Chapter 9 Evaluation and Recognition of the Difficult Airway
I Introduction
The quest to forecast difficult airway (DA) management has spanned more than a half century. In that time, a plethora of scientific investigations, book chapters, editorials, lectures, and workshops have been devoted to this essential issue. In 1956, Cass and colleagues underscored the point and began the search for a simple beside test to determine whose airway will be difficult to manage.1 As of this writing, such a test does not exist.2 Practitioners apply multiple tests, none of which are accurate. Absent reliable data, airway managers depend on case reports and personal experience to formulate critically important airway management plans.3
The medical literature boasts an abundance of articles discussing predictors of difficult intubation (DI) but relatively few explaining predictors of difficult mask ventilation (DMV). Among all of them, practitioners seek to determine which criteria are dependable and which are not.4 Having established a basis on which to predict DMV or DI or both, it becomes possible to select modes of airway management that optimize patients’ safety and comfort.
Generally, failed endotracheal intubation occurs once in every 2230 attempts.5 The average anesthesiologist in the United States has one failed intubation every other year. The incidence is small, but the potential consequences of DA management are of major importance. Failed ventilation accounted for 44% of intraoperative cardiac arrests reported by Keenan and Boyan.6 Thirty-four percent of liability claims identified by Caplan and coauthors were based on adverse respiratory events,7 of which three quarters were judged to be preventable.8
Radiographs and other imaging techniques have been advocated to predict DI but are too expensive and inconvenient to serve as routine screening tests. Highly specialized techniques such as acoustic reflectometry are of dubious reliability.9 More quantitative, noninvasive measurements, such as those with the laryngeal indices caliper,10 bubble inclinometer,11 and goniometer, offer the potential for accurate measurements but have never found their way into clinical practice.
A history of DA is a strong predictor of future problems12; in my opinion, it is the single most reliable predictor of a DA. The contrapositive is not necessarily true, however. A history of problem-free airway management is suggestive of future ease but not a guarantee. Many factors that contribute to difficulty are progressive with time. Examples of such problems include rheumatoid arthritis and obesity. An airway history should be elicited from all patients. Review of prior anesthesia records is frequently helpful; they may describe previously encountered problems, failed therapies, and successful solutions.13
II Problematic Ventilation by Traditional Face Mask
DMV occurs when a practitioner cannot provide sufficient gas exchange because of inadequate mask seal, large volume leaks, or excessive resistance to the ingress or egress of gas.13 The incidence of DMV varies between 0.08% and 5%.14,15 This wide range is probably related to conflicting definitions of DMV.16 Impossible mask ventilation occurs in 0.07% to 0.16% of patients.15,17 Risk factors for DMV include full beard, massive jaw, edentulous state, skin sensitivity (e.g., burns, epidermolysis bullosa, fresh skin grafts), facial dressings, obesity, age older than 55 years, and a history of snoring.15 Other criteria that suggest the possibility of DMV include large tongue, heavy jaw muscles, history of obstructive sleep apnea (OSA), poor atlanto-occipital extension, some types of pharyngeal pathology, facial burns, and facial deformities18 (Box 9-1).
Box 9-1 Risk Factors for Difficult Mask Ventilation
Many types of pharyngeal problems can produce DMV, including lingual tonsil hypertrophy,19 lingual tonsillar abscess, lingual thyroid,20 and thyroglossal cyst.21–24 Many abnormalities cannot be diagnosed by classic airway examination techniques. The presence of any one factor is suggestive of DMV, and as factors increase in number, the likelihood of difficulty increases. A greater than normal mandibulohyoid distance has been associated with OSA, the pathophysiology of which may be related to DMV.25–27 Anesthetic technique could contribute to DMV. El-Orbany and Woehlck suggested that high-dose opioid–induced vocal cord adduction produces DMV.28
Traditional face mask airway management is generally safe and effective. In the unusual instances in which it is not, endotracheal intubation remains one fallback option. Although this scheme works well in most cases, approximately 15% of all DIs are also DMVs.29 Some factors that predispose to DMV also contribute to DI; they include OSA, history of snoring, obese neck, and poor mandibular translation. Some 25% of impossible mask ventilation patients are also difficult to intubate. The overall incidence of impossible mask ventilation and DI is 1 in every 2800 patients.30 Proposed predictors of impossible mask ventilation are listed in Box 9-2.
III Problematic Intubation by Traditional Laryngoscopy
A Sniffing Position
DI occurs when multiple attempts at endotracheal intubation are required.13 The presence or absence of airway pathology does not influence its definition. Traditional laryngoscopy is performed to visualize the laryngeal opening. The observing laryngoscopist is situated outside the airway, above the patient’s head. To see through the airway, light must travel from the glottic opening to the laryngoscopist’s eye. Because light travels in straight lines, the technique requires an uninterrupted linear path between larynx and observer. Most of the manipulations performed attempt to satisfy this criterion.
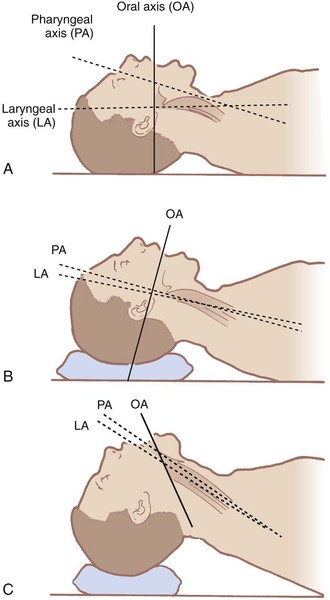
The airway contains three visual axes. They are the long axes of the mouth, oropharynx, and larynx. In the neutral position, these axes form acute and obtuse angles with one another (Fig. 9-1). Light cannot bend around these angles under normal circumstances. To bring all three axes into better alignment, McGill suggested the “sniffing the morning air” position.31 The true sniffing position has two components: cervical flexion and atlanto-occipital extension. Cervical flexion approximates the pharyngeal and laryngeal axes, and atlanto-occipital extension brings the oral axis into better alignment with the other two. Normal atlanto-occipital extension measures 35 degrees.32 With optimal alignment of the airway’s visual axes, it becomes possible to look through the airway into the laryngeal opening. A reduced atlanto-occipital gap or a prominent C1 spinous process impairs laryngoscopy33,34 if vigorous attempts at extension are performed, because the trachea bows and the larynx is forced anteriorly.33
The ability to achieve the sniffing position is easily tested. One simply has the patient flex the lower cervical vertebrae and extend at the atlanto-occipital joint. Pain, tingling, numbness, or inability to achieve these maneuvers predicts DI.35 The benefits of the sniffing position have been dogma for more than 70 years, but Adnet and colleagues and Chou and Wu have questioned its utility.36,37
B Mouth Opening
Mouth opening is important because it determines the available space for placing and manipulating laryngoscopes as well as endotracheal tubes.38,39 A small mouth opening may not accommodate either. Mouth opening also provides room to see through the uppermost part of the airway. Mouth opening relies on the temporomandibular joint (TMJ), which has both a hingelike movement and a gliding motion. The gliding motion is known as translation. The hingelike movement allows the mandible to pivot on the maxilla. The more the mandible swings away from the maxilla, the bigger the mouth opening.
The adequacy of mouth opening is assessed by measuring the interincisor distance. An interincisor distance of 3 cm provides sufficient space for intubation, absent other complicating factors. This corresponds approximately to two finger breadths.40 The two finger breadth test is performed by placing the examiner’s second and third digits between the patient’s central incisors. If they fit, there should be adequate room to perform laryngoscopy; if they do not fit, laryngoscopy may be difficult. Factors that interfere with mouth opening include masseter muscle spasm, TMJ dysfunction, and various integumentary aliments. Skin problems that adversely effect mouth opening include burn scar contractures and progressive systemic sclerosis. Masseter muscle spasm can be relieved by induction of anesthesia and administration of muscle relaxants. Mechanical problems at the TMJ remain unaltered by medications. Some patients demonstrate adequate mouth opening when awake but not after anesthesia induction.41 The problem can often be relieved by pulling the mandible forward. A mouth opening that was sufficient for a previous anesthetic may not be so after temporal neurosurgical procedures.42
D Tongue
A normal-size tongue usually fits easily into a normal-size mandibular space. A large tongue fits poorly into a normal-size mandibular space. After filling the space, a large tongue still occupies some of the oropharyngeal airway and obstructs it. For this reason, a large tongue (macroglossia) is a predictor of DI. Similarly, a normal-size tongue fits poorly into a small mandibular space.43 It, too, occupies some of the oropharyngeal airway, thereby obstructing the line of sight. Consequently, a small mandible (micrognathia) is a predictor of DI. In essence, a tongue that is large compared with the size of the mouth (oropharynx) and mandible takes up excessive space in the oropharynx and interferes with visualization.
The base of the tongue is located so close to the larynx that inability to adequately displace it anteriorly creates another problem. Because the base of the tongue hangs down over the larynx, the glottis is hidden from view. The glottic aperture is then anatomically anterior to the base of tongue—hence, the term anterior larynx. Under such circumstances, the larynx is anterior to the base of the tongue and cannot be seen because the tongue hides it. In this manner, glottic and supraglottic masses can create DI if they force the base of the tongue posteriorly. Some of the masses that may be encountered are lingual tonsils,19,44 epiglottic cysts,23 and thyroglossal duct cysts.
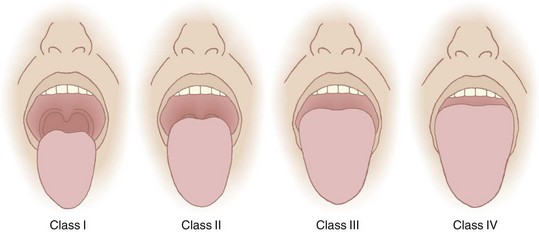
Recognizing the implications of tongue size for successful laryngoscopy, Mallampati and colleagues45 in 1985 and Samsoon and Young5 in 1987 devised classification systems to predict DL utilizing this concept. Mallampati and Samsoon reasoned that a large tongue could be identified on visual inspection of the open mouth. Both classification systems relate the size of the tongue to the oropharyngeal structures identified. A normal-size tongue allows visualization of certain oropharyngeal structures. As the tongue size increases, some structures become hidden from view. Both investigators proposed systems that reasoned backward from this premise.
Application of the Mallampati or the Samsoon classification system is easy and painless. The patient is seated in the neutral position. The mouth is opened as wide as possible, and the tongue is protruded as far as possible. Phonation is discouraged because it raises the soft palate and allows visualization of additional structures.46 The observer looks for specific anatomic landmarks: the fauces, pillars, uvula, and soft palate. The Mallampati classification system uses three groups and the Samsoon system uses four (Fig. 9-2). Both systems suggest that as tongue size increases, fewer structures are visualized and laryngoscopy becomes more difficult. Mallampati class tends to be higher in pregnant patients than in nonpregnant ones.47
Just as the size of tongue can be estimated, so too can the size of the mandible. The patient’s head is extended at the atlanto-occipital joint. The mentum of the mandible and the thyroid cartilage are identified. The “Adam’s apple” (thyroid notch) is the most superficial structure in the neck and serves as a good landmark for the thyroid cartilage. The vocal cords lie just caudad to the thyroid notch. The distance between the thyroid cartilage and the mentum (thyromental distance, or TMD) is measured in one of three ways: with a set of spacers, with a small pocket ruler, or with the observer’s fingers. The normal TMD is 6.5 cm. A TMD greater than 6 cm is predictive of easy intubation, and a TMD of less than 6 cm is suggestive of DI.48 If a ruler is not present at the bedside, practitioners can judge the TMD with their own fingers. The width of one’s middle three fingers frequently approximates 6 cm, and the TMD can be compared with the fingers’ span. In that way, clinically relevant approximations can be taken into account when examining patients for the purpose of predicting DI.
The ability to translate the TMJ is easily assessed before induction. The patient is simply asked to place the mandibular incisors (bottom teeth) in front of the maxillary incisors (upper teeth). Inability to perform this simple task usually results from one of two sources. First, the TMJ may not glide, predicting DI.49 Second, some patients find it difficult to coordinate the maneuver, in which case there is no implication for DI.
The upper lip bite test was proposed as a modification of the TMJ displacement test.50 The upper lip bite test is performed by asking the patient to move the mandibular incisors as high on the upper lip as possible. The maneuver is similar to biting the lip. Contact of the teeth above or on the vermilion border is thought to predict adequate laryngoscopic views. Inability to touch the vermilion boarder with the mandibular teeth is thought to predict poor laryngoscopic views. Both the TMJ translation test and the upper lip bite test assess TMJ glide, which is an important consideration during laryngoscopy. Khan and coworkers confirmed the predictive importance of this maneuver.51 Table 9-1 summarizes a quick, easy, bedside scheme for predicting DI.
TABLE 9-1 Generally Accepted Predictors of Difficult Intubation
| Criterion | Suggestion of Difficult Intubation |
|---|---|
| History of difficult intubation | Positive history |
| Length of upper incisors | Relatively long |
| Interincisor distance | Less than two finger breadths (<3 cm) |
| Overbite | Maxillary incisors override mandibular incisors |
| Temporomandibular joint translation | Inability to extend mandibular incisors anterior to maxillary incisors |
| Mandibular space | Small, indurated, encroached upon by mass |
| Cervical vertebral range of motion | Cannot touch chin to chest or cannot extend neck |
| Thyromental distance | Less than three finger breadths (<6 cm) |
| Mallampati-Samsoon classification | Mallampati III/Samsoon IV—relatively large tongue: uvula not visible |
| Neck | Short, thick |
Adapted from American Society of Anesthesiologists Task Force on Difficult Airway Management: Practice guidelines for management of the difficult airway: An updated report. Anesthesiology 98:1269, 2003.
IV Special Situations
A Morbid Obesity

In patients with MO, adipose tissue deposits in the lateral pharyngeal walls. These deposits are not fixed to bone and are highly mobile. They protrude into the airway, narrowing it, and are drawn farther into the airway during periods of negative airway pressure, such as during inspiration. In these ways, reduced dilator muscle function or pharyngeal adipose depositions predispose to OSA. (See Chapter 43 for further details.)
Although time to oxyhemoglobin desaturation is not a predictor of DI, it is an important consideration. The longer the time available to perform laryngoscopy, the greater the likelihood of success. Rapid hemoglobin desaturation limits that time and thereby reduces the chance of endotracheal intubation. A patient with MO and a BMI of 40 kg/m2, breathing room air, who becomes apneic desaturates to an oxygen saturation in arterial blood (SaO2) of 90% in approximately 1 minute, and to 60% in the next minute. In contrast, if the same patient is breathing 100% O2 before induction of anesthesia, the SaO2 takes approximately 21/2 minutes to fall to 90% and does not reach 60% for an additional 11/2 minutes.51,52 The data show that successful oxygenation before induction of anesthesia extends the period of time until oxyhemoglobin desaturation takes place. Consequently, preoxygenation provides a longer period for laryngoscopy, which should increase the chances of successful intubation.
Although OSA pathology and pathophysiology predispose to DMV and DI, the true incidence of problems resulting from MO is undefined. The popularity of bariatric surgery has brought numerous patients with MO to the operating room. Because these patients receive face mask ventilation infrequently, there is little practical experience to refute classic teachings about such ventilation. It is reasonable to expect fat cheeks, a short immobile neck, a large tongue, and pharyngeal adipose deposits to complicate face mask ventilation.53 Nevertheless, Brodsky and colleagues reported on a morbidly obese patient with a BMI of 43 kg/m2 and OSA who was ventilated easily by face mask.54 This experience serves to document the clinical findings of many practitioners. Along the same lines, considerable experience with laryngoscopy in patients with MO has developed. Absent findings to the contrary, most of these patients are easy to intubate. In other words, MO does not appear to be a strong independent predictor of DI.54–57 The presence of other DI predictors implies potential problems.58 Gonzalez and colleagues suggested that a neck circumference greater than 43 cm (19 inches) is such a predictor.59 Pretracheal fat accumulation has been investigated as a predictor of DI, but the results have been conflicting.60,61
Related posts:
 Physiologic and Pathophysiologic Responses to Intubation
Physiologic and Pathophysiologic Responses to Intubation
 Complications of Managing the Airway
Complications of Managing the Airway
 Ultrasonography in Airway Management
Ultrasonography in Airway Management
 Nonintubation Management of the Airway: Airway Maneuvers and Mask Ventilation
Nonintubation Management of the Airway: Airway Maneuvers and Mask Ventilation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


