Dizziness, Vertigo, and Ataxia
Henry Cohen MS, PharmD
Salah M. Mesad MD
DIZZINESS AND VERTIGO
Vertigo is a precise term, defined as a sensation of spinning or whirling motion; it implies a definite sensation of rotation of subject or of objects about the subject in any plane (Spraycar, 1991; Basmajian et al, 1992). Dizziness is an imprecise term, appropriately and commonly used by patients in an attempt to describe various subjective symptoms such as faintness (analogous to the feelings that precede syncope), giddiness, light-headedness, and unsteadiness; it may include vertigo (Spraycar, 1991; Basmajian et al, 1992). Dizziness is not mental confusion, blurred vision, headache, or tingling. Dizziness is one of the most common complaints causing patients to seek medical attention (Woodwell, 1989). In a United States national survey, dizziness was the 13th most common individual reason to visit a primary care provider (Herr et al, 1989). In a study from a general internal medicine outpatient clinic, dizziness was the third most frequent complaint (Kroenke & Mangelsdorff, 1989).
Anatomy, Physiology, and Pathology
Vertigo and dizziness can represent several different overlapping sensations; the pathophysiologic mechanisms are multifactorial. The vestibular nuclei, which are in the medulla and lower pons, receive input from the vestibular labyrinth via the vestibular branch of cranial nerve VIII and from the cerebellum (Herr et al, 1989). Vertigo is an illusion of motion without external stimuli, and it always indicates an imbalance within the vestibular system, although the symptom itself does not indicate where the imbalance originates. The maintenance of the sense of balance depends primarily on input from the vestibular labyrinth, visual system, and proprioceptive nerves arising from tendons, muscles, and joints (Frederick, 1973; Kelly, 1985). Therefore, vertigo and the sensation of dizziness can result from lesions in the inner ear, the deep paravertebral stretch receptors of the neck, the visual–vestibular interaction centers in the brain stem and cerebellum, the thalamus, or the cortex (Frederick, 1973; Baloh & Honrubia, 1990).
Nausea as a result of motion sickness is initiated by stimulation of the labyrinthine mechanism of the inner ear, which sends impulses to the chemoreceptor trigger zone (CTZ), in turn stimulating the vomiting center (VC). The CTZ, located in the area postrema of the fourth ventricle of the brain, is a major chemosensory organ for emesis. The VC is made up of a nucleus of cells located within the medulla. Vomiting is triggered by afferent impulses to the VC. Impulses are received from the sensory centers (eg, CTZ, gastrointestinal tract) and integrated by the VC, resulting in efferent impulses to the salivation center, respiratory center, and the pharyngeal, gastrointestinal, and abdominal muscles, ensuing in vomiting. The VC may also be directly stimulated by gastrointestinal irritation and vestibular neuritis. Enhanced activity of the central neurotransmitters, including dopamine in the CTZ, and acetylcholine in the VC, are major mediators for the emesis (Frederick, 1973; Baloh & Honrubia, 1990).
History and Physical Exam
Information from the history and physical exam can play a major role in determining the etiology of dizziness. Unfortunately, patients often have difficulty describing precise symptoms of dizziness. Therefore, the provider must take a careful history and perform a meticulous physical and neurologic exam to determine the type of dizziness; this will serve as a guide for confirmatory diagnostic studies (Herr et al, 1989; Adams & Victor, 1985; Lehrer & Poole, 1987). A cardiovascular exam should be done, including supine and standing blood pressure measurements in both arms, peripheral pulses, carotid bruits, heart murmur, and heart rate and rhythm. An ear exam is necessary to detect impacted cerumen or infection. Cerebellar function should be tested by performing the finger-to-nose test and having the patient tandem-walk while performing rapid alternating movements. Cranial nerves should be examined carefully by observing for any extraocular movement abnormality or nystagmus.
Dizziness when standing may be the result of vertigo, cerebral hypoperfusion, or disequilibrium (Kroenke et al, 1992). Dizziness when turning, and especially when rolling over in bed, is usually the result of vertigo. If the patient reports having symptoms of dizziness primarily while standing, both supine and standing blood pressure measurements and pulse rates should be determined. The patient should be allowed to be in both the supine and standing positions for at least 5 minutes before checking blood pressure and pulse rate. If there is an orthostatic decrease in blood pressure, the symptom is probably the result of impaired central nervous system (CNS) blood perfusion. Unsteadiness while walking, particularly in elderly patients, is often the result of disequilibrium, and its etiology is generally multifactorial. The presence of decreased visual acuity and signs of peripheral neuropathy or abnormal vestibular function supports a diagnosis of disequilibrium.
Psychogenic dizziness is a diagnosis of exclusion that should be especially considered in patients with psychiatric disorders, such as major depression, mania, anxiety disorder, and somatization disorders. The diagnosis of a hyperventilation syndrome can be established if symptoms of dizziness are reproduced by having the patient hyperventilate for 2 to 3 minutes.
Once the provider can establish that the patient is describing vertigo, further questioning will aid in determining the specific etiology. The provider must determine if vertigo is a recurrent or monophasic symptom and must assess the duration of the
episodes, the circumstances in which vertigo occurs, and the presence of other otologic or neurologic symptoms (Herr et al, 1989; Lehrer & Poole, 1987).
episodes, the circumstances in which vertigo occurs, and the presence of other otologic or neurologic symptoms (Herr et al, 1989; Lehrer & Poole, 1987).
Acute spontaneous vertigo can result from sudden loss of peripheral input caused by damage to the labyrinth or vestibular nerve, or it can be caused by a sudden unilateral impairment of vestibular nuclear or vestibulocerebellar activity (Kelly, 1985; Baloh & Honrubia, 1990). The patient experiences an intense sense of rotation aggravated by head motion and often by lying down, whereas sitting upright and keeping the head motionless relieves the vertigo. The patient usually notices that the visual world is moving slowly in one direction and quickly back in the other direction; this is the result of spontaneous nystagmus. Standing and walking are difficult, and the patient may fall toward the affected side. Acute spontaneous vertigo is almost always accompanied by autonomic symptoms, including malaise, pallor, diaphoresis, nausea, vomiting, and occasionally diarrhea.
The history often provides critical information that will aid in determining whether vertigo is peripheral (labyrinth) or central (brain stem or cerebellum) in origin (Table 53-1) (Herr et al, 1989; Frederick, 1973; Lehrer & Poole, 1987). Generally, peripheral vertigo is more severe than central vertigo and is more likely to be associated with autonomic symptoms, ear fullness or pressure, tinnitus, and hearing loss. Central vertigo is typically associated with neurologic symptoms such as diplopia, dysarthria, incoordination, numbness, and weakness. Lesions within the internal auditory canal produce a combination of vertigo, hearing loss, and facial weakness because of the involvement of cranial nerves VII and VIII. A prior history of cardiovascular disease (ie, hypertension) or stroke may suggest cerebral or brain stem vascular insult—hence, a central etiology. However, a prior history of ear trauma or ear infection accompanied by unilateral hearing loss suggests a peripheral etiology. Patients with central vestibular lesions often cannot stand or even walk a single step without falling.
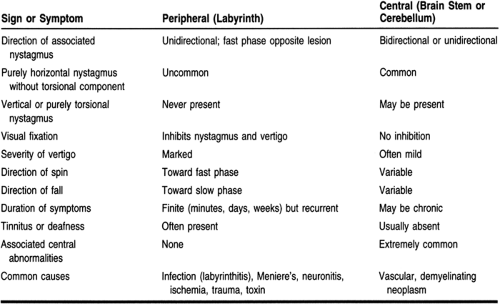 |
Patients with peripheral vestibular lesions have impaired balance, but they are able to ambulate, even during the acute phase. Spontaneous nystagmus of peripheral origin does not change direction with gaze in either side, although it increases in amplitude with gaze away from the fast phase. In contrast, spontaneous nystagmus of central origin typically changes direction when the patient looks away from the direction of the fast phase. Further, spontaneous nystagmus of peripheral vertigo is inhibited with fixation and therefore is usually prominent for only the first 12 to 24 hours. Spontaneous nystagmus of central vertigo often persists for weeks to months.
Magnetic resonance imaging (MRI) of the brain is indicated in patients with vertigo and focal neurologic findings, new-onset severe headaches, or vertical spontaneous or positional nystagmus. In the patient with acute vertigo and profound imbalance, cerebellar infarct or hemorrhage must be ruled out. Any central lesions or hemorrhaging must be identified immediately, because they can culminate in a mass effect with compression of the brain stem. If the indications for an MRI after a physical and neurologic exam are nebulous, the patient should be observed for 24 to 48 hours; on repeat neurologic examination without improvement, an MRI is indicated.
Recurrent attacks of vertigo may occur when there is a sudden temporary and largely reversible impairment of the labyrinth or its central connections (Herr et al, 1989; Frederick, 1973; Lehrer & Poole, 1987). Such attacks typically last minutes to hours rather than days and terminate through restoration of normal neural activity. The duration of vertigo episodes provides additional relevant diagnostic information. Vertigo of vascular origin, such as a transient ischemic attack, typically last minutes, whereas those of peripheral inner ear etiology generally persist for hours. On the neurologic exam, if focal neurologic findings are present, imaging studies of the head are warranted. However, patients with vertebrobasilar transient ischemic attacks often have a completely normal neurologic exam between attacks, and MRI of the brain is usually normal.
A screening audiogram and an electronystagmogram are indicated in all patients with recurrent vertigo that is likely to be of peripheral origin (eg, hearing loss) (Herr et al, 1989; Frederick, 1973; Lehrer & Poole, 1987). Vertigo accompanied by hearing loss is common in patients with otosclerosis. Episodes of vertigo with hearing loss, tinnitus, and the sensation of ear fullness occur in patients with Meniere’s disease. Patients
with acoustic neuromas usually have hearing loss rather than vertigo. Neurologic symptoms, which are generally referable to the posterior fossa, include diplopia, facial paresthesia or weakness, and dysarthria, as well as symptoms resulting from dysfunction of the motor and sensory tracts. Patients with vestibular neuronitis, benign paroxysmal positional vertigo, and recurrent vestibulopathy have normal hearing. Patients with benign positional vertigo (BPV) have intermittent episodes of vertigo with head turning. Vestibular neuronitis is characterized by a relatively sudden onset of severe constant vertigo that resolves after days or weeks. Patients with recurrent vestibulopathy have intermittent episodes of constant vertigo lasting for minutes or hours. Vertigo with or without hearing loss in a patient who has recently received aminoglycoside antimicrobials may be the result of an inherent toxic effect on the vestibular labyrinth (Jackson & Arcieri, 1971).
with acoustic neuromas usually have hearing loss rather than vertigo. Neurologic symptoms, which are generally referable to the posterior fossa, include diplopia, facial paresthesia or weakness, and dysarthria, as well as symptoms resulting from dysfunction of the motor and sensory tracts. Patients with vestibular neuronitis, benign paroxysmal positional vertigo, and recurrent vestibulopathy have normal hearing. Patients with benign positional vertigo (BPV) have intermittent episodes of vertigo with head turning. Vestibular neuronitis is characterized by a relatively sudden onset of severe constant vertigo that resolves after days or weeks. Patients with recurrent vestibulopathy have intermittent episodes of constant vertigo lasting for minutes or hours. Vertigo with or without hearing loss in a patient who has recently received aminoglycoside antimicrobials may be the result of an inherent toxic effect on the vestibular labyrinth (Jackson & Arcieri, 1971).
Benign Positional Vertigo
BPV is the most common cause of acute episodes of vertigo. It is characterized by brief (minutes or less) attacks of vertigo and nystagmus with certain head positions, such as lying down or turning over in bed, or tilting the head backward (Baloh et al, 1987). The patient can often identify a head position that can trigger symptoms. Symptoms may recur periodically for several days or months. Hearing is not affected. Diagnosis is confirmed by performing the Nylen-Barany maneuver, during which the patient is moved from the sitting position to a lying position with the head extended 45° backward. This maneuver is repeated with the head extended and turned to the right and to the left. The Nylen-Barany maneuver usually produces a brief attack of vertigo and nystagmus.
Positional vertigo nearly always is a benign condition. However, in rare cases, it is a symptom of a central lesion (in particular, the brain stem), including multiple sclerosis, tumors, stroke, or drug intoxications (alcohol and antiepileptic drugs). The Nylen-Barany maneuver helps distinguish benign positional nystagmus from more ominous central conditions. In BPV, there is a latency period for several seconds before the appearance of a transient vertigo and nystagmus, which dissipates on repetition of the Nylen-Barany maneuver. In BPV, nystagmus lasts less than 30 seconds and is unidirectional (Baloh et al, 1987). Any deviation from this characteristic nystagmus profile should raise suspicion that a central lesion may exist. Central positional nystagmus typically is nonfatiguing and purely vertical (either up- or downbeating). Most cases of central positional nystagmus have different neurologic findings.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


