Fig. 37.1
Sensory distribution of the median nerve
The carpal tunnel is a fibro-osseous tunnel, which contains the flexor tendons of the fingers (tendons of the flexor digitorum profundus, flexor digitorum superficialis, and flexor pollicis longus) and the median nerve (Fig. 37.2). The volar border is covered by the flexor retinaculum, a broad ligament that extends from the tuberosities of the scaphoid and the trapezium to the pisiform and the hook of the hamate.
Fig. 37.2
Illustration of cross section across wrist
The median nerve lies superficial to the tendons of the flexor pollicis longus and medial to the flexor carpi radialis just before entering the carpal tunnel. However, the location of the median nerve can be more medial, and therefore blind injection may result in nerve injury.
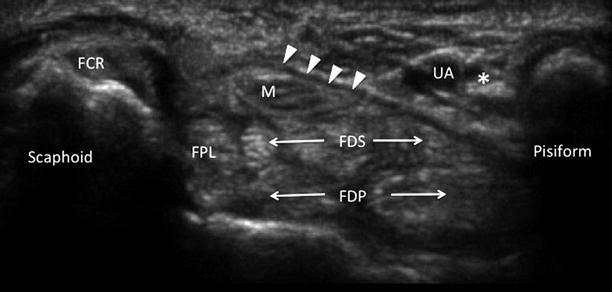
Ultrasound-Guided Carpal Tunnel Injection
The patient is in sitting position with the hand supinated resting on a pillow. The procedure is performed with sterile technique. A high-frequency linear ultrasound probe (6–13 MHz) is placed at the level of the pisiform and scaphoid tubercle. With the probe in this position, the ulnar artery, ulnar and median nerves should be visualized. The median is usually superficial and medial to the flexor pollicis longus (Fig. 37.3). A 1.5-inch, 25-G needle is inserted in-plane superficial and lateral to the ulnar artery toward the space between the median nerve and flexor retinaculum. Advancement of needle may be facilitated by hydrodissection with normal saline to release adhesion. A total volume of 2–3 mL of 1 % lidocaine mixed with 20–40 mg triamcinolone acetonide is sufficient. The patient is instructed to rest the hand over the next 24 h.