Chapter 32 Confirmation of Endotracheal Intubation
I Overview
A American Society of Anesthesiologists Closed Claims Studies
For the past several decades, the Committee on Professional Liability of the American Society of Anesthesiologists (ASA) has studied adverse anesthetic outcomes based on closed claims files of nationwide insurance carriers.1 From the beginning, it was evident that adverse outcomes involving the respiratory system constitute the single largest class of injury, representing one third of the overall claims. Generally involving healthy adults undergoing nonemergency surgery with general anesthesia, three mechanisms of injury accounted for approximately three quarters of the adverse respiratory events in the 1970s and early 1980s: inadequate ventilation (38%), esophageal intubation (18%), and difficult endotracheal intubation (DI; 17%). The remaining adverse respiratory events were produced by a variety of low-frequency (≤2%) mechanisms, including airway obstruction, bronchospasm, aspiration, premature and unintentional extubation, inadequate inspired oxygen delivery, and endobronchial intubation.1
Care was judged to be substandard in more than 80% of the cases of inadequate ventilation and esophageal intubation. Almost all (>90%) of the claims for inadequate ventilation and esophageal intubation were considered preventable with better monitoring, compared with only 36% of claims for DI. Death and permanent brain damage were more frequent in claims for inadequate ventilation and esophageal intubation (>90%) than in claims for DI (56%). Median payments were $240,000 for inadequate ventilation, $217,000 for esophageal intubation, and $76,000 for DI.1
In 23% of the claims for esophageal intubation, there was documentation of DI; in 73%, there was sufficient information to reconstruct the time to detection of esophageal intubation. Within this latter subset, 3% of esophageal intubations were detected within 5 minutes, 61% in 5 to 10 minutes, and 36% after 10 minutes. Auscultation of breath sounds (presumed) was documented in 63% of the claims for esophageal intubation. In 48% of cases, auscultation led to the erroneous conclusion that the tube was in the trachea. This diagnostic error was eventually recognized in a variety of ways, including reexamination with direct laryngoscopy, absence of the endotracheal tube (ETT) in the trachea at the time of an emergency tracheostomy, resolution of cyanosis after reintubation, and discovery of esophageal intubation at autopsy. Cyanosis was documented in 52% of the claims and preceded the recognition of esophageal intubation in only 34% of the cases.1
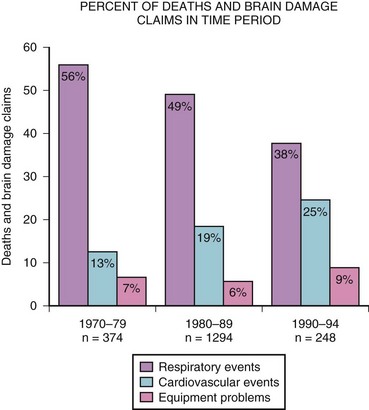
Because pulse oximetry and capnography have been used since the mid-1980s, data from the closed claims project were analyzed in 1999 to determine whether these monitoring modalities correlated with improvement in patients’ safety. After monitoring was instituted, respiratory events decreased, primarily in claims for injuries caused by inadequate ventilation and, to a lesser extent, esophageal intubation (Fig. 32-1).2
1 Pediatric Versus Adult Anesthesia Closed Malpractice Claims
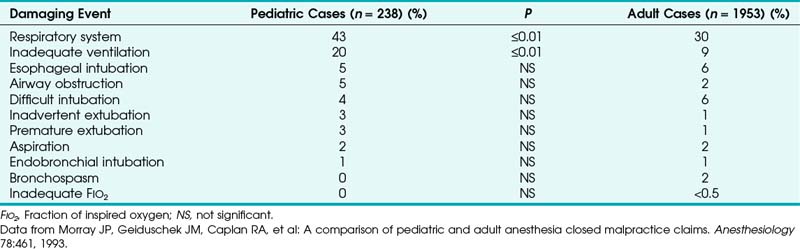
Outcome studies in pediatric patients revealed that adverse respiratory events constitute a leading cause of morbidity and mortality.3–5 The ASA closed claims study provided a database to compare pediatric and adult cases in which an adverse outcome occurred.5 The pediatric claims presented a different distribution of damaging events compared with claims of adults (Tables 32-1 and 32-2). Respiratory events and mortality rate were greater in pediatric claims.5 Anesthetic care was more often judged “less than appropriate,” and the complications more frequently were considered preventable with better monitoring. The median payment to the plaintiff was greater for pediatric claims than for adult claims. Cyanosis (49%), bradycardia (64%), or both often preceded cardiac arrest, resulting in death (50%) or brain damage (30%) in previously healthy children.5
TABLE 32-1 Comparison of Pediatric and Adult Damaging Events with Special Reference to the Respiratory System

B The Magnitude of the Problem of Endotracheal Tube Misplacement
Outcome studies have repeatedly identified adverse respiratory events including unrecognized esophageal intubation as a leading and recurring cause of injury in anesthetic practice.6–10 The report on confidential enquiries into maternal deaths in England and Wales in 1979-1981 revealed that 8 of 22 deaths attributable to anesthesia were related to difficulty in endotracheal intubation.9 In 4 patients, the ETT proved to be misplaced in the esophagus.9 An investigation of anesthesia deaths in Australia revealed that 69% were related to airway management, with esophageal intubation once again identified as an important contributing factor.8
All anesthesiologists experience esophageal intubations sometime in their career, especially during training and when difficulty in visualizing the larynx is encountered. Most esophageal intubations are immediately and easily recognized. What is intriguing is the rare situation in which misplacement of the ETT in the esophagus is not recognized, resulting in grave consequences. Failure to recognize esophageal intubation is not limited to junior residents or inexperienced personnel; it has occurred with experienced anesthesiologists. A case was reported in which three “consultant anaesthetists” failed to recognize esophageal intubation.6 There are also many case reports describing anesthetic catastrophes and near-disasters in patients whose esophagus had been unintentionally intubated and in whom some or many of the common signs indicative of proper ETT placement were misleading.8,11–17
Unintentional esophageal intubation occurs more frequently in emergency airway management, in critically ill patients, and in patients who suffer cardiac arrest during out-of-hospital paramedic intubation.18–20 In one report, esophageal intubation occurred in 8% of emergency intubation attempts in critically ill patients.20 In a study of paramedics trained in direct laryngoscopic endotracheal intubation, there were 14 esophageal intubations in 779 patients, an incidence of 1.8%.18 Esophageal tube placement was recognized and corrected in 11 of the 14 patients; three esophageal intubations (0.4% of the total) were not recognized and remained uncorrected. In another study, 25% of tracheas intubated in the prehospital setting had improperly placed ETTs detected on arrival at the hospital.21 Contributing factors to this high incidence of esophageal intubation include intubation under less than optimal conditions; unavailability of monitoring equipment, protocols, or algorithms; violation of the standard technique of auscultation of lung fields and the epigastrium; and intubation attempts by nonexpert personnel.18–22
II Confirmation of Endotracheal Tube Placement
A Is There an Ideal Test for Confirmation of Endotracheal Tube Placement?
Unfortunately, such a perfect test does not yet exist. Many clinical signs and technical aids have been described to confirm endotracheal intubation. A number of these reports relied on the placement of two ETTs, one in the trachea and the other in the esophagus.23–25 This scenario makes the observer’s decision as to which tube is in the trachea or esophagus much easier and helps in the recognition of esophageal intubation. However, the clinician does not have the luxury of choice between two ETTs in a given clinical situation.24,25
In the assessment of these tests, the reader must understand what is meant by false-negative and false-positive results. Although not all reports are in agreement, most use the term false-negative when the ETT is in the trachea but the test fails and false-positive when the ETT is in the esophagus but the result mimics that of endotracheal intubation.24,25 For capnography, a false-negative result occurs when the ETT is in the trachea but the waveform is absent, and a false-positive when the ETT is in the esophagus but the waveform is present.24,25 To avoid confusion and to maintain conformity, these definitions are retained throughout the discussion that follows.
B Methods of Verification of Endotracheal Tube Placement
1 Non-Failsafe Methods
a Observation and Palpation of Chest Movements
Commonly used maneuvers to confirm endotracheal intubation are observation of symmetrical bilateral chest movements and palpation of upper chest excursions during compression of the reservoir bag. These signs can easily distinguish tracheal from esophageal intubation in most patients. However, in obese patients, women with large breasts, and patients with a rigid chest wall, barrel chest, or less compliant lungs, these signs can be misinterpreted to indicate that the ETT is in the esophagus.26 More important, upper chest wall movements simulating ventilation of the lungs can be seen and felt with an esophageally placed ETT. This phenomenon has been described in many instances of what ultimately proved to be esophageal intubation, and it has been reported in patients with intrathoracic hiatal hernia and after gastric pull-up operations.11–1726
Pollard and Junius studied chest movements during esophageal ventilation in a male cadaver after a cuffed ETT was placed into the esophagus and attached to an inflating bag.16 As they reported, “Chest and epigastric movements observed when the bag was compressed were indistinguishable from those normally seen in ventilation of the lungs even in the upper chest area.” When the body was dissected starting with the epigastrium, it was noted that “the stomach was being inflated and was spontaneously deflating via the esophagus, the feel of the inflating bag being indistinguishable from normal pulmonary ventilation.” Even when the lower end of the esophagus was occluded, “chest movements still appeared identical to those seen when the lungs are inflated.” After the chest was entered, it was observed that “chest movements were caused by the flat esophagus distending into a firm tube that lifted the heart and upper mediastinal structures forward, elevating the sternum and ribs.” The lifting of the chest wall by the distended esophagus is the most plausible explanation for the presumed chest movements seen during esophageal ventilation. Another possible mechanism is that gastric insufflation causes upward displacement of the diaphragm and outward movement of the lower chest. With release of bag compression, gas escapes from the stomach up the esophagus, allowing the diaphragm to move downward and the lower chest to move inward.16
b Auscultation of Breath Sounds
There are several reasons why sounds heard with esophageal intubation may mimic breath sounds from the lungs. The combination of esophageal wall oscillations with gas movement and acoustic filtering can produce inspiratory or expiratory wheezes indistinguishable from sounds arising from gas movement in the airway.13,27,28 The high flow rate, distribution, and volume of gas delivered through the esophagus may lead to auscultation of predominantly bronchial breath sounds.13 In infants and children, esophageal sounds can be easily transmitted to wide areas of the chest wall.29 The quality of breath sounds may also differ depending on whether the chest is auscultated near the middle line or laterally near the axilla and may vary with the presence of pulmonary disease and from patient to patient.
Sounds retrieved by an esophageal stethoscope are different from those heard with a precordial stethoscope and should not be used to differentiate endotracheal from esophageal intuation.16,25 In patients with a thoracic stomach or hiatal hernia, many of the clinical signs of esophageal intubation may be obscured. Because of the intrathoracic location of a large distensible viscus, bilateral breath sounds may be heard during manual ventilation.12 For these reasons, whenever abnormal breath sounds are heard, they should not be relied on to confirm endotracheal intubations.30
Proper verification of ETT placement by auscultation is dependent on the clinician’s experience.31 In one study in the critical care setting, experienced clinicians identified ETT location correctly, whereas inexperienced examiners were correct in only 68% of cases.31
c Endobronchial Intubation
Intentional endobronchial intubation has been used to discriminate between endotracheal and esophageal intubation when doubt exists.32 The ETT is advanced until breath sounds are lost on one side and unilateral breath sounds are heard on the other side. That should not happen if the tube is in the esophagus. The ETT is then gradually withdrawn 1 to 2 cm beyond the point at which bilateral breath sounds are heard. This technique has been used in infants and children, particularly in infants with tracheoesophageal fistulas.33 However, it is not recommended for routine use because it can precipitate carinal irritation and bronchospasm.34
d Epigastric Auscultation and Observation for Abdominal Distention
Auscultation of the epigastric area to elicit air movement in the stomach has been suggested as a routine maneuver after endotracheal intubation, even before auscultation of the chest.14,15,25,26 However, normal vesicular breath sounds from the lungs can be transmitted to the epigastric area in tracheally intubated patients who are thin or small.26 On rare occasions, esophageal intubation may not be easily distinguishable from endotracheal intubation if epigastric auscultation alone is used. Furthermore, there are circumstances, such as obstetric emergencies, in which prepping of the abdomen before induction of anesthesia precludes epigastric auscultation after intubation.25
Abdominal distention caused by gastric insufflation after compression of the breathing bag in cases of esophageal intubation can be readily observed in most patients. Occasionally, this sign may not be a reliable indicator of esophageal intubation for the following reasons16,26,35:
1. Gastric insufflation and abdominal distention might have occurred during prior mask ventilation.
2. Gastric distention may not be apparent in obese patients.
3. A previously placed nasogastric tube (NGT) can cause intermittent decompression of the stomach.
4. Gradual gastric filling can be difficult to distinguish from normal abdominal movements because of the esophageal reflux of gases.
Conversely, gastric distention can occur in patients with congenital or acquired tracheoesophageal fistula despite placement of the tube in the trachea.33
e Combined Auscultation of Epigastrium and Both Axillae
In a study of 40 adult patients intubated in both the trachea and the esophagus, “blinded” observers auscultating both axillae failed to diagnose esophageal intubation in 15% of cases.36 When movement of the abdominal wall alone was used to assess ETT position, false results were obtained in 90% of cases. In contrast, the combined auscultation of the epigastrium and both axillae was found to be totally reliable in diagnosing esophageal intubation.36 These findings emphasize the importance of combining tests to achieve a high degree of reliability in assessing ETT placement.
Detection of misplaced ETTs by auscultation of the chest and epigastrium is probably more difficult in infants than in adults. Uejima reported on two children,29 aged 7 months and 5 years, in whom esophageal intubation occurred. In both, bilateral chest movements and breath sounds were heard over four areas of the chest and over the epigastrium. However, these “breath sounds” were not vesicular in nature. The ease of transmission of sounds from the esophagus to the chest and epigastrium may mimic breath sounds, especially in infants, emphasizing again that whenever any but normal vesicular breath sounds are heard, they should not be relied on to confirm endotracheal intubation.25
Attempts have been made to quantify and assess breath sound characteristics using electronic stethoscopes placed over each hemithorax and the epigastrium. With the use of computerized analysis, researchers digitized and filtered breath sounds to remove selected frequencies. Preliminary results suggested that this technique, when incorporated into a three-component, electronic stethoscope-type device, provides an accurate, portable mechanism to reliably detect ETT position in adults.37 However, before this method gains wide acceptance, further evaluation is necessary in a broader population of patients with a variety of pathologic states and with different conditions and environments.
f Reservoir Bag Compliance and Refilling
Manual compression of the reservoir bag after endotracheal intubation and cuff inflation yields a characteristic feel of compliance of the lungs and chest wall, whereas passive exhalation on release of bag compression is accompanied by rapid bag refilling. In almost all esophageal intubations, compressing the reservoir bag does not inflate the chest and is not followed by appreciable refilling. However, exceptions to this rule do occur, as has been shown in reports of accidental esophageal intubations. In these cases, repeated filling and emptying of the stomach resulted in concomitant emptying and refilling of the reservoir bag, leading to the erroneous conclusion that the ETT was in the trachea.13,14,16,17,35
It is possible that high fresh gas flow might have contributed to reservoir bag refilling in these cases. To enhance the reliability of this test, it has been suggested that the fresh gas flow should be shut off temporarily.38 If this is done, chest inflation and rapid bag refilling can be repeatedly done (three to five times) in tracheally intubated patients but not in esophageally intubated patients. Because changes in lung or chest wall compliance can be misinterpreted by the clinician compressing the reservoir bag and high airway resistance can lead to slow refilling, this test, used alone, should not be relied on to distinguish esophageal from endotracheal intubation.26
g Reservoir Bag Movements with Spontaneous Breathing
Movement of the reservoir bag during spontaneous breathing has been considered one of the signs indicative of endotracheal intubation. However, it has been demonstrated that this sign can be unreliable. In a group of anesthetized patients, the trachea and esophagus were intubated and the patients were allowed to breathe spontaneously.39 With the ETT intentionally occluded, the high negative intrapleural pressures generated with spontaneous breathing efforts were transmitted to the esophagus, resulting in reservoir bag movements and measurable tidal volumes (VT) up to 180 mL. Therefore, slight reservoir bag movements or measurements of small VT during spontaneous breathing are not reliable indicators of endotracheal intubation.39
h Cuff Maneuvers and Neck Palpation
The higher-pitched sound produced by leakage around a tube placed in the trachea with the cuff deflated during compression of the reservoir bag, compared with the “flatus-like” sound of leakage around a tube placed in the esophagus, has been used as a distinguishing test.26 As has been shown in case reports, when the cuff of an esophageally placed ETT is inflated close to the cricoid cartilage, the characteristic guttural sound may be absent or may become higher pitched, resembling leakage around a tracheally placed ETT.16
Palpation of the cuff on each side of the trachea between the cricoid cartilage and the suprasternal notch while moving the tube has been proposed to confirm endotracheal intubation.26 After intubation and cuff inflation, 2 or 3 fingers are placed above the suprasternal notch. Several rapid inflations of the cuff are performed (up to 10 mL of air). An outward force is felt by the palpating fingers if the ETT is in correct position. Intermittent squeezing of the pilot balloon of a slightly overinflated cuff with the thumb and index finger while sensing the transmitted pulsations in the neck has also been suggested as a sign for confirming ETT placement.40 Likewise, a maneuver using the pilot balloon as a sensor has been proposed.34 A high-volume, low-pressure, prestretched cuff may not be palpable despite correct placement.34 Conversely, an inflated cuff can be palpated in the neck in cases of esophageal intubations.17 Therefore, these maneuvers should not be relied on in verifying endotracheal intubation.25,26,30
If an assistant gently palpates the trachea in the suprasternal notch or applies cricoid compression during endotracheal intubation, an “old washboard-like” vibration is appreciated as the ETT rubs against the tracheal rings.41 It has been suggested that there should be no false-positive results of this sign if the ETT is misplaced in the esophagus, because the esophagus is soft and lies posterior to the trachea. Thus far, there have been no controlled studies to confirm the validity of this sign.
i Sound of Expelled Gases during Sternal Compression
Pressing sharply on the sternum while listening over the proximal end of the ETT to detect a characteristic feel and sound of expelled gases from the airway is occasionally used to distinguish esophageal from endotracheal intubation.16 This test is mistrusted by many because of (1) inability to distinguish gases expelled passing through the ETT from gases passing through or around a tube misplaced in the esophagus, (2) inability to distinguish gases being expelled through the nose, and (3) inability to distinguish esophageal and stomach gases present from prior mask ventilation.16
j Tube Condensation of Water Vapor
The basic principle of tube condensation as a sign of ETT placement is that water vapor seen in clear plastic ETTs is more likely to be present with gases exhaled through a tracheally placed tube than with gases emanating from the stomach through a tube in the esophagus (Fig. 32-2). Two studies have demonstrated water condensation in all cases in which ETTs were placed in the trachea.36,42 However, water condensation can and does occur when ETTs are placed in the esophagus. The fact that condensation was noticed in 85% of esophageal intubations in one study and in 28% in another study should strongly discourage its presence from being interpreted as a reliable indicator of a successful intubation.36,42

k Nasogastric Tubes, Gastric Aspirates, Introducers, and Other Devices
A test devised to distinguish between tracheal and esophageal placement of an ETT involves threading a lubricated NGT through the tube in question, applying continuous suction, and attempting to withdraw the NGT.43 This test exploits the distinguishing feature that the esophagus will collapse around the NGT when suction is applied, whereas free suction applied in the trachea will continue.
In a study of 20 patients in whom both trachea and esophagus were intubated, the ability to maintain suction and the ease of withdrawal during continuous suction clearly distinguished between the two positions.43 When the NGT was in the trachea, suction applied to it could be maintained easily because the trachea remained patent and air was entrained through the open end of the tube. This allowed the NGT to be withdrawn easily despite suctioning. In contrast, when suction was applied to the NGT in the esophagus, the esophageal wall collapsed around it, thereby obstructing suction and interfering with easy withdrawal of the NGT. Although the length of the NGT that could be easily inserted before an impediment or resistance was felt (5 to 15 cm distal to the tip of the tube) identified correct tracheal placement, it was less useful in identifying esophageal intubation. Similarly, the nature of the aspirate (mucus versus bile or gastric juice) was found to be of limited value in most patients. Because the total time spent to make these observations was 20 to 30 seconds, the authors concluded that the test is reliable.43 Despite their enthusiasm, this test is very rarely used because of the availability of better methods.
The Eschmann introducer is a 60-cm-long device (10 cm shorter than other similar devices) composed of two layers: a core of tube woven from Dacron polyester threads and an outer resin layer to provide stiffness, flexibility, and a slippery, water-impervious surface. Frequently, the device is referred to as a “gum elastic bougie”—despite the fact that it is not gum, not elastic, and not a bougie.44 The introducer has a 35-degree kink located 2.5 cm from its distal end. Because its outer diameter (OD) is 5 mm, it can be used with ETTs with an inner diameter (ID) of 6 mm or greater. The device has been used for many years to facilitate intubation and has been introduced to differentiate tracheal from esophageal intubation in emergencies when there is doubt about the ETT location.26 When inserted through the lumen of the ETT, the curved tip of the lubricated introducer may be felt rubbing over the tracheal rings, and resistance is encountered as the tip of the introducer meets the carina or a main stem bronchus at approximately 28 to 32 cm in the adult. If the ETT is in the esophagus, the introducer passes without resistance to the distal end of the esophagus or stomach.26 Forceful insertion of an excessive length of the introducer could conceivably result in bronchial rupture or other injuries. This has led the manufacturer to discourage its use as an ETT changer, because other devices specifically designed for this purpose are now available.45
l Transtracheal Illumination
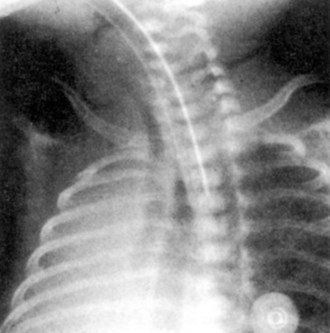
The success of transillumination of the soft tissues of the neck anterior to the trachea in accomplishing guided oral or nasal intubation has culminated in the development of improved lighted stylets and introducers (see Chapter 21).46–48 It has also prompted investigators to use transtracheal illumination to differentiate esophageal from tracheal ETT placement and to position the ETT accurately inside the trachea. Transmission of light through tissues depends on thickness, compactness, color, density, and light absorption characteristics of the tissue; wavelength, quality, and intensity of the light; proximity of the tissue to the light source; and the ambient lighting conditions in the room.49 Typically, endotracheal intubation with the lighted stylet or introducer inside the ETT or placement of the stylet in the lumen of the ETT after intubation gives off an intense, circumscribed, midline glow in the region of the laryngeal prominence and sternal notch (Fig. 32-3). The illumination is mostly seen opposite the thyrohyoid, cricothyroid, and cricotracheal membranes. In the event of esophageal intubation, the light is either absent or perceived as dull and diffuse.

To enhance transillumination, darkening the room, dimming the overhead lights, and applying cricoid pressure (to approximate the tracheal wall to the light source and stretch the soft tissues anterior to the light source) have been recommended.46–49 Newer lighted stylets or introducers, battery operated or incorporating a fiberoptic light source, have brighter lights than earlier prototypes. Consequently, dimming of the overhead lights or application of cricoid pressure may not be necessary. The reliability of transtracheal illumination in distinguishing esophageal from endotracheal intubation in adults has been demonstrated.49,50 In one study conducted on five cadavers, only 1 of 56 intratracheal placements was misidentified as esophageal, whereas of 112 extratracheal placements (esophageal or pyriform fossa), 1 was misidentified as intratracheal.50 In another study of 420 adult patients, tracheal transillumination was graded as excellent in 81% of patients and as good in the remaining 19%.49 In contrast, transesophageal illumination could not be demonstrated in any patient. Despite these reports, false-negative results (ETT in trachea but no transillumination) with the use of the newer lighted stylets and introducers in patients with neck swelling or dark skin and in obese patients have been noticed.31 Similarly, occasional false-positive results have been observed in thin patients. Nonetheless, the use of transillumination could reduce unrecognized esophageal intubations, especially outside the operating room where other technical aids are not available.49,50
Reports have delineated several complications with these transillumination devices.51–53 Loss of the bulb into the lung necessitating bronchoscopic removal has been reported.51 A change in design involving encasement of the bulb in a plastic retaining cover has virtually eliminated the possibility of this complication in future.47 Other reports have described arytenoid subluxation.52,53 However, this complication can occur after conventional intubation, and there is no evidence of an increased incidence with the use of lighted stylets.
m Pulse Oximetry and Detection of Cyanosis
Although unrecognized esophageal intubation ultimately leads to a severe fall in O2 saturation (and detectable cyanosis), minutes may elapse before this happens. A disturbing finding that emerged from the ASA closed claims study is that detection of esophageal intubation required longer than 5 minutes in 97% of cases.1 Furthermore, detectable cyanosis preceded the recognition of esophageal intubation in only one third of cases. Several factors contribute to the delay in diagnosing esophageal intubation by pulse oximetry or in detecting cyanosis, or both.
Reliance on the appearance of cyanosis as a clue to esophageal intubation can contribute to such a delay. Recognition of cyanosis usually necessitates the presence of more than 5 g/dL of reduced hemoglobin, which corresponds to 75% to 85% O2 saturation.54 The detection may also depend on the concentration and type of hemoglobin. With severe anemia, cyanosis may not be apparent until the arterial oxygen saturation (Sao2) falls to 60%. An infant with a high proportion of fetal hemoglobin may still look “pink” at an arterial partial pressure of oxygen (PaO2) near 40 mm Hg because of the increased blood affinity of O2 and leftward shifting of the fetal oxyhemoglobin dissociation curve; for this reason, a serious reduction in PaO2 may develop before cyanosis is apparent.55 Recognition of cyanosis is influenced by the limited exposure of the patient’s body and the insensitivity of the human eye to changes in skin color or even the color of the blood during arterial desaturation. It could also be affected by variations in room lighting and the color of the surgical drapes.
Noninvasive monitoring of oxygen saturation by pulse oximetry (SpO2) has proved to be a reliable indicator of Sao2.56,57 It is undoubtedly quicker to detect changes in SpO2 than to rely on clinical detection of cyanosis. The main limitation of pulse oximetry is that it does not measure PaO2, which may fall long before SpO2 is affected.
Preoxygenation of the patient’s lungs before anesthetic induction extends the period of time before a decrease in SaO2 occurs in case of esophageal intubation.58,59 In general, O2 deprivation or apnea after air breathing results in a substantial fall in PaO2 within 90 seconds, whereas PaO2, after O2 breathing, remains higher than 100 mm Hg for at least 3 minutes of apnea, and SaO2 does not change during this period.54,58 Consequently, pulse oximetry after preoxygenation does not immediately indicate that the esophagus has been intubated.59 Because of this prolonged interval with normal SpO2 being recorded initially after the intubation attempt, misplacement of the ETT may not be suspected later when SpO2 begins to decrease.1,59 Furthermore, the risk of misinterpretation of clinical findings suggestive of esophageal intubation may be greater when other clues such as decrease in SpO2 or cyanosis are not yet manifest.1 This “hazard” of preoxygenation has led a few clinicians to abandon such a practice so that esophageal intubation can be more readily appreciated.60 One does not need to go to such extremes as to abandon a practice that has definite merits. However, the presence of normal pulse oximetry readings after intubation should not be taken as evidence of successful endotracheal intubation, and after preoxygenation, oxyhemoglobin desaturation, as indicated by pulse oximetry, is a relatively late manifestation of esophageal intubation.1,13,59,61–63
Both O2 consumption and cardiac output can influence the Sao2 through their effects on mixed venous oxygen tension ( ) and mixed venous oxygen content (
) and mixed venous oxygen content ( ).54 A decrease in O2 consumption associated with anesthetic induction or an increase in cardiac output or both can lead to an increase in
).54 A decrease in O2 consumption associated with anesthetic induction or an increase in cardiac output or both can lead to an increase in  and
and  . The high
. The high  retards the decrease in PaO2 in the event of O2 deprivation resulting from esophageal intubation and consequently may delay its recognition. Conversely, in patients with low SaO2 and in those who have high O2 consumption (e.g., children, women in labor, morbidly obese patients) or decreased functional residual capacity (FRC), oxyhemoglobin desaturation may occur faster.
retards the decrease in PaO2 in the event of O2 deprivation resulting from esophageal intubation and consequently may delay its recognition. Conversely, in patients with low SaO2 and in those who have high O2 consumption (e.g., children, women in labor, morbidly obese patients) or decreased functional residual capacity (FRC), oxyhemoglobin desaturation may occur faster.
With the vocal cords open, manual ventilation into the esophagus can result in alveolar gas exchange. In 18 of 20 patients studied after intentional intubation of both the esophagus and the trachea, ventilation into the esophagus caused cyclic compression of the lungs by the distending stomach and esophagus, leading to some gas exchange evidenced by recording of carbon dioxide at the proximal end of the ETT.35 Although in this situation esophageal ventilation causes ventilation of the lungs with room air, it considerably delays the onset of cyanosis and oxyhemoglobin desaturation. Similarly, respiratory efforts by a spontaneously breathing patient through the unintubated trachea may delay the recognition of esophageal intubation. Esophageal ventilation may also be effective in yielding apneic oxygenation if the cords are open and there is a leak around the cuff of the misplaced esophageal tube.
n the Beck Airway Airflow Monitor
The Beck Airway Airflow Monitor (BAAM; Great Plains Ballistics, Lubbock, TX) consists of a cylindrical plastic whistle with a 2-mm-diameter aperture (Fig. 32-4). When connected to the proximal end of an ETT in a spontaneously breathing patient, the airflow is forced through the small lumen, producing a loud whistle.64 The pitch during inspiration and exhalation differs because of varying airflow velocities. The BAAM has been used to assist blind intubation and guide the ETT into the trachea. The loudness of the whistle indicates proximity to the tracheal air column, whereas cessation of the sound implies esophageal intubation, obstruction of the ETT, or excessive leak around the ETT. In patients who are not breathing spontaneously, a gentle squeeze of the chest produces whistling if the ETT is in the trachea. Because the whistle is produced by the airflow, an ETT in the pharynx can produce a whistle. Reports on this device have been limited to case reports and one study in neonates.64 More research is needed to determine its validity.

o Chest Radiography
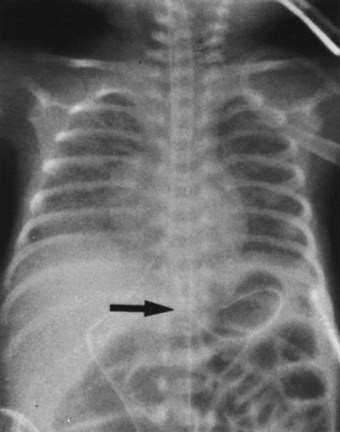
A chest radiograph can diagnose esophageal intubation if the ETT is located in the lower esophagus distal to the carina (Fig. 32-5).65 Because a tube in the esophagus is often projected over the tracheal air column on anteroposterior chest radiographs, the radiologic features of esophageal intubation are usually difficult to assess.63 However, it should be suspected in the following situations63,65:
• If any part of the border of the ETT is seen outside or lateral to the air column of the tracheobronchial tree (in the absence of a pneumomediastinum)
• In the presence of esophageal air and gastric distention, particularly if an NGT is in place
• If there is a noticeable deviation of the trachea caused by an overinflated cuff.
Although a lateral view of the chest could precisely reveal esophageal intubation, such views are often difficult to obtain. However, in one study, ETT location was identified correctly in 92% of the films taken with the patient in a 25-degree right posterior oblique position with the head turned to the right side.63 Because the esophagus is located slightly to the left as well as behind the trachea, this projection presents the relationship en face with respect to the radiologic beam, resulting in avoidance of superimposition of the trachea over the esophagus (Fig. 32-6). Because radiography is time-consuming and not failsafe, it should never be relied on for diagnosis of esophageal intubation, even in the critical care setting.
p Impedance Respirometry
Impedance respirometry, which measures electrical conductivity of the thorax, has been used to monitor respiratory rate in the critical care setting and to monitor apnea in infants. The ability of impedance respirometry to distinguish esophageal from endotracheal intubation has been explored.66,67 A high-frequency alternating current is passed between two electrodes placed on the anterior chest wall. With the increase in lung volume during inspiration, there is an associated decrease in lung electrical conductivity and therefore increased impedance.66,67 These changes can be measured and displayed as a waveform. If the esophagus is intubated, such an effect on thoracic impedance should be absent. Although assessment by thoracic impedance plethysmography was found to have 100% sensitivity in the detection of esophageal ETT placement in a study in adult patients,66 it correctly identified only 76 of 80 ETTs in children.67 Of those incorrectly identified, one was in the trachea and three were in the esophagus. Obviously, more studies are needed before any conclusions can be made. Although it is not a perfect test, use of impedance respirometry could decrease the time taken to identify incorrect placement when combined with other methods of ETT verification.67
2 Almost Failsafe Methods
a Identification of Carbon Dioxide in Exhaled Gas
The availability of capnometry (measurement of CO2 in expired gas) and capnography (instantaneous display of the CO2 waveform during the respiratory cycle) for intraoperative monitoring has prompted clinicians to extend their use to facilitate detection of esophageal intubation.35,68–71 The principle of use stems from the fact that exhaled CO2 can be reliably detected during controlled or spontaneous ventilation in patients with adequate pulmonary flow whose trachea is intubated, whereas no CO2 can be detected in gases emanating from an ETT in the esophagus.
Studies have revealed that the combined use of capnography and pulse oximetry could avert more than 80% of mishaps considered preventable.72 In an amendment to its original basic intraoperative monitoring standards, the ASA stated the following: “When an ETT is inserted, its correct positioning in the trachea must be verified by clinical assessment and by identification of CO2 in the expired gas. End-tidal CO2 (Etco2) analysis, in use from the time of ETT placement, is strongly encouraged.” (Standards for Basic Anesthetic Monitoring, 2003 Directory of Members, American Society of Anesthesiologists, Park Ridge, IL, p 493.) Identification of CO2 in the exhaled gas has emerged as the standard for verification of proper ETT placement. Furthermore, interruption of CO2 sampling in the exhaled gas due to disconnection, obstruction, accidental tracheal extubation, or total loss of ventilation is immediately detected. Two main methods are currently used: capnography and colorimetric detection of CO2.
Capnography
Currently available CO2 analyzers use various principles to measure CO2 in the inspired and exhaled gases on a breath-to-breath basis and display the CO2 waveform by mass spectrometry, infrared absorption spectrometry, or Raman scattering. A normal capnographic waveform in relation to the respiratory cycle is shown in Figure 32-7.73 A mass spectrometric tracing showing CO2 waveforms after esophageal intubation and after correct placement of the ETT in the trachea is shown in Figure 32-8. Although capnography typically distinguishes tracheal from esophageal intubation, false-negative results (i.e., ETT in trachea, absent waveform) and false-positive results (i.e., ETT in esophagus or pharynx, present waveform) have been reported.
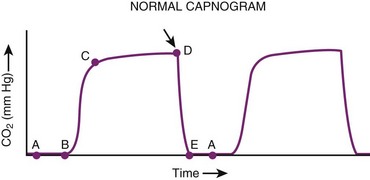
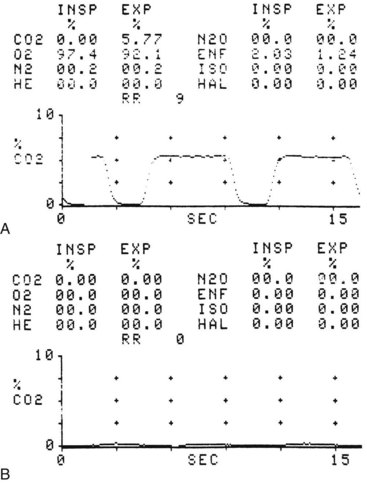
Figure 32-8 A, Normal capnograph, endotracheal tube (ETT) in trachea. B, Absent capnograph, ETT in esophagus.
Since the advent of capnography to confirm ETT placement, there have been reports of markedly different problems yielding unexpected false-negative results. For example, disconnection of the ETT from the breathing apparatus, apnea, and equipment failure may be misinterpreted as absent waveform caused by esophageal intubation.74 A kinked or obstructed ETT interferes with sampling of exhaled gas and may lead to an absent or distorted waveform. Lack of a CO2 waveform caused by severe bronchospasm has also been reported.74 Unintentional application of positive end-expiratory pressure (PEEP) to a loosely fitted or uncuffed ETT can cause exhaled gases to escape around the distal lumen of the tube and may result in a sampling error and absent waveform.75 In addition, dilution of exhaled gases by high fresh gas flow in a Mapleson D system when proximal sidestream sampling is used in infants weighing less than 10 kg leads to erroneous sampling.76,77 This problem can be corrected by distal sampling from the ETT, up to the 12 cm mark; by use of a mainstream sampling device; or by use of special ventilators.77 Lower sampling flow rates and gas sampling line leaks can result in artifactually low exhaled CO2 values and an abnormal waveform.78,79
Marked diminution of pulmonary blood flow increases the alveolar component of the dead space.54,70 Low cardiac output, hypotension, pulmonary embolism, pulmonary stenosis, tetralogy of Fallot, and kinking or clamping of the pulmonary artery during pulmonary surgery all cause a decrease in end-tidal carbon dioxide partial pressure (PETCO2), reflecting an increase in alveolar dead space.54,80,81 Other factors contributing to the increased alveolar dead space during anesthesia include patient age, large VT, use of negative phase during exhalation, short inspiratory phase, and presence of pulmonary disease.54,81 As a result of the widespread destruction of alveolar capillaries in patients with chronic obstructive pulmonary disease, an increased alveolar dead space ensues. An increase in alveolar dead space is manifested as a decrease in PETCO2 and an increase in the PaCO2 to PETCO2 difference (normally 0 to 5 mm Hg).54,81 If capnography alone is relied on to confirm ETT placement in patients who have a very large alveolar dead space, the low PETCO2 values might mislead the clinician into thinking that the ETT was not placed in the trachea.
An abrupt reduction in cardiac output reduces PETCO2 by two mechanisms: First, a reduction in venous return causes a decrease in CO2 delivered to the lungs, and second, the increase in alveolar dead space dilutes the CO2 from normally perfused alveoli, thus decreasing PETCO2.82–84 When cardiac arrest ensues, CO2 is no longer delivered to or eliminated through the lungs even if ventilation is adequate, and consequentially PETCO2 values exponentially decrease to remarkably low values (<0.5%). Ninety seconds after experimentally induced ventricular fibrillation, PETCO2 is usually decreased by 90%.85 Accordingly, a decision regarding the location of the ETT based on capnographic findings alone during cardiac arrest may lead to a misdiagnosis.
Experimental cardiac arrest demonstrated a remarkably high correlation between PETCO2, cardiac output, and coronary perfusion pressure during closed-chest precordial compression, during open-chest cardiac massage, and after resuscitation.86,87 Similar observations were reported during episodes of cardiac arrest in critically ill patients.86,87 The restoration of spontaneous circulation is heralded by a rapid increase in PETCO2 within 30 seconds. This overshoot in PETCO2, which is characteristic of successful resuscitation, may exceed the prearrest value and reflects washout of CO2 that has accumulated in venous blood and in tissues during circulatory arrest.86,88 In patients in whom resuscitative efforts fail to restore spontaneous circulation, PETCO2 remains low or even declines, whereas in those who eventually regain spontaneous circulation, PETCO2 reaches 19 mm Hg or higher. These observations suggest that capnography can be used for monitoring the adequacy of blood flow generated by precordial compression during cardiopulmonary resuscitation and can serve as a prognostic indicator of successful resuscitation.86,88
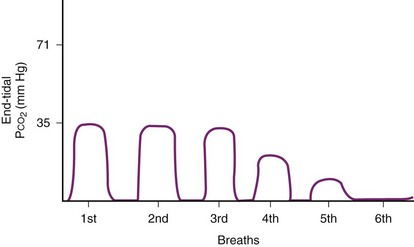
False-positive results can occur when the ETT is misplaced in the esophagus after exhaled gases are forced into the stomach during bag-mask ventilation preceding intubation attempts.85,89 If enough alveolar gas reaches the stomach, a CO2 concentration greater than 2% may be initially detected, and the CO2 waveform may be indistinguishable from that observed with endotracheal intubation.35,89,90 In fact, CO2 waveforms have been observed in one third of esophageal intubations,90 but repeated ventilation results in rapidly diminishing CO2 levels while the waveform becomes rather flat and irregular (Fig. 32-9).35,89 As a result of the dilution with successive ventilation, it is very unlikely that any CO2 would be detected after the sixth breath or after 1 minute in cases of esophageal intubation, making it easy to distinguish esophageal from endotracheal intubation.35 It has also been observed that compression of the chest caused clear, peaked CO2 elevation in 18 of 20 tracheally intubated patients but no changes in esophageal intubation.35 This simple, quick maneuver together with other signs can confirm proper ETT placement.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


