Discogenic Pain: Lumbar Discography
A vertebral disc is built like a jelly doughnut. The inner jelly part is the nucleus pulposus and the outer layer is the anulus fibrosus (Fig. 28-1). Intervertebral discs have been a suspected source of spine pain, and in 1947 investigators identified a nerve supply to the disc. Nerve innervation of a vertebral disc is limited to the outer third of the anulus fibrosus. A healthy disc has a high water content and acts as a cushion between two vertebral bodies. As a disc loses water content over time, it shrinks and becomes prone to developing cracks and tears in the anulus fibrosus. Radial tears in the innervated layer of a vertebral disc, the anulus fibrosus may be a source of low back pain (Fig. 28-2). In fact, 39% of people with chronic low back pain have degenerative discs.1 However, a number of people who have degenerative discs on imaging have no pain. Simply having degenerative discs on imaging is not enough to diagnose discogenic pain. Degenerative disc(s) on imaging, focal low back pain, and pain that cannot be explained by other reasonable causes combined lead to the diagnosis of degenerative disc disease.
Provocative discography is a diagnostic test for discogenic pain, helping pinpoint the disc(s) in which the pain originates. The role of discography is to distinguish a symptomatic disc from similarly degenerative ones on the basis of pain reproduction. A needle is inserted into the nucleus pulposus and contrast is slowly injected under pressure, which stresses the disc. Typically, a disc will not produce pain when stressed with less than 50 pounds per square inch (psi) of pressure. During the discography procedure, the patient remains awake and alert while contrast is slowly injected. The patient reports whether the stress put on the disc during the injection reproduces the pain usually experienced. This is analogous to palpation for tenderness. This is a functional diagnostic test; thus although a patient may have three
degenerative discs on imaging and significant back pain, discography may reveal only one of the three degenerative discs that is actually a source of low back pain. Vanharanta et al.2 found that concordant pain (pain equivalent to the patient’s normal back pain) reproduced on discography correlated with the extent of annular disruption. This means that the more symptomatic the disc, the more dramatic the response would be on discography.
degenerative discs on imaging and significant back pain, discography may reveal only one of the three degenerative discs that is actually a source of low back pain. Vanharanta et al.2 found that concordant pain (pain equivalent to the patient’s normal back pain) reproduced on discography correlated with the extent of annular disruption. This means that the more symptomatic the disc, the more dramatic the response would be on discography.
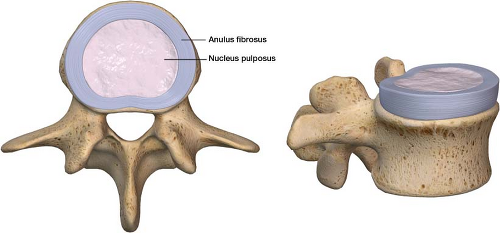 Figure 28-1 Intervertebral disc: Inner nucleus pulposus and outer annular fibrosus. |
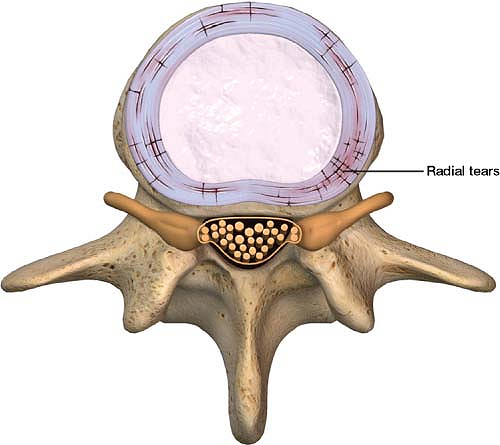 Figure 28-2 Radial tear in the anulus fibrosus. Radial tears in the innervated layer of a vertebral disc, the anulus fibrosus, are thought to be a source of low back pain. |
When to use
For focal back pain of suspected discogenic origin, it is appropriate to prescribe rest and physical therapy for a few weeks in patients who do not have progressive pain or significant neurologic deficit. If the pain does not improve and imaging reveals degenerative discs, it is appropriate to present interventional and surgical options. A series of epidural steroid injections is reasonable treatment option. If the patient does not respond. Discography is an interventional diagnostic test (not therapeutic), which can lead to surgical treatment if results are positive. A patients who refuse future surgical options such as fusion and artificial disc replacement (ADR) should not undergo this invasive diagnostic procedure. There is no point in obtaining the results of an interventional diagnostic test if you cannot act on the results.
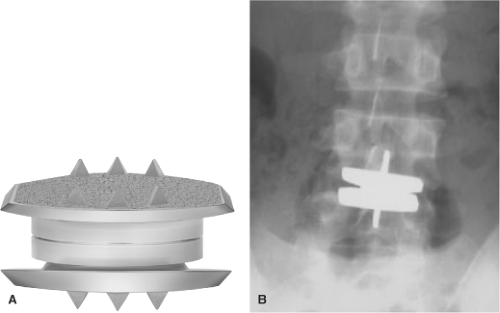 Figure 28-3 Artificial disc replacement. A: The CHARITE total disc replacement is composed of three parts; two cobalt-chromium alloy endplates and a sliding ultra-high-molecular-weight polyethylene (UHMWPE) core. B: Disc replacement at the L4 to L5 level. (A, from Bridwell KH, DeWald RL. The Textbook of Spinal Surgery, 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011,484; B, from Cox JM. Low Back Pain: Mechanism, Diagnosis, and Treatment, 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011,469.) |
Spine surgeons often obtain the results of provocative discography to help determine if a patient would benefit from an ADR or spinal fusion. In 2004, the Food
and Drug Administration (FDA) approved ADR which entails replacement of the painful disc with an artificial disc (Fig. 28-3). At this time, however, ADR does not have an excellent track record like knee and hip replacement. A spinal fusion fuses vertebral bodies in an attempt to alleviate pain and instability on the theory that removing the painful disc will stop pain. In patients undergoing fusion for low back pain, 89% derived significant relief when discography had revealed disc disease and pain reproduction, whereas only 52% derived relief when morphologic changes of the disc were seen but no pain reproduction was produced during discography.3 It is possible to fuse multiple levels if multiple discs are involved. Discography helps avoid fusion at a level where the disc is abnormal on imaging but functionally not producing pain.
and Drug Administration (FDA) approved ADR which entails replacement of the painful disc with an artificial disc (Fig. 28-3). At this time, however, ADR does not have an excellent track record like knee and hip replacement. A spinal fusion fuses vertebral bodies in an attempt to alleviate pain and instability on the theory that removing the painful disc will stop pain. In patients undergoing fusion for low back pain, 89% derived significant relief when discography had revealed disc disease and pain reproduction, whereas only 52% derived relief when morphologic changes of the disc were seen but no pain reproduction was produced during discography.3 It is possible to fuse multiple levels if multiple discs are involved. Discography helps avoid fusion at a level where the disc is abnormal on imaging but functionally not producing pain.
How to Perform the Procedure
It is important to explain the procedure to the patient completely, answer all questions, and obtain informed consent. (The practitioner should be sure to emphasize that this is a diagnostic, not a therapeutic, procedure. It is essential to clarify that discography will not provide pain relief and is, on the contrary, used to elicit pain.)
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


