Cardiopulmonary Resuscitation
The cardiopulmonary physiology and pharmacology that form the basis of anesthesia practice are also applicable to treating the victims of cardiac arrest (Otto CW. Cardiopulmonary resuscitation. In: Barash PG, Cullen BF, Stoelting RK, Cahalan MK, Ortega R, Stock MC, eds. Clinical Anesthesia. Philadelphia: Lippincott Williams & Wilkins; 2013:1672–1700). (Please see Appendix C for American Heart Association [AHA] Resuscitation Protocols).
II. Scope of the Problem
Cardiopulmonary resuscitation (CPR) is systematic therapy that is aimed at sustaining vital organ function until natural cardiac function can be restored.
In clinical practice, the severity of underlying cardiac disease is the major determining factor in the success or failure of CPR.
Brain adenosine triphosphate is depleted in 4 to 6 minutes of no blood flow. It returns nearly to normal within 6 minutes of starting effective CPR.
Factors associated with poor outcomes are a long arrest time before CPR is begun, prolonged ventricular fibrillation without definitive therapy, and inadequate coronary and cerebral perfusion during cardiac massage.
Optimum outcome from ventricular fibrillation is obtained only if basic life support is begun within 4 minutes of arrest and defibrillation is applied within 8 minutes.
Blood flow decreases rapidly with interruptions of chest compressions (checking the pulse, intubation, defibrillation attempts, starting intravenous [IV] lines) and resumes slowly with reinstitution of compressions, emphasizing the importance of continued chest compressions in overall outcome.
III. Ethical Issues: Do not Resuscitate Orders in the Operating Room
The patient’s right to limit medical treatment, including refusing CPR (with a “do not resuscitate” [DNR] order) is
firmly established in modern medical practice based on the ethical principle of respect for patient autonomy.
Table 58-1 History of Cardiopulmonary Resuscitation
Bible story of Elisha breathing life back into the son of a Shunammite woman
Andreas Vesalius described tracheostomy and artificial ventilation in 1543
Teaching of resuscitation by the Society for the Recovery of Persons Apparently Drowned founded in London in 1774
Establishment of mouth-to-mouth ventilation as the only effective means of artificial ventilation in the 1950s by Elam, Safar, and Gordon
Successful use of the internal defibrillator in 1947
External defibrillation introduced in the late 1950s
Description by Kouwenhoven, Jude, and Knickerbocker of closed chest compression
Description by Redding and Pearson of the value of epinephrine
There are ethically sound arguments on both sides of the issue of whether DNR orders should be upheld in the operating room (OR).
A desire by the anesthesiologist or surgeon to suspend DNR orders during surgery is often based on the knowledge that nearly 75% of cardiac arrests in the OR are related to surgical or anesthetic complications and that resuscitation attempts are highly successful.
A mutual decision to suspend or limit a DNR order in the perioperative period may be achieved by communication among the patient, family, and caregivers.
Many interventions used commonly in the OR (mechanical ventilation, vasopressors, cardiac antidysrhythmics, blood products) may be considered forms of resuscitation in other situations. The only modalities that are not routine anesthetic care are cardiac massage and defibrillation.
Specific interventions included in a DNR status must be clarified with allowance made for methods necessary to perform anesthesia and surgery.
IV. Components of Resuscitation
The major components of resuscitation from cardiac arrest are airway, breathing, circulation, drugs, and electrical therapy (ABCDE). Traditionally, these have been divided into basic life support
(BLS) and advanced cardiac life support (ACLS) (Figs. 58-1 through 58-4). Recent advances in resuscitation (public access to automatic external defibrillators [AEDs]) have tended to blur the lines between BLS and ACLS.
(BLS) and advanced cardiac life support (ACLS) (Figs. 58-1 through 58-4). Recent advances in resuscitation (public access to automatic external defibrillators [AEDs]) have tended to blur the lines between BLS and ACLS.
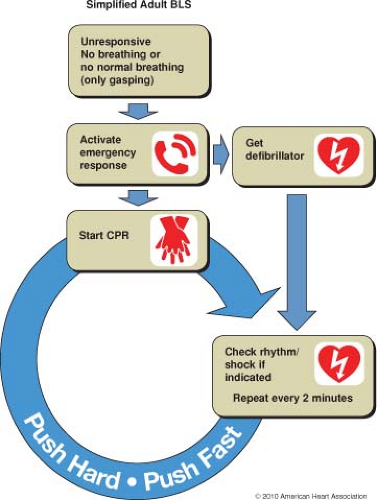 Figure 58-1. Simplified adult basic life support (BLS) algorithm. (From 2010 American Heart Association Guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2010; 122(suppl 3):S687, with permission.) |
Airway Management. The techniques used for airway maintenance during anesthesia are also applicable to cardiac arrest victims (Table 58-2).
Foreign body airway obstruction must be considered in any person who suddenly stops breathing and becomes
cyanotic and unconscious. (This occurs most commonly during eating and is usually caused by food, especially meat, impacting in the laryngeal inlet, at the epiglottis, or in the vallecula).
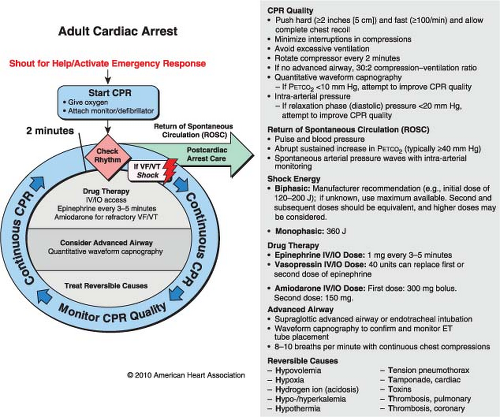
Figure 58-2. Advanced cardiac life support (ALCS) circular algorithm. (From 2010 American Heart Association Guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2010; 122(suppl 3):S737, with permission.)
The signs of total airway obstruction are the lack of air movement despite respiratory efforts and the inability of the victim to speak or cough.
Treatment is the abdominal thrust maneuver (chest thrusts are an alternative for parturients and massively obese individuals) and the finger sweep.
In an awake victim, the rescuer reaches around the victim from behind, placing the fist of one hand in the epigastrium between the xiphoid and umbilicus. The fist is grasped with the other hand and pressed into the victim’s epigastrium with a quick upward thrust. If the first attempt is unsuccessful, repeated attempts should be made because hypoxia-related muscular relaxation may eventually allow success.
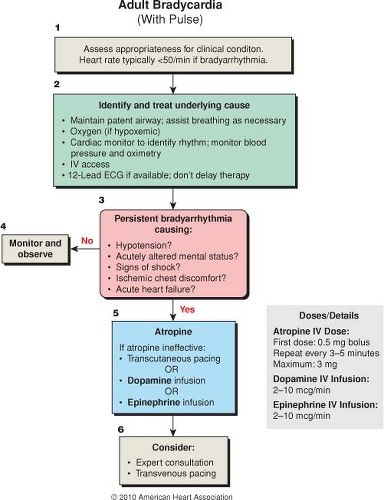
Figure 58-3. Adult bradycardia (with pulse) algorithm. (From 2010 American Heart Association Guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2010; 122(suppl 3):S749, with permission.)
Ventilation. When ventilation is provided in the rescue setting, mouth-to-mouth or mouth-to-nose ventilation is the most effective immediately available method. Although inspired gas with this method contains only about 17% oxygen and nearly 4% carbon dioxide (composition of exhaled air), it is sufficient to maintain viability.
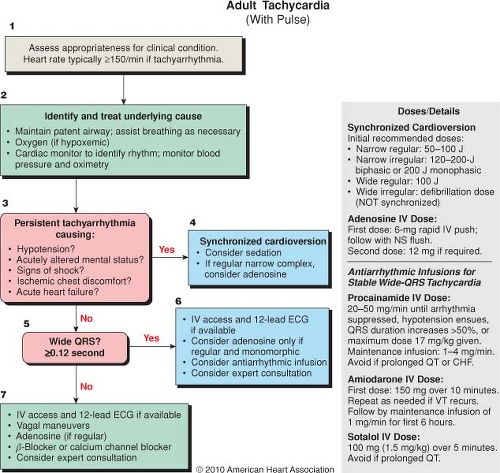
Figure 58-4. Adult tachycardia (with pulse) algorithm. (From 2010 American Heart Association Guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2010; 122(suppl 3):S751, with permission.)
Table 58-2 Techniques Used for Airway Maintenance During Cardiopulmonary Resuscitation
Head tilt and chin lift: The head is extended by pressure applied to the brow while the mandible is pulled forward by pressure on the front of the jaw, lifting the tongue away from the posterior pharynx
Jaw thrust: Applying pressure behind the rami of the mandible
Oropharyngeal or nasopharyngeal airway: Danger of inducing vomiting or laryngospasm in a semiconscious victim
Tracheal intubation: Should not be performed until adequate ventilation and chest compression have been established
Alternatives to tracheal intubation
Laryngotracheal mask airway
Airway Combitube
Translaryngeal ventilation
Tracheostomy
Physiology of Ventilation During Cardiopulmonary Resuscitation
Avoiding gastric insufflation requires that peak inspiratory airway pressures remain below esophageal opening pressure (∼20 cm H2O). Partial airway obstruction by the tongue and pharyngeal tissues is a major cause of increased airway pressure contributing to gastric insufflation during CPR. Properly applied pressure to the anterior arch of the cricoid (Sellick maneuver) causes the cricoid lamina to seal the esophagus and can prevent air from entering the stomach at airway pressures up to 100 cm H2O.
Achievement of an acceptable tidal volume during low inspiratory pressures characteristic of rescue breathing requires a slow inspiratory flow rate and long inspiratory time (breaths over 1.5–2.0 seconds during a pause in chest compressions).
Techniques of Rescue Breathing (Table 58-3)
Circulation
Physiology of Circulation During Closed Chest Compression. Two theories of the mechanism of blood flow during closed chest compression have been suggested. The mechanism that predominates varies from victim to victim and even during the resuscitation of the same victim.
Table 58-3 Techniques of Rescue Breathing
Mouth-to-mouth ventilation: The rescuer delivers exhaled air to victim, and exhalation by the victim is passive
Mouth-to-nose ventilation
Oropharyngeal airway with an external extension mouthpiece (it is often difficult to obtain a good mouth seal)
Mouth-to-mask ventilation: The mask may include one-way valve to direct the victim’s exhaled gases away from the rescuer and a side port for delivery of supplemental oxygen
Self-inflating resuscitation bag
Tracheal intubation: After placement of the tracheal tube, no pause should be made for ventilation because blood flow during CPR decreases rapidly when chest compressions are stopped
CPR = cardiopulmonary resuscitation.
The cardiac pump mechanism proposes that pressure on the chest compresses the heart between the sternum and spine. Compressions increase the pressure in the
ventricular chambers (closing the atrioventricular valves) and eject blood into the lungs and aorta. During the relaxation phase of closed chest compression, expansion of the thoracic cage causes a subatmospheric intrathoracic pressure, facilitating blood return.
The thoracic pump mechanism proposes that the increase in intrathoracic pressure caused by sternal compressions forces blood out of the chest (backward flow into veins is prevented by valves) with the heart acting as a passive conduit.
Distribution of Blood Flow During Cardiopulmonary Resuscitation. Cardiac output is decreased between 10% and 33% of normal during CPR, and nearly all the blood flow is directed to organs above the diaphragm. (Abdominal viscera and lower extremity blood flow are decreased to <5% of normal.)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








