TOPICS
INTRODUCTION
Anesthesiologists are often involved in various aspects of care on a labor and delivery unit. However, the anesthesiologist’s primary responsibility is to provide care to the mother, particularly during an anesthetic for cesarean or complicated vaginal delivery. Thus, on a labor and delivery unit, at least one person other than the members of surgical team should be qualified to provide neonatal resuscitation and be immediately available to assume responsibility for resuscitation of the depressed newborn.1 Because the primary responsibility of the obstetrician and anesthesiologist is care of the mother, these individuals may not be able to shift care from the mother to the newborn. For the anesthesiologist, this may even be the case when the patient has a neuraxial anesthetic that is functioning adequately.1 However, the anesthesiologist should offer assistance in situations including management of a difficult neonatal airway or during the absence of a designated qualified individual for resuscitation. The benefit to the child must be weighed against the risk to the mother in these special circumstances.2 In the majority of situations, after assisted vaginal delivery or cesarean section, the mother is stable; therefore, if there is a need for neonatal resuscitation, the anesthesiologist should be available to help. In certain institutions, there may be an anesthesia care team caring for the mother (eg, an attending and a resident or fellow, or a nurse anesthetist). If the mother is stable, one member of this team may be free to help care for the neonate. It is important to keep in mind that soon after delivery the mother is undergoing tremendous physiologic changes and maternal status may change quickly. It still remains a judgment call for the anesthesiologist in charge to determine where his or her priorities lie—caring for either the mother or the newborn or caring for both.
History
Neonatal resuscitation has come a long way since the days of swinging the infant upside down and dilating the rectum with a raven’s beak back in the 19th century.3 Figure 11-1 is an illustration, reputedly of Dr. Bernhard Schultze himself, demonstrating the Schultze method of neonatal resuscitation.
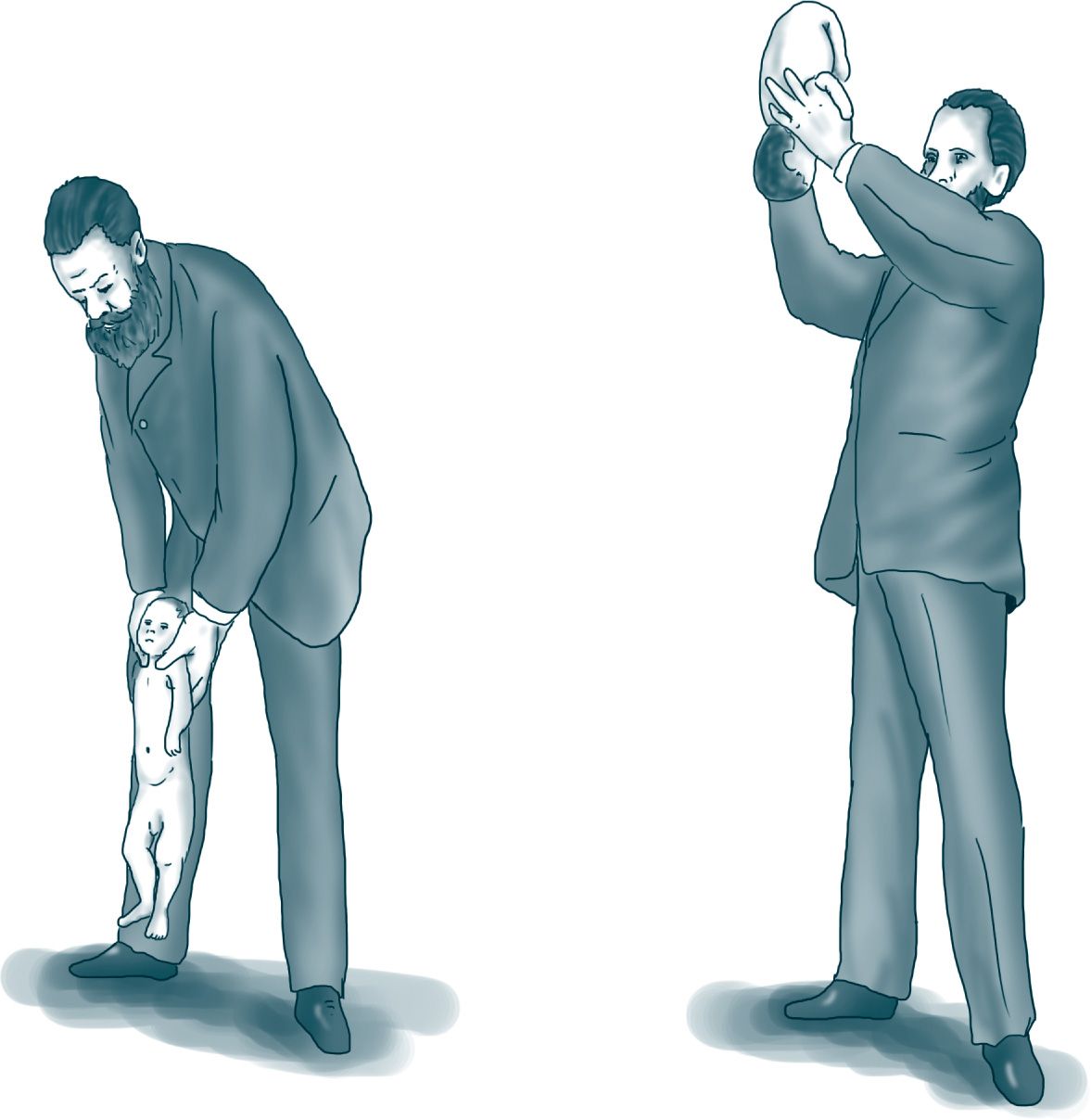
Figure 11-1. The outdated and obsolete Schultze method of neonatal resuscitation from the 19th century. From Schultze BS. Der Scheintod Neugeborener. Jena: Mauke’s Verlag; 1871.
There are approximately 4 million neonatal deaths per year worldwide, and 23% of these are the result of birth asphyxia.4 In an attempt to improve outcome, the Neonatal Resuscitation Program (NRP) was developed by a joint American Academy of Pediatrics (AAP) and American Heart Association (AHA) committee, which produced its first textbook in 1987.5 The NRP was initiated to ensure that at least one person trained in neonatal resuscitation be present in every hospital delivery, and it is designed to be uniform for all personnel who attend deliveries, including physicians and nurses. By the end of 2010, more than 2.9 million health care providers in the United States had been trained in the techniques of neonatal resuscitation.5 It is strongly recommended that anyone who may be involved in neonatal resuscitation should be trained and kept up-to-date with these neonatal resuscitation programs.
One of the most important factors demonstrated to provide better outcomes in neonatal resuscitation is communication among the caregivers. The other major criteria for success is that neonatal resuscitation is most effective when performed by a designated and coordinated team. Recent work in the field of neonatal resuscitation culminated in the guidelines mentioned above. Although these guidelines apply primarily to newborn infants undergoing transition from intra to extrauterine life, they may be applied within the first week to months after birth, should the clinician be called to a neonatal resuscitation.
Epidemiology
Delivery, although generally safe, may be complicated for some infants. Approximately, 10% of births will require some sort of assistance following delivery, and approximately 1% of these infants will require extensive resuscitation.6 In the United States, there are approximately 5000 delivery rooms, with a total of 4,130,665 births registered in 2009.7 According to these statistics, this will result in approximately 400,000 neonatal resuscitations a year, and thankfully the majority of these will result in a healthy newborn. Keep in mind that prolonged resuscitation in the newborn is a poor prognostic feature.
NEONATAL RESUSCITATION
Neonatal resuscitation should be planned in an organized fashion, with anticipation, preparation, evaluation, and management of the infant. Each item is described in detail below.
Anticipation: Identifying the At-Risk Mother and Fetus
Early knowledge of a complicated or high-risk pregnancy is important. In anticipating the need for resuscitation, it helps to monitor the progress of labor and fetal well-being. The need for resuscitation can be predicted in approximately 80% of cases.2 Table 11-1 identifies some of the many antepartum and intrapartum risk factors to consider, which should put one on high alert for the need to resuscitate the neonate.5 Another very useful method of assessing the fetus is fetal scalp blood sampling. Any time the procedure is carried out on the labor floor, the anesthesiologist should be informed beforehand and should be on standby for an urgent or emergent delivery. The fetal scalp sample values, both normal and abnormal, and their interpretations and resultant obstetric plans are outlined in Table 11-2.8
Table 11-1. Risk Factors Suggesting a Greater Need for Neonatal Resuscitation
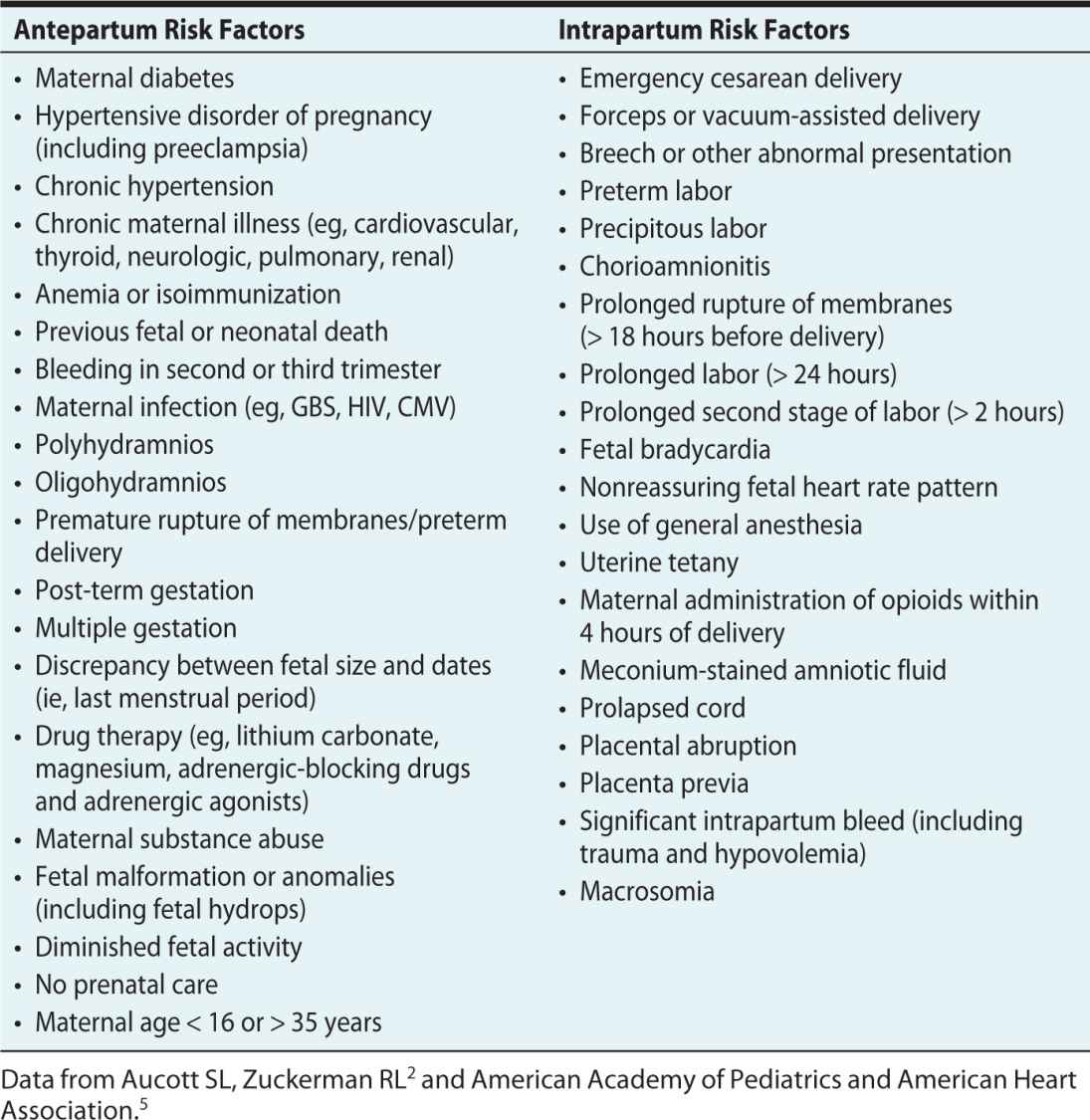
Table 11-2. Blood Gases/Fetal Blood Sampling
Used with permission from Scott Moses, MD at Fpnotebook.com. Fetal scalp pH. http://www.fpnotebook.com/OB/Lab/FtalSclpPh.htm. Updated July 16, 2014.8
Preparation
As with most things in anesthesiology, problems that can be foreseen, anticipated, and prepared for in advance may be dealt with more successfully. In trauma, the “golden hour” is often described as being the crucial resuscitation steps taken in the hour immediately after the initial trauma. In neonatal resuscitation, it may be considered that there is a “golden minute” immediately after the neonate is born. The initial two steps in the neonatal resuscitation algorithm take place over two 30-second intervals—the “golden minute.” Despite prior assessment of risk during pregnancy and labor, there remains unpredictability about which newborns may require resuscitation; therefore, staff must be ready to resuscitate in all situations. A good resource to guide clinical practice in this regard is the 2010 update from the AHA and the AAP resuscitation guidelines,6 some of which are discussed later in this chapter. It must be remembered that these guidelines are continually being challenged and updated, and some of the guidelines are already being reassessed.
In preparing for resuscitation of the newborn, one must become familiar with all the equipment that may be needed, and these should be checked on a regular basis. It is essential to have equipment readily available and in good working condition. See Table 11-3 and Figure 11-2 for equipment that should be on hand.

Figure 11-2. Various items for bag/mask ventilation. Data from http://www.indiamart.com/meditrininstruments/infant-careequipment.html.
Table 11-3. Equipment
Suction Equipment
• Bulb syringe
• Mechanical suction and tubing
• Suction catheters: 5F or 6F, 8F, and 10F, 12F or 14F
• 8F feeding tube and 20-mL syringe
• Meconium aspiration device
Bag-and-Mask Equipment
• Neonatal resuscitation bag with a pressure-release valve or pressure manometer (the bag must be capable of delivering 90%-100% oxygen)
• Face masks: newborn and preterm sizes (masks with cushioned rim preferred)
• Oxygen source
• Compressed air source
• Oxygen blender to mix oxygen and compressed air with flow meter (flow rate up to 10 L/min) and tubing
Intubation Equipment
• Laryngoscope with straight blades: number 0, 00 (preterm) and number 1 (term)
• Extra bulbs and batteries for laryngoscope
• Tracheal tubes: 2.5, 3.0, 3.5, and 4.0 mm ID uncuffed
• Stylet (optional)
• Scissors
• Tape or securing device for tracheal tube
• Alcohol sponges
• CO2 detector or capnograph
• Laryngeal mask airway
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


