Bag-Mask Ventilation
Steven C. Carleton
Robert F. Reardon
Calvin A. Brown III
Bag-mask ventilation (BMV) is a foundational skill in airway management. BMV is a consideration in every airway intervention, and evaluation for potential difficulty in bagging is a fundamental component of every airway assessment. Effective BMV reduces both the urgency to intubate and the anxiety that accompanies challenging laryngoscopy and intubation, buying time as one works through the potential solutions for a difficult or failed airway. The confident application of BMV is particularly critical when muscle relaxants are used to facilitate intubation; competence with BMV should be considered a prerequisite to using paralytic agents for this purpose. The ability to oxygenate and ventilate a patient with a bag and mask effectively eliminates the “can’t oxygenate” portion of the can’t intubate, can’t oxygenate scenario (see Chapter 2), leaving three unsuccessful attempts at intubation, or a failed best attempt after induction and paralysis in the “forced to act” scenario as the only pathways to a failed airway.
In spite of its importance, there is a paucity of literature that adequately describes effective BMV. Most health care providers mistakenly think that they are proficient at it, and it is given less attention in many airway texts and courses than are more glamorous, but less frequently applied, airway techniques. Nonetheless, BMV is among the most difficult airway skills to master, requiring a clear understanding of functional airway obstruction, familiarity with the required equipment, mechanical skill, teamwork, and an organized approach when initial efforts are suboptimal.
Successful BMV depends on three factors: (1) a patent airway, (2) an adequate mask seal, and (3) proper ventilation. A patent airway permits the delivery of appropriate tidal volumes with the least possible positive pressure. Basic methods for opening the airway include head extension, and the chin lift and jaw thrust maneuvers. Creating an adequate mask seal requires an understanding of the design features of the mask, the anatomy of the patient’s face, and the interrelationship between the two. Proper ventilation involves delivering an appropriate volume at a rate and force that minimize gastric insufflation and the potential for breath stacking and barotrauma.
The specific type of bag used is critically important. Self-inflating bags are useful in the emergency situation because of their low cost and simplicity. The bags vary in volume depending on their intended use, with adult bags typically having a volume of 1,500 ml, whereas those for children and infants have volumes of 500 and 250 ml, respectively. Bags that minimize dead space, incorporate unidirectional inspiratory and expiratory airflow valves, and have an oxygen reservoir are essential to optimize oxygenation during BVM (see Chapter 5). Bags with a pop-off pressure valve minimize the potential for barotrauma; most with this feature allow the valve to be manually disabled when high pressures are required for ventilation.
Face masks for BMV in the emergency department and prehospital setting are usually disposable, plastic models. Three sizes (small, medium, and large) are sufficient to accommodate most adults and school-aged children. Choice of size is empiric. Smaller masks are available for use in toddlers, infants, and newborns. A selection of face masks is shown in Figure 9-1. Note that it is generally easier to establish an adequate mask seal if the mask is too large than if it is too small because the mask must cover both the mouth and nose. A typical mask consists of three components:
A round orifice that fits over the standard 22-mm outside diameter connector on the bag assembly.
A hard shell or body; this is often clear, to allow continuous monitoring of the patient’s mouth and nose for regurgitation.
A circumferential cushion or inflatable cuff, which evenly distributes downward pressure onto the patient’s face, filling irregular contours and promoting an effective seal.
Although newer, ergonomically designed face masks may be more effective in reducing mask leaks than standard, disposable face masks, such masks are not widely available and have yet to be evaluated in the emergency clinical setting.
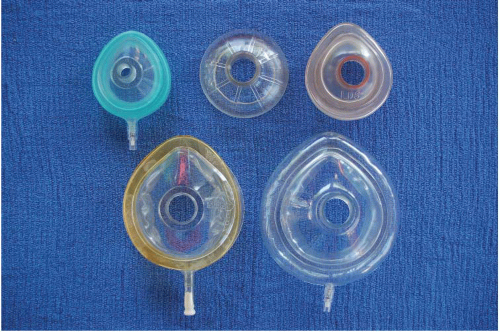 Figure 9-1 • Face masks of various types in sizes from infant to large adult. |
OPENING THE AIRWAY
The airway should be opened before placing the mask on the face. Functional occlusion of the airway is common in supine, obtunded patients, particularly when neuromuscular blocking agents have been given. This results from posterior displacement of the tongue into the oropharynx as the supporting mandible and hyoid bone relax, but also may result from occlusion of the hypopharynx by the epiglottis, or circumferential collapse of the pharynx as supporting muscles relax. Airway collapse is exacerbated by flexion of the head on the neck, and by opening the mouth. Maneuvers to open the airway are directed at counteracting these conditions by anterior distraction of the mandible and hyoid. The head tilt/chin lift is an initial maneuver that may be used in any patient in whom cervical spine injury is not a concern. In this technique, the clinician applies downward pressure to the patient’s forehead with one hand while the index and middle fingers of the second hand lift the mandible at the chin, pulling the tongue from the posterior pharynx, and slightly extending the head on the neck. Airway caliber may be augmented by coupling atlanto-occipital extension with slight flexion of the lower cervical spine (i.e., the “sniffing position”) similar to positioning for direct laryngoscopy (see Chapter 12). Although chin lift may be sufficient in some patients, the jaw thrust maneuver more effectively displaces the tongue anteriorly with the mandible and hyoid, minimizing its obstructing potential. The jaw thrust is achieved by forcibly and fully opening the mouth to translate the condyles of the mandible out of the temporomandibular joints, then pulling the mandible forward (Fig. 9-2A-D). This is most easily accomplished from the head of the bed, by placing the fingers of both hands on the body, angle, and ramus of the mandible with the thumbs on the mental processes. The forward position of the mandible can be maintained, and anterior traction on the hyoid and tongue can be increased, by closing the mandible on the bite-block of an oropharyngeal airway (OPA). It is useful to think of the jaw thrust maneuver as “creating an underbite,” with the bottom incisors placed anterior to the upper incisors. The fingers maintain the thrusted position while the mask is applied to the face. The jaw thrust is the safest first approach to opening the airway of a patient with a potential cervical spine injury; properly performed, it can be accomplished without moving the head or neck. Jaw thrust should also be
applied in any patient where chin lift and head tilt incompletely open the airway. The effectiveness of these airway maneuvers has been substantiated in multiple studies. Reduced emphasis on the jaw thrust technique in advanced cardiac life support is intended to lessen the complexity of CPR for laypersons, rather than representing opposition to its use.
applied in any patient where chin lift and head tilt incompletely open the airway. The effectiveness of these airway maneuvers has been substantiated in multiple studies. Reduced emphasis on the jaw thrust technique in advanced cardiac life support is intended to lessen the complexity of CPR for laypersons, rather than representing opposition to its use.
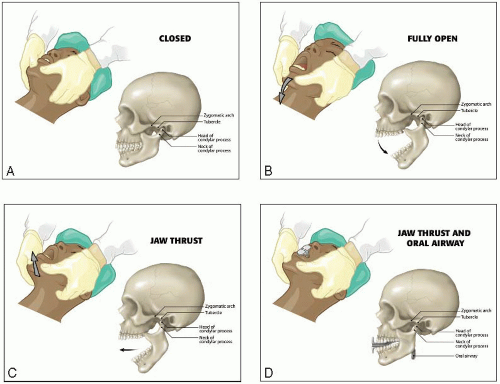 Figure 9-2 • Relieving upper airway obstruction by “creating an underbite” with the jaw thrust maneuver. This is the most important technique for opening and maintaining the airway. A: From the head of the bed, the closed mandible is grasped between the thumbs and fingers of both hands. B: The mandible is widely opened. C: The open mandible is displaced anteriorly out of the temporomandibular joint. D: The mandible is closed on the bite block of an OPA to maintain the jaw thrust with the lower teeth in front of the upper teeth. |
ORAL AND NASAL PHARYNGEAL AIRWAYS
Once an open airway has been established, it must be maintained. OPAs and nasopharyngeal airways (NPAs) are important adjuncts in achieving this goal. Both prevent the tongue from occluding the airway and provide an open conduit for ventilation. OPAs are available in a variety of lengths, measured in centimeters (Fig. 9-3A). They are intended to extend from the central incisors to just short of the epiglottis and posterior pharyngeal wall. The appropriate size can be estimated by choosing an OPA that extends from the lips to just beyond the angle of the mandible when held alongside the face. Sizes from 8 to 10 cm suffice for the majority of adults. Two methods of insertion are in common use. In one, the OPA is inserted into the open mouth in an inverted position with its tip sliding along the palate. As the insertion is completed, the OPA is rotated 180° into its final position with the flange resting against the lips. This method is designed to minimize the likelihood of the OPA impinging the tongue and displacing it posteriorly. In the second method,
the tongue is pulled forward with a tongue blade or laryngoscope blade, and the OPA is inserted in its normal orientation until the flange rests against the lips. The latter technique has less potential for causing trauma to oral structures but requires additional hands and equipment. NPAs are available in various sizes based on internal luminal diameter (Fig. 9-3B). Sizes from 6 to 8 mm accommodate most adult patients. The appropriate size is commonly stated as the diameter of the patient’s small finger, or 0.5 to 1.0 mm smaller than the endotracheal tube size for the patient, but neither method of estimation has been validated. For the purpose of augmenting BMV while minimizing the potential for nasal trauma, the smallest effective tube should be used; generally, this is 6 mm in adult females and 7 mm in adult males. When time permits, the larger nostril should be chosen based on inspection, and decongested with oxymetazoline or neosynephrine spray. Topical anesthesia spray, such as 4% lidocaine, also can be applied. A generously lubricated NPA is then inserted through the inferior nasal meatus parallel to the palate until the flange rests at the nostril. A slight rotatory motion during insertion may facilitate passage. If resistance is met, the tube should either be downsized, or insertion should be attempted through the contralateral nostril. An NPA should never be forced when resistance is encountered, as bleeding almost inevitably results. Relative contraindications to NPA insertion should be observed, including bleeding diathesis and suspected traumatic disruption of bony cranial floor structures.
the tongue is pulled forward with a tongue blade or laryngoscope blade, and the OPA is inserted in its normal orientation until the flange rests against the lips. The latter technique has less potential for causing trauma to oral structures but requires additional hands and equipment. NPAs are available in various sizes based on internal luminal diameter (Fig. 9-3B). Sizes from 6 to 8 mm accommodate most adult patients. The appropriate size is commonly stated as the diameter of the patient’s small finger, or 0.5 to 1.0 mm smaller than the endotracheal tube size for the patient, but neither method of estimation has been validated. For the purpose of augmenting BMV while minimizing the potential for nasal trauma, the smallest effective tube should be used; generally, this is 6 mm in adult females and 7 mm in adult males. When time permits, the larger nostril should be chosen based on inspection, and decongested with oxymetazoline or neosynephrine spray. Topical anesthesia spray, such as 4% lidocaine, also can be applied. A generously lubricated NPA is then inserted through the inferior nasal meatus parallel to the palate until the flange rests at the nostril. A slight rotatory motion during insertion may facilitate passage. If resistance is met, the tube should either be downsized, or insertion should be attempted through the contralateral nostril. An NPA should never be forced when resistance is encountered, as bleeding almost inevitably results. Relative contraindications to NPA insertion should be observed, including bleeding diathesis and suspected traumatic disruption of bony cranial floor structures.
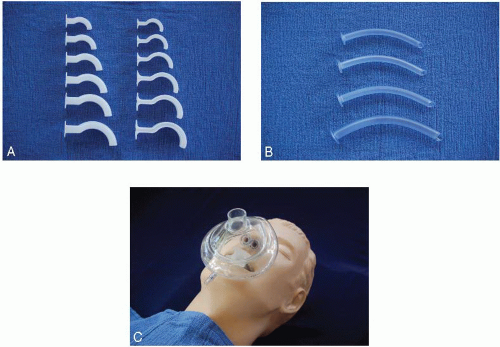 Figure 9-3 • A: Guedel (left) and Berman (right) OPAs. B: NPAs. C: OPA and two NPAs in place within the body of the mask to optimize airway maintenance. |
OPAs generally facilitate airway maintenance more reliably than NPAs, but OPAs are tolerated poorly in patients with intact gag and cough reflexes. Use of an NPA, particularly when time permits topical anesthesia of the nose, may be tolerated in this circumstance. When airway patency during BMV is difficult to maintain with an OPA, it can be supplemented by one, or even two, NPAs (Fig. 9-3C). The following cannot be stated strongly enough: At a minimum, an OPA should be inserted whenever BMV is used to support oxygenation and ventilation in an unresponsive patient and, absent contraindications, an NPA should be strongly considered when supporting respirations by BMV in a responsive patient, or to augment airway maintenance with an OPA.
POSITIONING AND HOLDING THE MASK
Once the airway is opened, the mask is placed to obtain a seal on the face. This should be accomplished with the mask detached




Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
