Fig. 26.1
The three stages of calcification (Reproduced with permission from Philip Peng Educational Series)
Precalcific Stage
During the precalcific stage, fibrocartilaginous metaplasia of the matrix takes place where the tenocytes becomes chondrocytes. The patient is essentially asymptomatic.
Calcific Stage
It is further divided into three phases. In the formative phase, calcium deposit appearing like chalk develops around the chondrocytes within the fibrocartilaginous matrix. After a variable period of inactivity (resting phase), the disease progresses to the resorptive phase where cell-mediated resorption takes place. At this phase, vascular channels develop at the periphery of the calcification. Migration of macrophages and multinucleated giant cells soon removes the calcium deposit by phagocytosis.
In the formative and resting phases, many patients are asymptomatic if the hard calcium deposit is not large enough to induce impingement syndrome. These calcifications tend to be well circumscribed and discrete when examined radiographically and often produce significant acoustic shadowing by ultrasound scan (Fig. 26.2). It is difficult to aspirate the calcifications in these two phases because the calcifications are quite hard and chalk-like. Most common indication of lavage at this stage is calcification over 1 cm in diameter, which commonly causes impingement syndrome.

Fig. 26.2
Sonography of the calcium deposit in hard calcific phase. The arrows indicate the calcification. Note the anechoic shadow cast by the calcium (Reproduced with permission from Philip Peng Educational Series)
In the resorptive phase, the calcium deposit is usually soft with toothpaste-like consistency but it is the most symptomatic phase. Shedding of calcium crystals into the adjacent subacromial bursa may result in severe acute pain and restricted range of motion. This phase typically lasts for 2 weeks or longer. These calcifications appear ill-defined on radiographs, producing little or no acoustic shadowing by ultrasonography (Fig. 26.3). This stage is the most common indication for ultrasound-guided intervention.
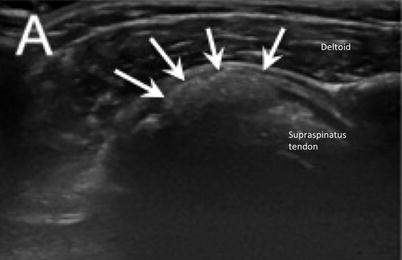
Fig. 26.3
Sonography of the calcium deposit in soft calcific phase. The arrows indicate the calcification. Note the minimal echogenic shadow cast by the calcium (Reproduced with permission from Philip Peng Educational Series)
Post-calcific Stages
The granulation tissue with fibroblasts and vascular channels grows into the location previously occupied by the calcification and replaces the calcification. The tendon undergoes fibrosis and eventual repair.
Dystrophic calcification is not included in the entity of calcific tendinopathy and is not a candidate for this procedure. This occurs in degenerative tissue and does not heal spontaneously. This is in contrast to the calcific tendinosis, which occurs in healthy tissue, is cell mediated, and is self-limiting.
Ultrasound-Guided Intervention for Calcific Tendinitis
Patient Preparation
The patient is placed in semi-reclined position in the modified Crass position (hand is placed on the ipsilateral hip with the palm against the body). A linear array ultrasound transducer (6–13 MHz) is positioned to show the long axis of the supraspinatus tendon and its insertion onto the greater tuberosity. To better appreciate the size, consistency, and shape of the calcium deposit in the supraspinatus tendon, at least two orthogonal planes (long and short axes) should be viewed [4]. With the ultrasound showing the long axis of supraspinatus tendon, a 25-gauge needle is inserted in-plane providing generous infiltration with lidocaine to the subcutaneous tissue, deltoid muscle, and subacromial bursa.
Fenestration
Single Needle Technique
An 18-gauge needle is advanced in-plane to fenestrate the calcium deposit (Fig. 26.4) [6]. Initially, the physician may encounter stiff resistance as the needle fractures the dense calcium. Rotating the needle will enhance fenestration (Fig. 26.5). With multiple “passes” throughout the deposit, the resistance will diminish as the deposit is fractured into smaller pieces. Care should be taken to avoid breaking the rim of the deposit.
Fig. 26.4




Needle insertion into the center of calcium (outlined by arrows) with in-plane method (Reproduced with permission from Philip Peng Educational Series)
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
