CHAPTER 37
Endoscopic Discectomy
INTRODUCTION
Endoscopic discectomy is a minimally invasive treatment for disc herniation, protrusion, or extrusion. The goal of endoscopic discectomy is to provide relief from nerve root compression through the removal of herniated nuclear material. Endoscopic discectomy is also a therapeutic option for cases of advanced degeneration with proven discogenic pain. Endoscopic discectomy can be approached differently for the 2 basic types of disc herniations, contained and noncontained, both of which can be carried in an outpatient setting. The focus of this discussion is on contained herniations or disc bulges.
INDICATIONS
• Contained disc herniations within the annulus or posterior longitudinal ligament (typically 6-10 mm)
• Unilateral leg pain greater than back pain
• Radicular/neurological symptoms in a specific dermatomal distribution that correlates with MRI/CT/discography findings
• Positive straight leg raising test or positive bowstring sign, or both
• No improvement after 6 weeks of conservative therapy
• Well maintained disc height of 60% or more
• Alleviation of radicular pain with low volume selective nerve root block on the affected side at the operative level
• Facet joint pain should be excluded
Endoscopic discectomy should be strongly considered in patients with herniation within the far lateral recess beyond the intervertebral foramen. Such patients are difficult to treat with the traditional approach of microdiscectomy which may require removal of a large portion or the entire facet.
CONTRAINDICATIONS
• Diffuse annular bulge involving the entire circumference of the vertebral body
• Severe lateral recess stenosis
• Calcified disc herniations
• Severe degenerative facet disease
• Ligamentum flavum hypertrophy
• Free or extruded disc fragments within the spinal canal
• Clinical evidence of significant progressive neurologic deficits and/or cauda equina syndrome
• The existence of other pathologies or conditions, such as fracture, tumor, pregnancy, or active infection
• An absolute contraindication for endoscopic discectomy includes significant (>= 3 mm) migration of disc fragment
RELEVANT ANATOMY
• The central nucleus pulposus contains collagen fibers organized randomly, and elastin fibers arranged radially; these fibers are embedded in a highly hydrated aggrecan-containing gel.
• Interspersed at a low density are chondrocyte-like cells sitting in a capsule within the matrix.
• The annulus fibrosus is made up of a series of 15 to 25 concentric rings, or lamellae, with the collagen fibers lying parallel within each lamella. Elastin fibers lie between the lamellae.
• The posterior lamellar annular layers are thinner than in the anterior spine, which assists in spinal flexion and extension but also predisposes the posterior annulus to disruption.
• Trauma and internal disc derangement can lead to disc herniation, which consists of protrusion of the nucleus pulposus through the annulus fibrosus.
• The morphology of the macroscopic annulus fibrosus and the microscopic anatomy both undergo changes in disc herniation.
• The posterior concavity of the disc is often reduced or inverted, whereas the cellular structure itself in the annulus fibrosus undergoes a transformation from spindle-shaped cells to rounded chondrocytes at the area of disc herniation.
• The pathology of disc herniation is often a narrow neck of disc protruding through annular fibers with a “mushroom” head of the nucleus pulposus compressing the nerve roots, posterior longitudinal ligament (PLL), or dura.
• As the sinuvertebral nerve innervates the dura and PLL, inflammatory cytokines exuding from the exposed nucleus pulposus can cause back pain without leg pain.
• Compression of the nerve root by the disc herniation often produces dermatomal numbness, dysesthesia, reflex changes, and weakness.
• If the nerve root is not directly mechanically compressed, there may be radicular pain from the inflammatory response of the DRG to the chemicals and enzymes from the nucleus pulposus, but without the other signs of radiculopathy.
• The increased blood flow to the nerve root after discectomy suggests the mechanism of neurologic deficit is partially related to vascular ischemia from compression of the nerve root.
Other considerations for endoscopic discectomy include patient size, location of the disc herniation, neuroforaminal size, presence of furcal nerves, presence of overlying annular inflammatory membrane, disc height, anatomic impediments to access (osteophytes in the neural foramen, iliac crest morphology), and applicability to the technique selected.
BASIC CONCERNS
• Disc herniations are of two basic types: contained and noncontained. Contained herniated discs have an intact outer annulus with displaced disc material being held within the outer annulus of the contained herniated disc. In contrast, noncontained herniated disc has localized displacement of disc material beyond the intervertebral disc space and a breach in the outer annulus.
• Using the standard foraminal posterolateral approach, the morbidly obese patient presents anatomic limitations to treatment of disc herniations. The straight anteroposterior skin-to-skin measurement may be 15 cm or more. Using a 45-degree-angled insertion of a needle for endoscopic discectomy in a standard extrapedicular approach (as used in discography) would require a needle length of 21 cm or more (>8 in). Therefore, depending on the access needles or cannulas available, obese patients may not be candidates for endoscopic discectomy.
• Location of the disc herniation is less likely to be a significant determinant of success with most decompression systems utilizing an “inside-out” technique.
• A small neural foramen predisposes to injury during disc access with large needles because of the exiting nerve root being displaced inferiorly in the neural foramen. The “safe triangle” for disc access is smaller when there is significant apical foraminal impingement.
• The presence of osteophytes also causes some difficulties when there is zygapophyseal hypertrophy or vertebral body osteochondrosis.
• A calcified annulus fibrosus also causes some difficulty with disc access.
• The presence of a high iliac crest poses significant problems with rigid cannula or needle systems at L5-S1 because trajectory of the disk entry will predispose to damage to the superior S1 end plate, in addition to posing problems when nonflexible instruments are used through the cannula.
• Furcal nerves are accessory nerves present in approximately 15% of the population, and are found primarily at L4-L5. They traverse the foramen quite laterally and exit with the L5 nerve root. Compression of the furcal nerves with a lateral disc herniation can cause L4 and L5 symptoms. These are primarily sensory nerves and can be injured by a needle placed across the neural foramen into the disc.
• Inflammatory membranes over the surface of the annulus fibrosus are exquisitely sensitive to pressure and may make posterolateral needle placement quite painful.
PREOPERATIVE CONSIDERATIONS
• Informed consent and proper explanation of all potential complications including nerve root injury, infection, bleeding, development of spinal instability, damage to end plate, and disc space collapse.
• Anticoagulation should be corrected.
• Thorough physical examination of the lumbar region and lower extremities for assessment of neurologic symptoms as well as the absence of infection or skin ulceration.
• Patient must be able to lie prone for the intended length of the procedure.
• Intravenous access for IV fluid and medications for sedation. Sedation may be administered, but the patient’s level of consciousness must be carefully monitored to ensure that the patient can still respond to pain.
• Evaluation for contrast allergy.
• Strict sterile conditions are essential to reduce the potential for postoperative discitis.
• The patient should be administered cefazolin 1 to 2 gm intravenously 30 minutes prior to the procedure. Alternatively, if the patient is allergic to cephalosporin medication, Clindamycin 600 mg IV may be administered.
FLUOROSCOPIC VIEWS
Anterior-Posterior. The procedure is started with an anterior-posterior (AP) image of the lumbar spine with the desired level in view. The fluoroscopic beam should be aligned with cranial-caudal tilt such that it is parallel to the end plates of the vertebral bodies and the end plates appear “crisp” or on the edge.
Oblique. From the AP view, the C-arm is rotated in an oblique manner so that the superior articular process (SAP) of the inferior vertebra is in the midposition of the disc space and subsequently creates a inverted triangular opening to approach the disc, eg, for the L5-S1 level, the SAP forms this triangle’s medial border, the lateral border is made up by the iliac crest and superior border by the vertebral body end plate.
The lumbar discs superior to L5-S1 are typically easier to enter because the iliac crest lies lower and typically does not obstruct the view of the disc space. The L5-S1 disc space will typically require the most cranial tilt. Less cranial tilt is needed as one progresses to superiorly adjacent discs. Typically, a straight anteroposterior view is sufficient for the L3-4 disc and the L2-3 disc will actually need somewhat of a caudal tilt. For entrance to all disc levels, the SAP should be at the midpoint of the disc with the edges of the end plates clearly visualized.
Lateral. During penetration into the outer annulus and advancement into the nucleus pulposus, multiple AP and lateral images of the disc are obtained. The goal is to prevent unnecessary instrumentation and decrease the possibility of penetration into the anterior nucleus or annulus.
EQUIPMENT
See Figure 37-1. This image shows the Disc-FX kit with accessories available for the postero-lateral access to the intervertebral disc.
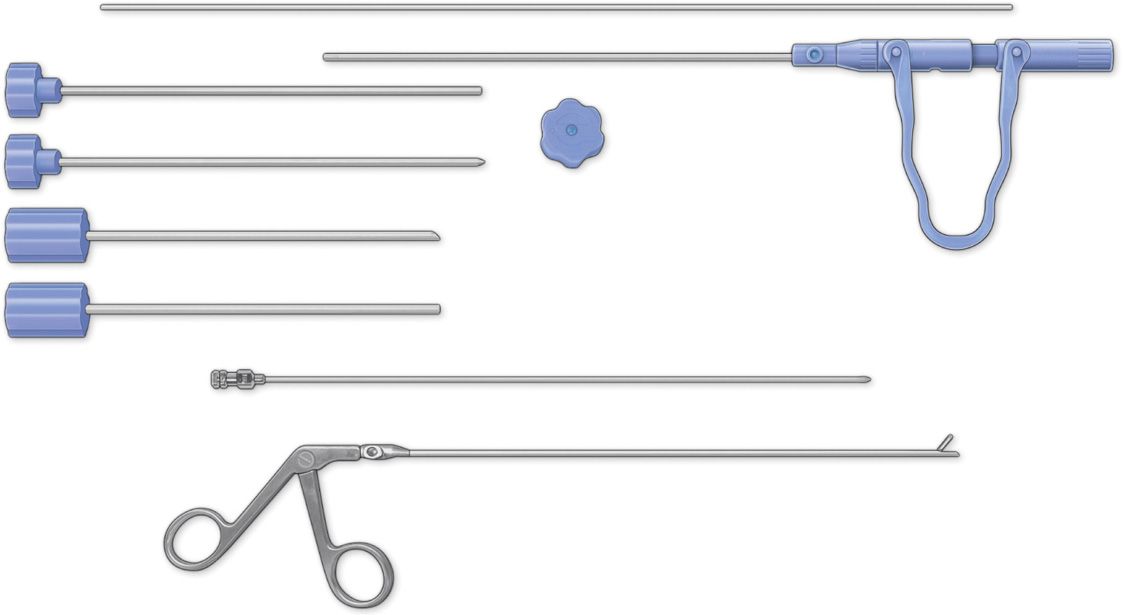
Figure 37-1. Disc-FX kit with accessories for posterolateral. (Reproduced with permission from Elliquence.)
EQUIPMENT FOR POSTEROLATERAL INTRADISCAL APPROACH
• Monitor, camera, and light source
• Bipolar system
• Spine scope sheath
• Spine scope with camera
• Standard IV tubing
• Spinal needle 18 or 16 gauge × 8 in
• Guidewires (thin and thick)
• Scalpel #11
• Tapered dilator
• Cannula, beveled
• Cannula depth stop
• Trephine
• Cannula, straight
• Graspers
• 10-cc syringe for local
• 10-cc syringe for Indigo carmine
EQUIPMENT FOR TRANSFORAMINAL APPROACH
• Multichannel, 20-degree oval spinal endoscope with 2.7 mm working channel and integrated continuous irrigation (inflow and outflow) ports
• Multichannel, 70-degree oval spinal endoscope
• 7-mm working cannula with various open slotted, beveled, and tapered ends
• 2-channel tissue dilator/obturator
• Specialized single and double action rongeurs for visualized fragmentectomy
• Larger straight and hinged rongeurs for discectomy and targeted fragmentectomy
• Trephines for annulotomy and foraminoplasty
• Micro rasps, curettes, and penfield probes
• Annulotomy knife
• Flexible bipolar radiofrequency probe
• Fluid pump for continuous irrigation
• Video endoscopy tower
Medications
• Lidocaine 1%
• Omnipaque
• Indigo carmine
• Normal saline for irrigation
Technique
The most common technique is through a postero-lateral approach described below:
POSTEROLATERAL TRANSDISCAL APPROACH
Step 1: Insertion of Needle into the Disc (Figure 37-2)
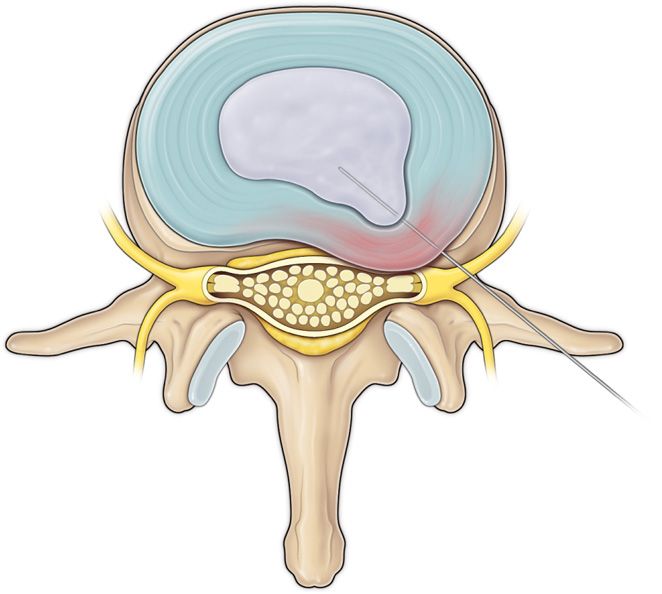
Figure 37-2. Step 1. Needle insertion by using posterolateral approach via Kambin’s triangle.
• The patient is placed in the prone position with a pillow or bolster to lessen the lumbar lordosis.
• Start with an AP image of the lumbar spine where the spinous processes of the operative levels are centered between the pedicles.
• Using a marking pen, draw lines connecting the spinous processes and lines across the disc space. Using a lateral view, disc inclination angles are drawn and the cephalad/caudal entry point is determined by the intersection of these lines.
• Once the entry point is determined, the skin window and subcutaneous tissues are infiltrated with local anesthesia.
• A 6-in, 18-gauge needle is then inserted from the skin window at the desired trajectory, using a posterolateral approach into the intervertebral disc via Kambin’s triangle, typically at a 30-degree angle to the floor (coronal plane) and passed anteromedially toward the anatomic disc center, infiltrating the needle tract with local anesthetic while advancing the needle.
• The lateral projection of C-arm should confirm correct annular location of the tip of the needle at the annular window (annular entry point).
• In the AP view, the needle tip should be at the disc between the pedicles. In the lateral view, the correct needle tip position should be just touching the posterior annulus surface. These two views of the C-arm confirm that the needle tip has engaged the safe zone, the center of the foraminal annular window.
• While monitoring the AP view, advance the needle tip though the annulus to the midline (anatomic disc center).
• Then check the lateral view. If the needle tip is in the center of the disc on the lateral view, it reflects a good position for central nucleotomy.
• For paracentral herniations, the needle tip should ideally be in the posterior one-third of the disc.
Step 2: Perform the Discogram
• Perform a confirmatory contrast discography. It is optional if the discogram has been performed before.
• The contrast mixture of a water-soluble contrast such as Iohexol and Indigo carmine dye is used.
• This combination of contrast ratio gives readily visible radiopacity on the discography images and intraoperative light blue chromatization of the pathologic nucleus and annular fissures help guide the targeted fragmentectomy.
Step 3: Insertion of the Guidewire through the Needle (Figure 37-3)
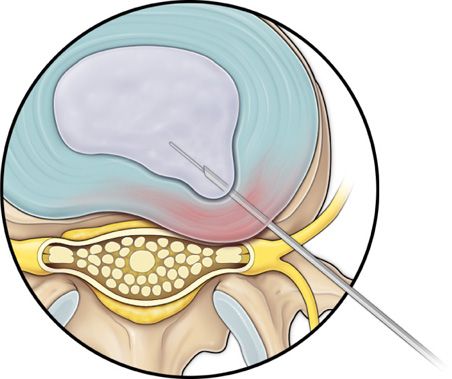
Figure 37-3. Step 3. Insertion of the guidewire through the needle; needle removed.
• Insert the guidewire through the 18-gauge needle channel. Advance the guidewire tip, 1 to 2 cm deep into the annulus, then remove the needle.
Step 4: Insertion of Cannula and Dilator over the Guidewire (Figure 37-4)
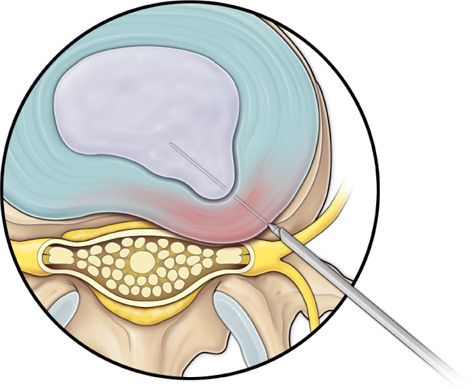
Figure 37-4. Step 4. The cannula and dilator passed over the guidewire.
• Make a 2-cm stab incision at the skin entry of the guidewire to facilitate placement of the dilating obturator.
• Slide the bluntly tapered tissue dilating obturator over the guidewire until the tip of the obturator is firmly engaged in the annular window.
Step 5: Perform Annulotomy (Figure 37-5)
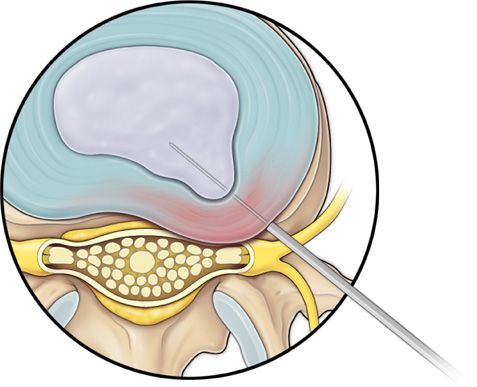
Figure 37-5. Step 5. Insertion of trephine or annulotome over the guidewire.
• Advance the bluntly tapered obturator, use mallet if required. Annular fenestration is the most painful step of the entire procedure. Advance the obturator tip deep into the annulus and confirm again with AP and lateral fluoroscopic views.
• Slide the beveled access cannula over the obturator toward the disc. Advance the cannula until the beveled tip is deep in the annular window with the beveled opening facing dorsally.
• Remove the dilator and insert trephine to perform the annulotomy.
Step 6: Perform Nucleotomy (Figures 37-6 and 37-7)
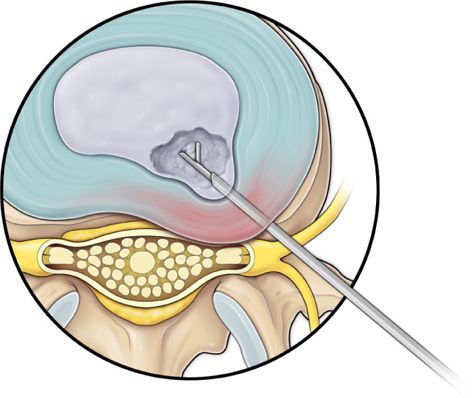
Figure 37-6. Step 6. Guidewire, trephine and dilator removed, and nucleus debulking forceps inserted.
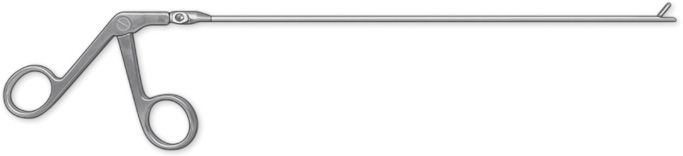
Figure 37-7. Nucleus debulking forceps.
• Remove the trephine or annulotome, insert the dilator and cannula, and advance to the center of nucleus pulposus.
• Remove the dilator and guidewire, and insert tissue debulking forceps or nucleotome to remove the disc material. The disc material is sent for biopsy.
• Enlarge the annulotomy medially to the base of the herniation with cutting forceps. This is performed to release the annular fibers at the herniation site that may pinch off or prevent the extruded portion of the herniation from being extracted.
• Directly under the herniation, a large amount of blue stained nucleus is usually present.
Step 7: Perform Radiofrequency Ablation (Figure 37-8)
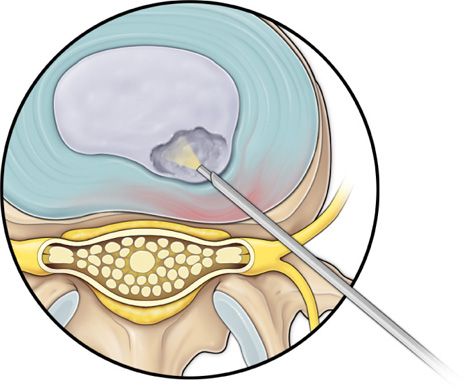
Figure 37-8. Step 7. The debulking forceps removed and flexible radiofrequency bipolar probe is inserted for nucleus ablation and annulus modulation.
• The flexible radiofrequency bipolar probe is used to contract and thickened the annular collagen at the herniation site. It is also used for hemostasis throughout the case.
Step 8: Endoscopic Visualization (Figure 37-9)
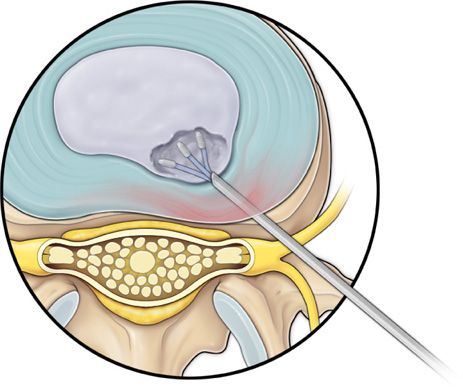
Figure 37-9. Step 8. Optional endoscopic observation of nucleotomy and annulus modulation.
• The disc visualization is optional to see the cavity created after the removal of disc material.
TRANSFORAMINAL APPROACH
• Most steps of this approach are similar up to steps 5 of the posterolateral transdiscal approach.
• The patient is positioned in the prone position with a pillow or bolster under the abdomen to lessen the lumbar lordosis.
• Using a posterolateral access, a 16- or 18-gauge spinal needle is introduced into the intervertebral disc via transforaminal approach.
• After an optional discography, a guidewire is placed through the needle.
• The needle is removed and a small skin incision of 2 mm is made for introduction of the dilator and working cannula.
• The dilator and working cannula are placed on the intervertebral disc annulus over the guidewire.
• An initial endoscopic inspection is carried out along with fluoroscopy, to ensure correct positioning. The 3 main steps of the procedure will be done through the placed cannula.
• Free subligamentary material is removed with the rongeur or the annulus is opened with the trepan provided for additional intradiscal work. Additional intervertebral disc material is then removed manually.
• The bipolar probe is inserted into the nucleus, and nuclear ablation is performed with a defined energy and frequency modulation. It is also possible to continue the nucleotomy using the rongeur.
• The relieved nucleotomy region can be checked with another endoscopic inspection.
• Modulation of the dorsal annulus can be performed by placing the bipolar probe on the pathological region and sweeping it dorsally.
• Subsequent retraction of the working cannula with a simultaneous endoscopic view can show the epidural space and the nerve roots after the decompression. If necessary, the instruments can be used again for continued decompression.
PERFORM ANNULOTOMY
• Advance the bluntly tapered obturator, use mallet if required. Annular fenestration is the most painful step of the entire procedure.
• Advance the obturator tip deep into the annulus and confirm again with AP and lateral fluoroscopic views.
• Slide the beveled access cannula over the obturator toward the disc.
• Advance the cannula until the beveled tip is deep in the annular window with the beveled opening facing dorsally and caudally (8 o’clock position).
• Remove the dilator and connect adaptor to end of cannula. Connect suction to cannula.
• Connect light source and white balance. Connect irrigation fluid.
CAVITY CREATION
• With cannula in the posterior and lateral third of the disc space, insert working channel into cannula.
• Dissection is performed with the rongeur and elliquence Trigger-Flex bipolar probe.
• With the opening of the bevel facing toward the spinal canal, dissection is continued to the posterior annular fibers.
• Nucleus pulposus near the herniation will stain blue secondary to the Indigo carmine.
• The herniated disc is extracted under direct visualization.
• Examine site for other.
• Radiofrequency can be used to thicken the annular collagen fibers at the herniations.
POSTPROCEDURE FOLLOW-UP
A procedure that does not result in substantial relief of pain should not be considered a failure until at least 6 weeks have passed postoperatively.
• Analgesics and anti-inflammatory medications can be given for a short period after the procedure.
• Closely monitor for procedure-related complications such as infection and/or bleeding.
• If the patient has a very inflamed nerve root, consider an image guided selective nerve root block to facilitate recovery.
• Postoperative physical therapy can be very helpful to facilitate recovery and prevent a re-herniation.
Postoperative discitis should be considered in all patients who develop:
• New or different back pain
• Radiation of pain to other areas of the body
• Tenderness around the spine
• Inability to bend without aggravation of pain
These patients may or may not exhibit systemic symptoms such as fever, chills, or weight loss. The appropriate work-up includes an erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), white blood cell count (WBC), and CT scan or MRI.
POTENTIAL COMPLICATIONS AND PITFALLS
Potential complications of endoscopic discectomy include:
• Nerve root injury
• Infection
• Bleeding
• Dural tears
• Scar tissue formation
• Development of spinal instability
• Damage to end plates and disc space collapse
Because the transforaminal endoscopic approach passes adjacent to the exiting spinal nerve root and dorsal root ganglia, there is potential for nerve irritation, dysesthesias, or overt nerve damage.
CLINICAL PEARLS
• For the oblique fluoroscopic view, positioning the SAP at the midpoint of the superior end plate will ensure that the nerve root is out of the introducer needle’s trajectory and decrease the risk of injury.
• A stab incision prior to placement of the introducer needle may facilitate appropriate needle placement and decrease the introduction of excessive force.
• During probe activation, the probe tip should be monitored under live fluoroscopy to decrease the possibility of inadvertently advancing the probe into the anterior annulus.
• In some systems, an eccentric parallel channel in the obturator allows for four-quadrant annular infiltration using small incremental volumes of local anesthetic in each quadrant, enough to anesthetize the annulus, but not the nerves.
• The use of local anesthesia and conscious sedation rather than general anesthesia or spinal anesthesia, and the use of standardized needle placement can decrease the occurrence of intraoperative nerve injury.
• The vast majority of herniations can be treated via the uniportal technique.
• Biportal technique allows better approach for large central herniations. This allows the use of larger articulating instruments that fit through the contralateral 7-mm access cannula under direct endoscopic vision.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


