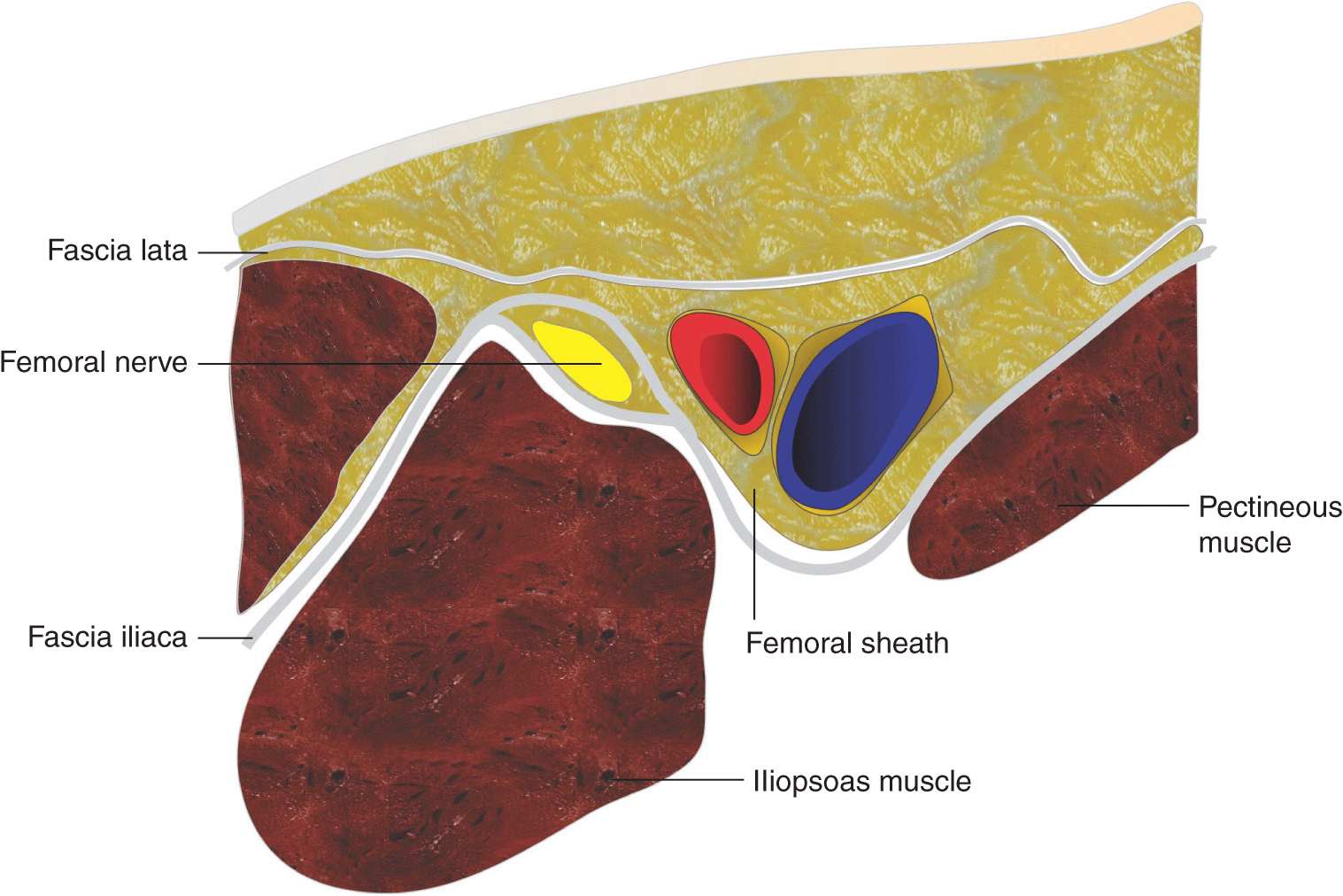
FIGURE 21-3. Arrangement of the fascial sheaths at the femoral triangle. Femoral nerve is enveloped by two layers of fascia iliaca, whereas femoral vessels are contained in the vascular (femoral) sheath made up of fascia lata.
The branches to the sartorius muscle depart from the anteromedial aspect of the femoral nerve toward the sartorius muscle. Because sartorius muscle twitch may be the result of the stimulation of this specific branch and not the femoral nerve, the sartorius motor response should not be accepted. Although the needle in the proper position (close to the main trunk of the femoral nerve) often results in sartorius muscle twitch, quadriceps twitch results in more consistent blockade, and it routinely should be sought before injecting local anesthetic unless ultrasound is used concomitantly.
The femoral nerve supplies the muscular branches of the iliacus and pectineus and the muscles of the anterior thigh, except for the tensor fascia lata. The nerve also provides cutaneous branches to the front and medial sides of the thigh, the medial leg and foot (saphenous nerve), and the articular branches of the hip and knee joints (Table 21-1).
TABLE 21-1 Femoral Nerve Branches
Distribution of Blockade
Femoral nerve block results in anesthesia of the skin and muscles of the anterior thigh and most of the femur and knee joint (Figure 21-4). The block also confers anesthesia of the skin on the medial aspect of the leg below the knee joint (saphenous nerve, a superficial terminal extension of the femoral nerve).
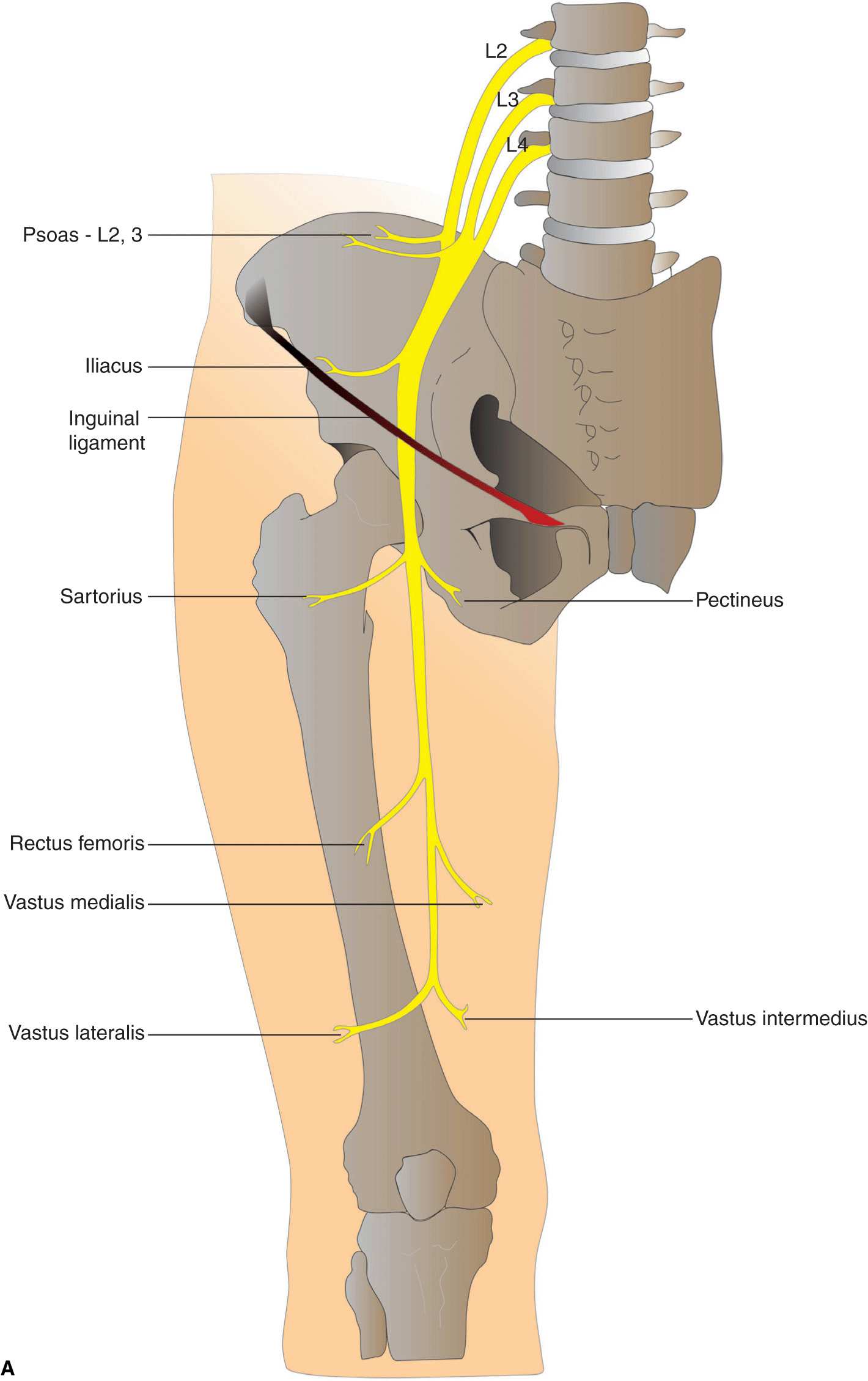
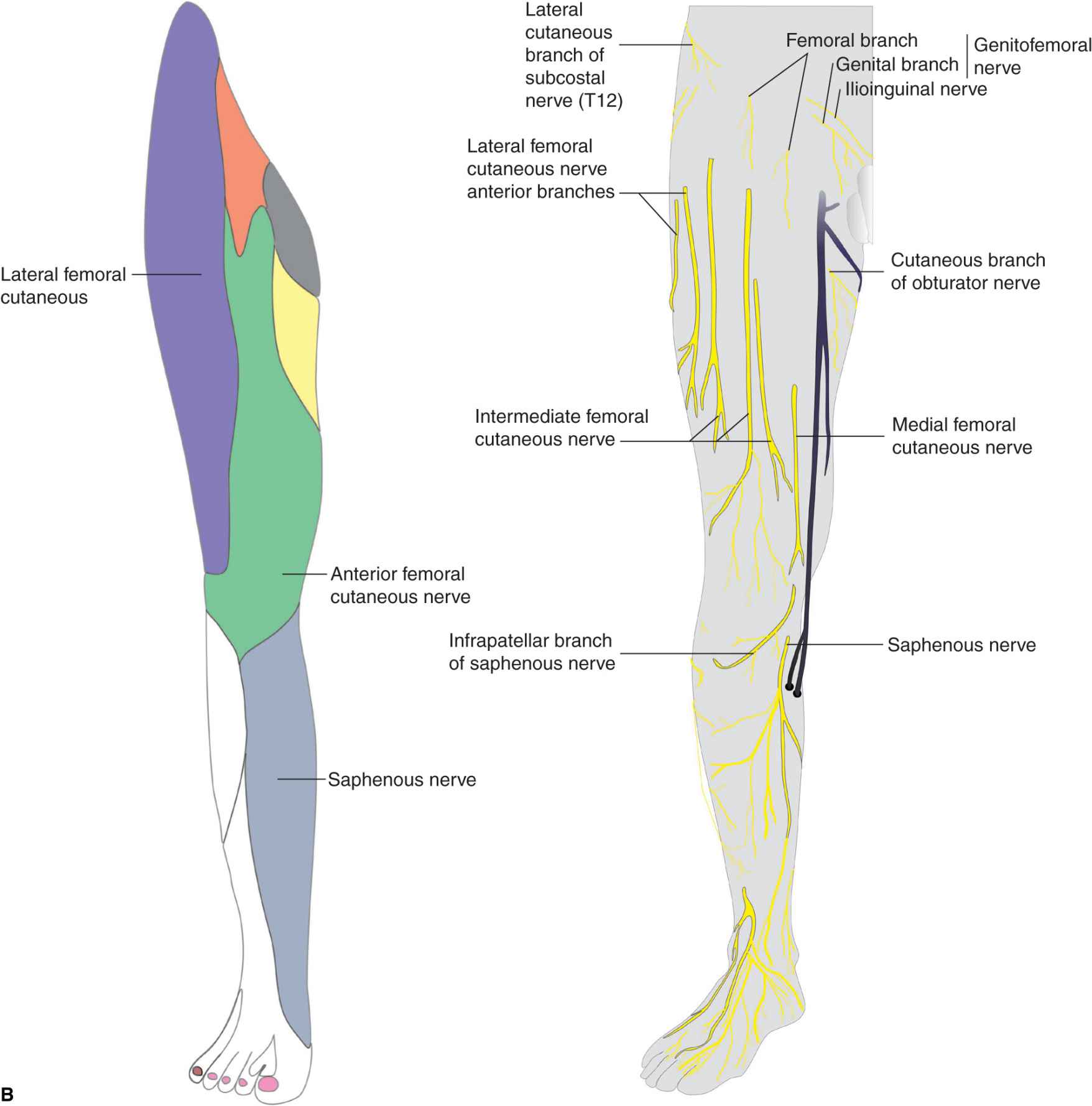
FIGURE 21-4. (A) Motor innervation of the femoral nerve. (B) Sensory innervation of the femoral nerve and its cutaneous branches.
Single-Injection Femoral Nerve Block
Equipment
A standard regional anesthesia tray is prepared with the following equipment:
• Sterile towels and gauze packs
• One 20-mL syringe containing local anesthetic
• A 3-mL syringe plus 25-gauge needle with local anesthetic for skin infiltration
• A 5-cm, 22-gauge short-bevel insulated stimulating needle
• Peripheral nerve stimulator
• Sterile gloves; marking pen
Landmarks and Patient Positioning
The patient is in the supine position with both legs extended. In obese patients, a pillow placed underneath the hips can facilitate palpation of the femoral artery and the block performance.
Landmarks for the femoral nerve block are easily recognizable in most patients and include the femoral crease (Figure 21-5) and femoral artery pulse (Figure 21-6).
FIGURE 21-5. Femoral nerve block is performed at the level of the femoral crease (line).
FIGURE 21-6. The main landmark for the femoral nerve block is the femoral artery, which is palpated at the level of the femoral crease. Needle insertion point is just lateral to the pulse of the femoral artery.
The following maneuvers can be used to facilitate landmark identification:
• The femoral crease can be accentuated in obese patients by having an assistant retract the lower abdomen laterally.
• Retraction of the abdomen should be maintained throughout the procedure to facilitate palpation of the femoral artery and performance of the block.
• Avoid excessive pressure on the crease when palpating for the artery because it can distort the landmarks.
The needle insertion site is labeled immediately lateral to the pulse of the femoral artery (Figure 21-6). All landmarks should be outlined with a marking pen.
Technique
After thorough preparation of the area with an antiseptic solution, local anesthetic is infiltrated subcutaneously at the estimated site of needle insertion. The injection for the skin anesthesia should be shallow and in a line extending laterally to allow for a more lateral needle reinsertion when necessary. The anesthesiologist should stand at the side of the patient with the palpating hand on the femoral artery. The needle is introduced immediately at the lateral border of the artery and advanced in sagittal, slightly cephalad plane (Figure 21-1).
After initial stimulation of the femoral nerve is obtained, the stimulating current is gradually decreased until twitches are still seen or felt at 0.2 to 0.4 mA, which typically occurs at a depth of 2 to 3 cm. After obtaining negative results from an aspiration test for blood, 15 to 20 mL of local anesthetic is injected slowly.
Troubleshooting
When stimulation of the quadriceps muscle is not obtained on the first needle pass, the palpating hand should not be moved from its position. Instead, visualize the needle plane in which the stimulation was not obtained and:
• Ensure that the nerve stimulator is properly connected and functional.
• Withdraw the needle to skin level, redirect it 10° to 15° laterally, and repeat needle advancement (Figure 21-7).

FIGURE 21-7. When lateral redirection of the needle does not bring about motor response, the needle is reinserted 1 cm lateral to the original reinsertion point.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


