Cancer Pain
Pain management is of particular importance in cancer patients. Extensive research has shown that pain is the symptom that cancer patients fear most. Up to 50% of patients undergoing cancer treatment and up to 90% of patients with advanced cancer have debilitating pain.1 Effectively managing your patients’ pain will dramatically improve their quality of life while enduring cancer treatment. Though the top priority is to cure or put the cancer in remission, proper pain management should be provided concurrently from the beginning of treatment. This chapter will help you do that, your goal being to develop a regimen that prevents baseline pain and is flexible enough to treat breakthrough pain. Breakthrough pain is defined as episodic exacerbations of pain above the established baseline.2 Both the medical and procedural management of cancer pain will be reviewed here.
The first step in setting up a proper pain plan is to determine all potential individual sources of pain. I say “sources” in the plural as a cancer patient commonly may have more than one type of pain. Both the cancer itself and its treatment can cause pain. The patient’s type of cancer, location of the pain, how the pain feels (electric, dull, sharp), and treatments administered (chemotherapy, radiation therapy, surgery) will help you identify the pain generators. Once you have established the pain generators, determine the severity of each instance. In terms of pain, the focus should be on how functional the patient is. Does the patient have trouble walking or dressing because of pain? Does the pain medication affect mental status? The following list provides the most common pain generators in cancer patients; it is not all consuming but touches on the most prevalent.
Metastatic Bone Pain
The most common cause of pain in cancer patients is bone metastases—70% of patients with bone metastasis have bone pain. The pain is caused by stretching of the periosteum (the membrane that lines the outer surface of all bones; Fig. 3-1) and nerve irritation in the endosteum (the tissue lining the medullary cavity of the bone; see Fig. 3-1). If you have ever been kicked in the shin, you have an understanding of what bone pain feels like.
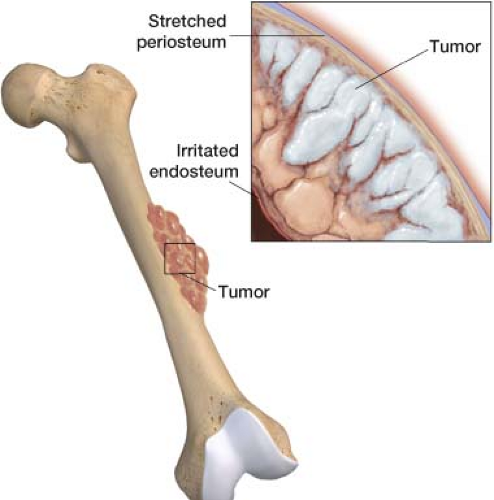 Figure 3-1 Metastatic bone pain: Stretching of the periosteum, irritation of the endosteum. |
When evaluating any patient with cancer pain it is necessary to consider bone metastasis. The patient may have pain from metastatic bone destruction from a lung primary or possibly a pathologic fracture. Cancers that tend to metastasize to the bone are: Breast, lung, thyroid, kidney, and prostate. The ribs, pelvis, and spine are normally the first bones involved. Pathologic fractures are common in breast cancer due to the lytic nature of the lesions. They are less common in lung cancer due to short life span and rare in prostate cancer, which tends to involve osteoblastic lesions.
Imaging can help you confirm your diagnosis of metastatic bone pain. A bone scan is very sensitive in detecting osseous metastases and is recommended as the imaging study of choice. Laboratory studies should be performed as well to identify anemia, thrombocytopenia, and hypercalcemia that can be seen with metastatic bone disease.
Visceral Pain
Visceral pain (internal organ pain) occurs when pain fibers around organs are activated. Tumors cause pain by invasion, obstruction, distension, or compression of an organ (Fig. 3-2). Organs that are hollow are more likely to be painful than solid organs. Hollow organs include the uterus, ureter, fallopian tubes, colon, rectum, stomach, bladder, bile duct, and gallbladder. Visceral pain is not well localized—patients often complain of a deep, gnawing, or dull pain of unspecified location. This is because there are a small number of visceral afferent nerves covering a large area. Visceral pain can be referred to the back, groin, or shoulder. Pancreatic and uterine cancers are especially known for their painful attack of abdominal/pelvic organs.
Neuropathic Pain
Neuropathic pain in cancer patients is often not caused by the cancer itself; instead, it may be a side effect of treatment.
Chemotherapy
Chemotherapy can cause a painful sensory neuropathy (Fig. 3-3). Patients often describe this neuropathy as a burning electric pain in the distal extremities. The symptoms usually begin during chemotherapy but may have a delayed onset. Three of the most common offending agents are vincristine (used for hematologic cancer), cisplatin, and paclitaxel (used for breast and ovarian cancer).1,3
Radiation
Targeted radiation used to treat cancer can also cause neuropathic pain (Fig. 3-4). Radiation injury to the brachial or lumbosacral plexus can occur with direct exposure. The mechanism of radiation-induced neuropathy may be related to a combination of localized ischemia and subsequent fibrosis due to microvascular insufficiency. Radiation injury to the plexus may present 1 to 30 years following radiation treatment. For the brachial plexus, pain is commonly described as aching in the shoulder or hand. Other symptoms include paresthesia in the lateral fingers or entire hand. For the lumbosacral region, presenting symptoms include weakness of the legs associated with sensory symptoms, paresthesia, and numbness. Weakness starts distally in the L5 to S1 segments and slowly progresses. Magnetic Resonance Imaging (MRI) and/or Electromyography (EMG) can help establish the diagnosis. MRI features suggestive of radiation-induced plexopathy include diffuse, uniform, symmetric swelling, and T2 hyperintensity of the plexus as compared to nonuniform, asymmetric, focal enlargement, and the presence of a mass with postcontrast enhancement, which is indicative of tumor recurrence. The EMG feature suggestive of radiation-induced plexopathy is myokymia. Myokymia is a brief spontaneous tetanic contraction of motor units or groups of muscle fibers.
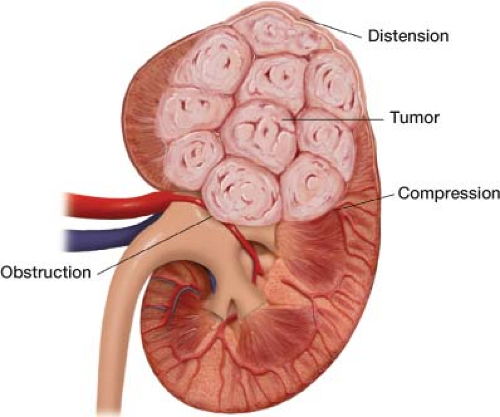 Figure 3-2 Visceral pain, internal organ pain. Pain is caused by invasion, obstruction, distension, or compression of an organ. |
Headache
Metastatic brain tumors are more common than primary brain tumor with lung cancer being the main source. Meningiomas are the most common primary brain tumor and are typically benign. While gliomas (tumor arising from glial cells) represent 80% of all malignant primary brain tumors. Parenchymal brain tissue has no pain receptors; pain is generated when vessels and/or the meninges are stretched by a mass
(Fig. 3-5). The meninges and blood vessels are innervated by both cervical and cranial (primarily trigeminal) nerves. Headache due to tumor is typically worse in the morning, and may be accompanied by vomiting, confusion, double vision, numbness, or weakness. The headache can worsen with increase of intracranial pressure as a result of sneezing or a bowel movement. Cancer patients with a long history of headache pre dating the cancer who present with different headache symptoms are of a great concern. On ophthalmoscopic examination, if the intracranial pressure is raised enough, bilateral papilledema and optic disc swelling can be seen.
(Fig. 3-5). The meninges and blood vessels are innervated by both cervical and cranial (primarily trigeminal) nerves. Headache due to tumor is typically worse in the morning, and may be accompanied by vomiting, confusion, double vision, numbness, or weakness. The headache can worsen with increase of intracranial pressure as a result of sneezing or a bowel movement. Cancer patients with a long history of headache pre dating the cancer who present with different headache symptoms are of a great concern. On ophthalmoscopic examination, if the intracranial pressure is raised enough, bilateral papilledema and optic disc swelling can be seen.
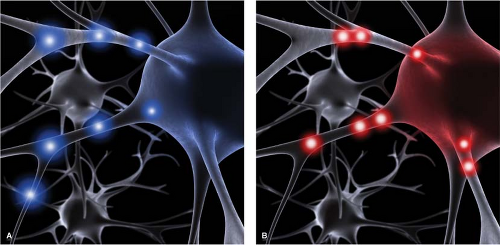 Figure 3-3 Chemotherapy-induced peripheral nerve dysfunction. A. Nerves send impulses in a regular controlled pattern. B. When nerves are injured they fire aberrantly which is interpreted by the brain as burning, electric neuropathic pain. |
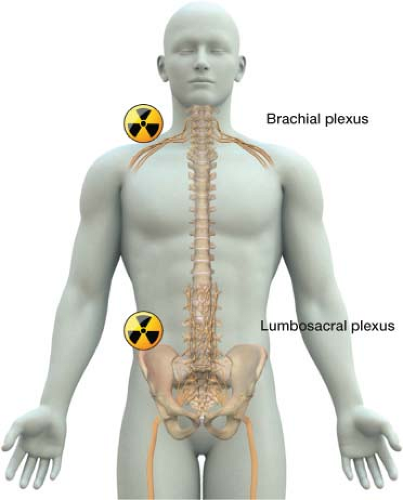 Figure 3-4 Radiation-induced neuropathic pain. Brachial plexopathy and lumbosacral plexopathy. |
Spinal Cord Compression due to Tumor
Spinal cord compression occurs in roughly 2% to 5% of cancer patients. A tumor produces edema, inflammation,
and mechanical compression, with direct neural injury to the cord, as well as vascular damage and impairment of oxygenation (Fig. 3-6). Patients present with acute back pain and neurologic deficits in the lower extremities, which may include sensory changes and/or weakness. They also may present with bowel or bladder incontinence. This is a neurologic emergency, as patient outcomes can often be determined by the care provided in the first hours of onset. Treatment guidelines are covered in the latter part of this chapter.
and mechanical compression, with direct neural injury to the cord, as well as vascular damage and impairment of oxygenation (Fig. 3-6). Patients present with acute back pain and neurologic deficits in the lower extremities, which may include sensory changes and/or weakness. They also may present with bowel or bladder incontinence. This is a neurologic emergency, as patient outcomes can often be determined by the care provided in the first hours of onset. Treatment guidelines are covered in the latter part of this chapter.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


