Chapter 38 Anesthetic and Airway Management of Microlaryngeal Surgery and Upper Airway Endoscopy
I General Considerations
The range and precision of laryngologic surgical procedures have dramatically expanded over the past decade. Patient outcomes have improved due to technologic advances such as the introduction of high-magnification operating microscopes and video endoscopes, instrument miniaturization, new injection materials, and the use of powered instrumentation and optical fiber–based lasers.1–5
Advances and demands of the new surgical techniques and an expanding patient population that was previously considered unsuitable for surgery have created novel challenges for the anesthesiologist. State-of-the-art anesthesia and airway management for laryngeal surgery require the anesthesiologist to be adept with various methods of managing the difficult airway and performing airway exchange, to competently execute intraoperative ventilation strategies, to be proficient with inhalational and total intravenous anesthesia, and to quickly tailor anesthetic techniques to the various durations of the surgical cases. New challenges have developed with the widespread introduction of minimally invasive laryngeal robotic surgery, which demands a fully open surgical field for three-dimensional visualization and superior motor control.4,6,7
Successful anesthetic management of microlaryngeal cases requires a high degree of cooperation with the surgeon, a reciprocal understanding of the potential problems, and adequate preparation on both sides to meet the anticipated challenges that may arise.1,3,8,9 Thorough appreciation by the anesthesiologist of the complexity of the upper airway anatomy, the pathologic process involved, and all steps of the surgical procedure is necessary for devising a rational anesthetic plan and maintaining a good working relationship with the surgeon.1,8,10 The expert ability to safely share the patient’s airway with the surgeon, in conjunction with an intimate knowledge of possible immediate intraoperative and early postoperative complications of laryngeal surgery, greatly contributes to safe patient management in the perioperative period.8
Microlaryngeal surgery encompasses a wide range of laryngeal procedures that can be organized in two broad categories: phonomicrosurgery (i.e., benign and malignant vocal cord lesions, laser laryngeal surgery, and vocal cord augmentation) and laryngeal framework surgery (i.e., vocal cord paralysis and motion disorders, scarring, stenosis of the glottic, subglottic, and tracheal areas, and laryngeal trauma).1 For practical purposes, these may be further categorized as involving endoscopy alone, surgical excision, injection, dilation, or a combination of these approaches.
This chapter focuses on airway management and anesthesia for microlaryngeal surgery, diagnostic direct laryngoscopy, and endoscopy (i.e., bronchoscopy and esophagoscopy). A combination of these three interventions, called panendoscopy, is typically performed as part of the diagnostic work-up for patients with head and neck cancer, and is accompanied by surgical biopsies of the base of the tongue, piriform sinuses, nasopharynx, and other diseased or suspicious areas.11–13 Additional surgical indications for bronchoscopy and esophagoscopy are discussed in the corresponding sections of this chapter, and management of pediatric patients is discussed separately from approaches to adults.
II Patient Preoperative Evaluation and Preparation
Patients presenting for phonomicrosurgery may have a variety of comorbidities contributing to their voice symptoms and affecting anesthetic management. Changes in voice quality can be exaggerated by inadequate airflow production (e.g., chronic obstructive pulmonary disease [COPD]) or vocal fatigue caused by neuromuscular disorders (e.g., myasthenia gravis, muscular dystrophy, Parkinson’s disease).1 Various rheumatologic and musculoskeletal ailments can alter posture, impairing voice quality, and endocrine disorders, such as hypothyroidism, can cause dysphonia as a result of swelling in the Reinke’s space (i.e., superficial lamina propria) of the vocal cords.1
Almost one half of the patients presenting with laryngeal and voice disorders have silent laryngopharyngeal reflux as the primary cause or as a significant etiologic factor.1,14 Coexistent significant glottic insufficiency (e.g., vocal cord paralysis) may place these patients at increased risk for aspiration of gastric contents,13,15 and it can usually be diagnosed during a routine preoperative flexible fiberoptic laryngoscopy or laryngostroboscopy performed by the surgeon. Those presenting for esophagoscopy for evaluation and treatment of esophageal obstructing lesions, achalasia, Zenker’s diverticulum, active gastrointestinal bleeding, or esophageal foreign body removal constitute another category of patients at high risk for aspiration. Even when gastroesophageal reflux is not clinically significant, adequate preoperative pharmacologic control of the symptoms is warranted: the combination of acid exposure and direct trauma from the operating procedure and the endotracheal intubation can lead to laryngeal mucosal injury.16
Many patients presenting for laryngeal surgery and panendoscopy have a long history of heavy smoking and drinking,17 which are directly linked to the development of squamous cell carcinoma of the larynx, the second most common malignancy of the head and neck.18 It is not uncommon for these patients to present with anemia.18 Appropriate laboratory studies should be obtained, and the electrolyte and fluid status of these patients should be optimized preoperatively.
Chronic cigarette smoking and alcohol use can cause induction of the cytochrome P450 multi-enzyme system, leading to increased perioperative requirements for opioids and neuromuscular blockers and generation of higher levels of potentially toxic metabolites of volatile halogenated anesthetic agents.19–22 Patients with chronic alcohol consumption require preoperative evaluation of liver function and coagulation status. For those with advanced liver disease, controlled hypotensive techniques should be avoided, and intraoperative hypotension should be treated aggressively to prevent adverse outcomes associated with prolonged decrease in hepatic circulation and further deterioration of liver function.23
Many patients who present for laryngeal surgery are elderly and have cardiovascular disease. Appropriate diagnostic tests are indicated for them as part of the preoperative work-up. The pulmonary status of COPD patients should be optimized to decrease airway reactivity and the possibility of postoperative pulmonary complications. Patients with significant lung disease and ventilation-perfusion ( ) mismatch may not be suitable candidates for intraoperative ventilation techniques, such as spontaneous ventilation, apneic intermittent ventilation (AIV), or jet ventilation (JV),22–24 which may be required for microlaryngeal surgery (see “Intraoperative Ventilation Techniques and Strategies for Microlaryngeal Surgery”).
) mismatch may not be suitable candidates for intraoperative ventilation techniques, such as spontaneous ventilation, apneic intermittent ventilation (AIV), or jet ventilation (JV),22–24 which may be required for microlaryngeal surgery (see “Intraoperative Ventilation Techniques and Strategies for Microlaryngeal Surgery”).
The rate of difficult endotracheal intubation may reach almost 16% among patients presenting for ear, nose, or throat cancer surgery,25 which is on average six times higher than among the general surgical patient population.25–29 Comprehensive preoperative airway assessment is paramount (see Chapter 8); however, standard anesthesia airway assessment tests fail to account for aspiration risk, lower airway problems, and base of the tongue pathology (e.g., epiglottic cancer, epiglottic and vallecula cysts, lingual tonsillar hypertrophy). Pathology of the base of the tongue may be encountered with increased frequency in patients presenting for panendoscopy and microlaryngeal surgery (Fig. 38-1).
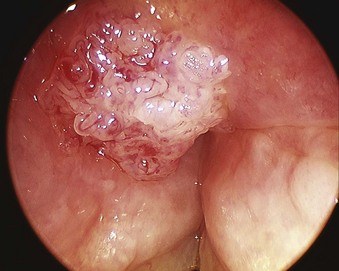
Figure 38-1 Epiglottic carcinoma.
(Courtesy of Edward Damrose, MD, Stanford University Medical Center, Stanford, CA.)
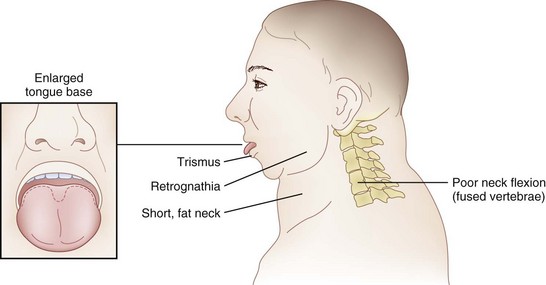
Postradiation changes in the neck and decreased mandibular protrusion are important factors predicting the risk of impossible mask ventilation, difficult mask ventilation, and difficult intubation in patients at risk for these conditions (see Chapter 8),30,31 and these risk factors may occur with increased frequency among patients presenting for microlaryngeal surgery or panendoscopy.12 The pharyngeal space may also be reduced by limited submandibular compliance of the soft tissues (e.g., cancerous involvement, masses, inflammation, previous radiation therapy) (Fig. 38-2), which may result in difficult intubation or failed intubation due to the restriction of the space that accommodates the tongue during direct laryngoscopy.32

Pharyngeal restriction can be further accentuated by a large tongue or intraoral masses that can be exophytic and mobile.32 Drooling, dysphagia, and expiratory snoring are the signs of marked pharyngeal restriction,17,32 but inspiratory stridor at rest represents the most worrisome sign, suggesting a reduction in airway diameter at the supraglottic, periglottic, or glottic level of at least 50%.15,31–33
Airway compromise in these patients may also involve the lower airways. Airway narrowing at the tracheal or tracheobronchial level is typically characterized by expiratory stridor, whereas biphasic inspiratory-expiratory stridor usually points to obstructive subglottic lesions.8 In some cases, preoperative examination of the flow-volume loops may be helpful.34
It is prudent to assess the laryngeal mobility, the degree of tracheal deviation, and the location of the cricothyroid membrane (CTM).18 Significant tracheal deviation, especially in combination with the fixed hemilarynx (Fig. 38-3) and poor or absent visualization of the vocal cords during preoperative nasal endoscopy, can be an ominous sign,33,35 warranting performance of an awake tracheostomy, if technically feasible. Usually, the extent of disease in elective cases has been comprehensively evaluated preoperatively by routine chest radiography, computed tomography (CT), magnetic resonance imaging (MRI), and flexible fiberoptic laryngoscopy, providing the anesthesiologist with valuable information regarding the location, size, spread, and vascularity of the obstructive lesions; the degree of obstruction; the mobility of the vocal cords; and the extent of laryngeal and tracheal deviation or compression.8,18,36 Preoperative discussion of these findings with the surgeon helps to devise safe and rational airway management and anesthetic plans for the patient.18

Other airway considerations for patients presenting for microlaryngeal surgery or panendoscopy include anticipation of the presence of supraglottic and glottic edema due to inflammation, infection, tumors, previous radiation therapy or repeated endoscopies,37 and careful dental assessment. Gentle airway manipulation during direct laryngoscopy is essential. The use of a smaller-diameter endotracheal tube (ETT) is frequently warranted, and the absence of dental trauma should be documented before surgical instrumentation of the patient’s airway commences.
III Operative Laryngoscopy and Microlaryngeal Surgery
A Special Considerations and Anesthesia Objectives
In contrast to direct laryngoscopes used by the anesthesiologists, which are designed only to identify the glottic opening, operating laryngoscopes can provide excellent and wide laryngeal exposure and allow diagnostic examination, biopsy, and operation on structures in the larynx and pharynx, with minimal distortion of the areas of surgical interest.16,38 The handles of these laryngoscopes are integrated with the blades and have a wide proximal aperture that facilitates the passage of instruments during suspension laryngoscopy.38,39 Many types of laryngoscopes exist (Fig. 38-4), each offering certain advantages for its intended application, such as the ability to better expose supraglottic, glottic, or subglottic areas.38 Many laryngoscopes are multipurpose, and selection is frequently dictated by individual or institutional preference.38

Figure 38-4 Commonly used operating laryngoscopes. The posterior apertures of the Kleinsasser (left), Dedo (center), and Holinger (right) operating laryngoscopes are shown. The bigger size and wider channel of the Kleinsasser and Dedo laryngoscopes allows passage of the surgical instruments and binocular microlaryngeal surgery. Notice the metal cannula inserted into the left side port of the Kleinsasser laryngoscope for supraglottic jet ventilation (JV). In the Dedo scope, the JV port is integrated with the lumen, and it can be used for smog evacuation during laser surgery. The Holinger laryngoscope is monocular but has greater maneuverability. It is widely used for diagnostic laryngoscopy and visualization of the anterior commissure. The left side channel of the Holinger laryngoscope is occupied by a light guide. Supraglottic JV through the Holinger laryngoscope requires insertion of a metal cannula inside its lumen (see Fig. 38-15).
With the use of these laryngoscopes, systematic endoscopy of the larynx and pharynx frequently proceeds in three stages, progressing from handheld examination to suspension laryngoscopy (for more detailed evaluation with the straight and angled telescopes) and then to microlaryngoscopy using the operating microscope for image magnification, biopsy, microsurgery, or laser surgery.38 Suspension laryngoscopy (Fig. 38-5) frees the surgeon’s hands for precision bimanual surgery and facilitates maintenance of a stable plane of anesthesia.38,40 The use of a video monitor by the surgeon permits the anesthesiologist to observe the surgical procedure and monitor the patient’s airway.


The essential requirements for precision microlaryngeal surgery and optimal preservation of function include a clear and still surgical field, absence of patient movement, and allocation of sufficient time to carefully complete the procedure in an unhurried manner.9,38,39,41 The patient’s airway must be protected from blood, debris, and irrigation fluid, and ventilation must be adequately controlled.3,8,41 The anesthesiologist must safely share the patient’s airway with the surgeon, and must be prepared to skillfully and confidently switch from one ventilation technique to another during the case if needed or dictated by surgery.
In most surgical procedures, the patient’s airway is shared with the surgeon, and immediate access to the airway is difficult or impossible because the operating room (OR) table is turned 90 or 180 degrees away from the anesthesiologist. The ETT must be secured diligently to prevent accidental extubation under the surgical drapes or withdrawal of the ETT into the larynx, resulting in a sudden air leak or possible compression of the anterior branch of the recurrent laryngeal nerve by the ETT cuff.42,43
Performance of conventional and operative direct laryngoscopy, supraglottic tissue distention, and laryngeal stimulation elicit intense cardiovascular responses, resulting in tachycardia, arterial and pulmonary hypertension, and arrhythmias.44–46 Although these responses are usually short lived, myocardial ischemia and compromise of cerebral circulation may occur in high-risk patients, resulting in adverse outcomes.47–49 Anesthetic technique should ensure a stable plane of anesthesia, nonstimulating emergence from anesthesia, a rapid return of consciousness, and protective airway reflexes, and it should facilitate quick discharge of patients, because most of these surgical procedures are done on an outpatient basis.3,8
Special attention should be directed to adequately protecting the patient’s eyes and arms to prevent accidental injury or compression by heavy surgical instrumentation.9 When rigid endoscopy is planned, a tooth guard should be used routinely.34 It may be prudent to warn the patients in advance of the potential for dental trauma, and any previous dental damage should be carefully documented.34,43
Patients who are vocal performers or use the voice in some professional capacity present unique challenges.16 The anesthesiologist must frequently think outside the box and exercise different advanced airway management options to avert trauma to the patient’s vocal cords and cricoarytenoid joints.
B Airway Management for Microlaryngeal Surgery
1 Conventional and Advanced Airway Management
Video laryngoscopy reliably improves laryngeal exposure by at least one grade,50–54 allows continuous observation of the entire intubation procedure by the entire team, and may therefore be a near-ideal technique for managing difficult airways in patients presenting for microlaryngeal surgery. Choosing the video laryngoscopic device depends on the operator’s preference and must consider the nature and location of the lesions. For example, it may be safer to navigate around tumors at the base of the tongue with the Pentax Airway Scope, whose blade engages under the epiglottis, unlike other devices that typically require the tip of the blade to be placed in the vallecula. Video laryngoscopes that use the steering technique (i.e., styleted ETT), such as the Glidescope video laryngoscope, offer better control of intubation and may facilitate ETT maneuvering around the intraoral masses.55 Although the use of the Glidescope may be less traumatic compared with the Airtraq in patients presenting for microlaryngeal surgery,56 in the largest published series of Glidescope-assisted intubations in more than 2000 patients with difficult airways,57 the strongest predictor of the steering technique failure was altered neck anatomy with presence of a surgical scar, radiation changes, or a mass. These conditions are frequently encountered in patients presenting for diagnostic direct laryngoscopy and microlaryngeal surgery.
Although advanced airway management techniques can be highly successful when direct laryngoscopy fails, the patient’s unfavorable anatomy (Fig. 38-6) may not be modifiable for the surgical exposure, which requires the use of the largest operating laryngoscope and placement of the patient’s head in the Boyce-Jackson position using a combination of cervical flexion and atlantooccipital extension (see Fig. 38-5).1,38,58,59 If suspension laryngoscopy fails or if the location of the lesion is not easily accessible, it can be performed, to the extent microlaryngeal surgery permits, with the help of the flexible fiberoptic bronchoscope (FFB) inserted through the laryngeal mask airway (LMA).60–62 The intubating laryngeal mask airway (iLMA) offers certain advantages, such as a rigid, wide metal tube that can accommodate a large-diameter FFB,61 optimal alignment of the iLMA aperture with the glottic opening,63 diminished hemodynamic responses compared with suspension laryngoscopy,61 and superior ventilation capabilities.63–66
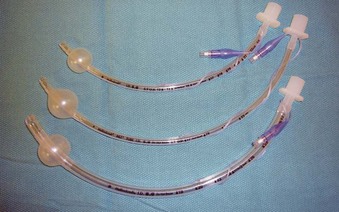
The iLMA is associated with an outstanding success rate for blind endotracheal intubation in patients with difficult airways.63,65 Unfortunately, the manufacturer-supplied iLMA ETTs are too big for most microlaryngoscopic surgery. An ETT with a smaller inner diameter (ID) (e.g., 5.0-mm ID microlaryngeal tracheal [MLT] tube) is typically required to maximize the surgical view (Fig. 38-7). Placement of MLT tubes through the iLMA can be achieved with the help of a small-diameter FFB; however, passage of the ETT through the laryngeal inlet into the trachea is blind. Blind advancement of the ETT may cause inadvertent laryngeal trauma and core out pedunculated supraglottic or glottic tumors, nodules, or cysts.56,67 When the FFB route (with or without the use of a supralaryngeal airway device) is chosen for endotracheal intubation, it is advantageous to closely match the outer diameter (OD) of the scope with the ID of the ETT to minimize the risk of complications associated with blind ETT advancement. Use of optical stylets (e.g., Bonfils, Shikani, Clarus Video System) may also be beneficial in that regard, because the ETT will follow the trajectory of the stylet navigated under direct vision through the vocal cords. However, most of the available adult-size stylets require the use of an ETT with a minimum ID of 5.5 to 6.0 mm.
The decision to proceed with an awake or asleep approach to an anticipated difficult airway should follow the American Society of Anesthesiologists (ASA) difficult airway algorithm,68 with special attention directed to predictors of difficult mask ventilation, impossible mask ventilation, and their association with difficult intubation (see Chapter 8). The anesthesiologist also should review the pertinent preoperative findings identified on flexible fiberoptic laryngoscopy, chest radiography, CT, and MRI and should discuss these findings with the surgeon.
If an asleep approach to the difficult airway is chosen, several preformulated alternative airway management plans must be in place before induction of anesthesia. If the airway is marginal, the patient’s neck should be prepped, and the surgical team should be present on induction, ready to perform an emergent cricothyrotomy or tracheostomy, or to employ rescue techniques such as the use of the surgical anterior commissure scope or a rigid bronchoscope.11,18,69,70 The anterior commissure scopes (e.g., Holinger, Ossoff-Pilling, Benjamin Slimline/Super-Slimline, Jackson) (Fig. 38-8; see Fig. 38-4) have great leverage capabilities, incorporate the recessed lighting and concurrent rigid microsuction, and can be very effective in handling poor laryngeal exposure or glottic obstruction.1,13,38,69 The anterior flare at the distal oval end allows these scopes to be used as a conduit for orotracheal intubation when the bougie introducer or the ETT is passed directly down the lumen (Fig. 38-9).69


Figure 38-9 Airway rescue is achieved with a bougie introducer and a Holinger laryngoscope in a patient with difficult laryngeal exposure. The endotracheal tube (ETT) cannot be directly advanced down the narrow barrel of the Holinger laryngoscope due to impaired visualization during tube advancement. The bougie introducer is used first, followed by removal of the laryngoscope and railroading the ETT over the bougie into the patient’s trachea. The ETT can be directly advanced through the wider lumen of other laryngoscopes, such as the Lindholm or Dedo (see Fig. 38-14).
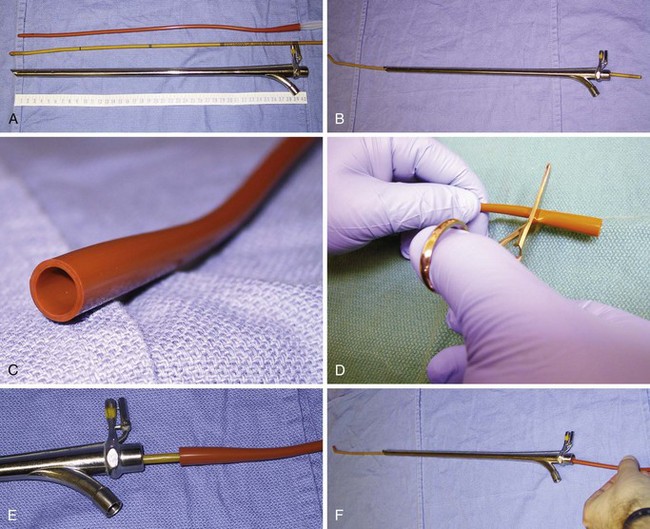
In experienced hands, rigid bronchoscopy may be used to rescue failed direct laryngoscopy and failed intubation and to manage a “cannot intubate, cannot ventilate” (CICV) situation.68 It also serves as an indispensable tool for managing acute airway obstruction resulting from foreign bodies, hemoptysis, or tumors.71 After the bronchoscope is placed into the patient’s trachea by the surgeon, manual (Fig. 38-10) or JV can commence in a safe manner through the lumen of the bronchoscope. Subsequent airway exchange to the ETT can be performed using a bougie introducer (Fig. 38-11).72,73 This exchange technique can also be conducted when the rigid bronchoscope is employed first as part of a panendoscopy procedure in patients with abnormal airway.

Patients with an advanced airway obstruction and inspiratory stridor at rest comprise some of the most feared and complicated cases for the anesthesiologist.33 The incidence of difficult mask ventilation and impossible mask ventilation among patients with severe stridor and upper airway obstruction of more than 75% of the lumen reaches 40% and 6%, respectively,74 compared with 1.4% and 0.15% for the general surgical population.30,31,75 These patients frequently present for panendoscopy and microlaryngeal surgery on an emergent or semi-emergent basis, yet they require a systematic and thoughtful approach by the anesthesiologist and the surgeon.38 The nature of the obstructing lesion (e.g., vascular, submucosal, pedunculated, inflammatory) and its location (e.g., supraglottic, glottic, subglottic, midtracheal, lower tracheal, and bronchial [mediastinal]) may require completely different intubation considerations and approaches.17,33,34,36,38,69,71
In the context of laryngeal surgery, the optimal technique of airway management of the stridorous patient with an advanced proximal airway obstruction (i.e., supraglottic, glottic, and subglottic levels) remains a subject of controversy. An awake flexible fiberoptic intubation, inhalational induction, and intravenous induction with muscle relaxants17,33,74,76 have been used successfully, but none should be considered fail-safe. Thorough preoperative discussion of the surgical pathology and formulation of closely coordinated airway management plan with the surgeon are essential for safe management of these patients.
Based on our experience and review of the pertinent literature,17,33,35,38,69,71,74,76–80 current recommendations for management of the critically obstructed airway can be outlined as follows:
1. For patients with severe stridor (e.g., symptoms exaggerated at night, hypoxemia-induced agitation or panic attacks, use of accessory muscles on inspiration, a large tumor, fixed hemilarynx, gross anatomic distortion, a larynx not visible on preoperative nasal endoscopy or flexible fiberoptic laryngoscopy), strongly consider tracheostomy under local anesthesia without sedation.
2. Patients with moderate stridor and a significant lesion seen on nasal endoscopy or flexible fiberoptic laryngoscopy, but who are considered possible to intubate, are best managed with an inhalational induction or an awake fiberoptic intubation. All airway instrumentation should proceed in a careful and gentle manner. Endotracheal intubation should be accomplished rapidly, with a small ETT. The number of attempts should not exceed two, because critical airway obstruction can quickly progress to complete as a result of manipulation of the airway.
3. If an inhalational induction is chosen, a sufficiently deep and stable plane of anesthesia is essential to avoid loss of the airway (e.g., avoidance of cough, laryngospasm). Endotracheal intubation should be performed under direct vision (e.g., direct laryngoscopy, video laryngoscopy, flexible fiberoptic bronchoscopy). Muscle relaxants should be avoided until after the intubation is completed to prevent sudden, complete airway obstruction, especially when the tumor is subglottic. The patient’s neck should be prepared, and the surgical team should be present and ready to attempt an airway rescue with an anterior commissure scope or a ventilating rigid bronchoscope or by emergent cricothyrotomy or tracheostomy.
4. If endotracheal intubation under direct vision (e.g., direct laryngoscopy, video laryngoscopy, flexible fiberoptic bronchoscopy) fails in an anesthetized or awake patient or is deemed problematic, tracheostomy should be performed expeditiously, with the patient breathing spontaneously.
5. An awake fiberoptic intubation should be used with caution, because sudden loss of the airway can be precipitated by one or more of the following factors:
6. Additional fallback strategies may include the following:
7. Patients with inspiratory obstruction due to bilateral vocal cord paralysis or fixation of cricoarytenoid joints typically do not present ventilation or intubation problems.
8. If tracheostomy is avoided, an extubation strategy must be decided on with the surgeon. Extubation should be performed over an airway exchange catheter (AEC), with the necessary reintubation equipment immediately available. Some patients should remain intubated until the airway inflammation and edema subside, and the patient’s airway is then reevaluated.
2 Intraoperative Ventilation Techniques and Strategies for Microlaryngeal Surgery
Surgery can be conducted in an awake patient, frequently under conscious sedation, or with the patient anesthetized (Box 38-1). The ventilation options under general anesthesia consist of “tube” (i.e., endotracheal intubation) and “tubeless” techniques, with the latter represented by the techniques of spontaneous ventilation, AIV, and JV.8,13,38,81,82
Box 38-1 Ventilation Techniques and Strategies for Microlaryngoscopic Surgery
a Awake Airway Surgery with Conscious Sedation
For selected patients, many laryngoscopic procedures can be safely and effectively performed in an office-based setting, including diagnostic endoscopy, laser surgery, panendoscopy for cancer screening and biopsies, and therapeutic vocal cord injections.2–516 The key to success for office-based surgery remains adequate topical and regional anesthesia of the patient’s airway, which is usually performed by the surgeon and typically follows preparation of the patient for awake oral and nasal flexible fiberoptic intubation (see Chapter 19). Although highly motivated patients can undergo office-based laryngoscopic surgery strictly under local anesthesia, most desire sedation and amnesia.3
If presence of the anesthesiologist is requested, the main objectives are to monitor for possible local anesthetic toxicity (see Chapter 19), to supplement local anesthesia with a rapidly titratable and reversible state of sedation, and to treat acute hyperdynamic responses that can occur in up to 20% to 30% of patients, despite seemingly adequate topical anesthesia of the airway.3,83 Judicious use of intravenous opioids or sedatives/hypnotics, or both, is paramount, because a loss of patient cooperation may result in intraoperative injury.3,16,34 Sedation of the patients with obstructive sleep apnea and morbid obesity should be performed with extreme caution.84,85
b Asleep Airway Surgery with General Anesthesia
General anesthesia for microlaryngeal surgery represents a unique example of some of the conflicting intraoperative goals that exist between the surgeon and the anesthesiologist with regard to the patient’s airway control and maintenance. For the surgeon, ideal operating conditions would be completely unobstructed surgical visualization, unimpeded surgical manipulation, and absence of movement in the surgical field. From the anesthesiologist’s perspective, the ideal anesthetic technique would allow adequate protection of the patient’s lower airway from aspiration and the use of stable, controlled mechanical ventilation with the ability to measure the concentration of anesthetic gases, peak inspiratory pressure (PIP), inspired oxygen concentration (FIO2), and end-tidal carbon dioxide level (EtCO2).81 In most cases, these objectives can be balanced by the use of a small MLT tube, maximizing the patient’s safety and the success of surgery.
Endotracheal Intubation with Microlaryngeal Tracheal Tubes
The use of a small (5.0-mm ID) MLT tube with positive-pressure ventilation remains the standard for airway management in most nonlaser microlaryngeal surgery, and it is associated with minimal or no intraoperative complications.86,87 (For anesthetic management of the laser airway surgery see Chapter 40.) Adequate gas exchange can be maintained through small-ID ETTs in most adult patients,88,89 unless the duration of surgery approaches 2 hours (which happens rarely).88 Even then, despite a consistent trend toward progressive hypercapnia and respiratory acidosis, the pH and EtCO2 values remain within physiologic range.89
With most glottic pathology originating in the anterior two thirds of the larynx,90 consistent positioning of a small MLT tube between the arytenoid cartilages in the posterior part of the glottis leaves most of the surgical field unobstructed to the surgical view and manipulations.4,13,16,38,91 Even with many posterior glottic disorders, it may be possible for the surgeon to gently displace the MLT tube anteriorly with the microsurgical cupped forceps or to perform the surgery using the specially designed posterior glottic laryngoscopes.90,92
However, if the posterior glottis is occupied by a significant surgical pathology (e.g., posterior glottic or subglottic stenosis, transglottic tumor) (Fig. 38-12), use of alternative, tubeless ventilation techniques becomes necessary.38 Because of the surgeon’s preference, tubeless ventilation can also be requested as a primary ventilation mode from the outset of the procedure.

Tubeless Techniques
Spontaneous Ventilation
Spontaneous ventilation is rarely used in adult microlaryngeal surgery,93–95 but it is commonly employed in the pediatric patient population, for whom it offers the additional ability to evaluate dynamic airway function and the level of obstruction (see “Anesthesia for Pediatric Airway Endoscopy and Microlaryngeal Surgery”). Anesthetic gases can be delivered (insufflated) through a nasal trumpet connected through an ETT adapter to the anesthesia circuit,96–99 an ETT positioned in the nasopharynx,82,100,101 a metal cannula, a side port of the rigid bronchoscope or operating laryngoscope (Fig. 38-13; see Fig. 38-10),38 or a catheter placed through the vocal cords into the patient’s trachea.9,102,103 Scavenging of anesthetic gases can be facilitated with an open suction tube at the corner of the patient’s mouth.

Although this technique offers free access to the larynx, it does not provide a still surgical field for precision surgery, it affords no protection of the lower airway, and it contaminates the OR environment.34,87,103 Deep planes of anesthesia are usually required to blunt the laryngeal responses and to prevent patient movement, which tends to provoke cardiovascular instability and ventilatory compromise (i.e., hypoxemia, hypercarbia, and short periods of apnea).8,39,104 With careful technique, inhalational agents can be substituted for total intravenous anesthesia (TIVA).82,96,105 However, control of the patient’s movement and a stable plane of anesthesia frequently remains problematic.104 Monitoring an adequate hypnotic state (e.g., processed electroencephalographic activity) may be advisable for these patients.
The protagonists of spontaneous ventilation technique may wish to routinely supplement general anesthesia with topical or local anesthesia of the airway (usually done by the surgeon after deployment of suspension laryngoscopy), which facilitates maintenance of a more stable and lighter plane of anesthesia, promotes hemodynamic and respiratory stability, and decreases the incidence of intraoperative laryngospasm.39,82,96,103,105,106
Apneic Intermittent Ventilation
AIV remains a relatively popular technique for microlaryngeal surgical procedures of short duration in some surgical centers.87 Compared with spontaneous ventilation, it affords more stable and controlled anesthetic conditions, as well as full muscle relaxation. After induction of anesthesia, the patient’s lungs are ventilated by a face mask or an LMA, which is followed by a period of apnea to allow deployment of a suspension laryngoscope by the surgeon. The patient’s trachea is subsequently intubated by the surgeon with a small-diameter, preferably uncuffed ETT that is placed through the lumen of the laryngoscope,87 and the patient’s lungs are hyperventilated with an FIO2 of 1.0 (Fig. 38-14). The ETT is then removed to provide a fully unobstructed and still surgical view of the larynx. The ETT is withdrawn and reinserted as frequently as necessary to maintain an oxygen saturation by pulse oximetry (SpO2) of 90% or greater and EtCO2 between 40 and 60 mm Hg,18,87,107 allowing periods of apnea up to 5 to 10 minutes in healthy adult patients.87,108 Apneic oxygenation through the hypopharyngeal catheter, preceded by an adequate period (10 minutes) of preoxygenation and denitrogenation of the patient’s lungs, can be tried in anesthetized and paralyzed patients.108

TIVA is typically used for maintenance. Monitoring the hypnotic state of anesthesia is advisable during AIV, because the incidence of awareness and recall may reach 4% (30 times higher than in the general surgical population), especially when the inhalational agents are used to supplement intravenous anesthesia.109,110
The disadvantages of AIV include slowing the pace of surgery, disruption of the surgical field, possible trauma to the vocal cords and lower airway due to repeated endotracheal intubation, and a propensity for laryngospasm.87 In a study of more than 350 patients,87 the incidence of intraoperative laryngospasm with AIV was 1.4%. The AIV may not be suitable for patients with significant lung or cardiovascular disease,107 and it leaves the patient’s lower airway unprotected to aspiration.18
Appropriate and successful phonomicrosurgery can rarely be performed using AIV, because the apnea periods are too short to permit unhurried precision surgery.1,111 This technique may be better reserved for short, uncomplicated cases.
Jet Ventilation
Supraglottic JV (i.e., jet nozzle above the glottic opening) for microlaryngeal surgery can be performed through the side port of a suspension operating laryngoscope, with the jet cannula attached to the lumen of the laryngoscope (Fig. 38-15; see Fig. 38-4)1,24,59,112 or through a specialized jet laryngoscope.113,114
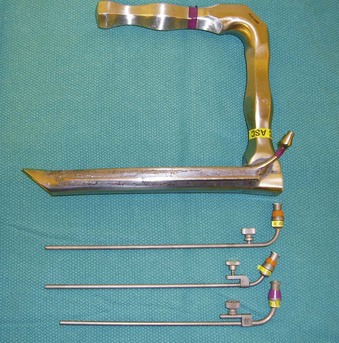
Figure 38-15 A Dedo operating laryngoscope with the integrated side port (top) can be used for supraglottic jet ventilation, and different jetting metal cannulas (bottom) can be inserted through the side ports of the operating laryngoscopes or directly through their lumen (see Fig. 38-4).
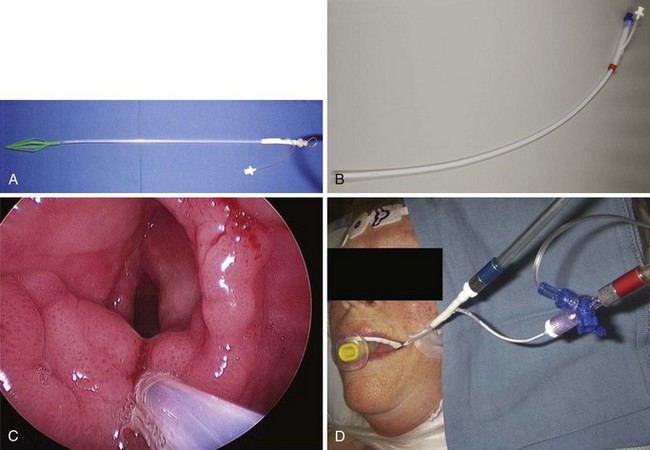
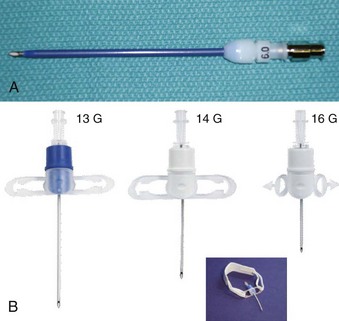
Subglottic JV (i.e., jet nozzle below the glottic opening) is established by bypassing the larynx from above (i.e., translaryngeal or transglottal approach) or below (i.e., percutaneous approach) through the CTM or the upper TTJV rings.74,86,87,111 Transglottal JV typically employs specialized, laser-safe, small-diameter, orally placed, double-lumen catheters (Fig. 38-16),24,81,115,116 in which the large port is used for jetting and the smaller lumen for monitoring the distal airway pressure and respiratory gases. Long, single-lumen catheters (typically 1.5- to 3-mm ID), some of which are laser resistant, may be used and can be placed through the oral or nasal route24,34,87,102,117–119; however, they lack concurrent monitoring capability. Alternatively, a small-diameter, movable, metal jet cannula can be passed through the glottis by the surgeon after the suspension laryngoscope is in position (Fig. 38-17).87,120 For transglottal JV, midtracheal placement of the catheter or cannula is usually preferred. TTJV is typically administered through a long catheter or Ravussin-type cannula (Fig. 38-18).74,86,121 For TTJV catheter or cannula placement, the use of an FFB or a rigid bronchoscope may be advocated to monitor the procedure87,111,122 and to minimize the risk of unnoticed posterior tracheal wall laceration, which may lead to submucosal gas injection and barotrauma.87,111 Use of a rigid bronchoscope with the bevel turned posteriorly may be especially efficacious, because the posterior tracheal wall is protected by the bronchoscope from the needle entry.87 For transglottal JV and TTJV, endoscopic control also allows adjustment of the position of the distal end of the catheter or cannula to optimize HFJV.24,86,87,122

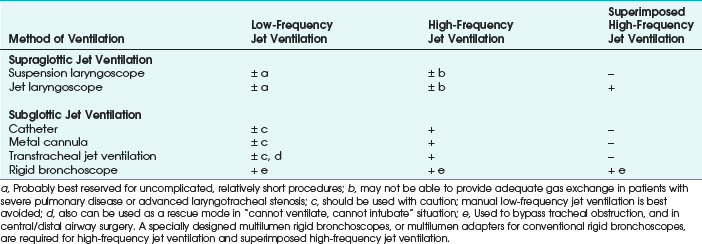
Compared with endotracheal intubation, supraglottic and subglottic JV techniques have distinct advantages of providing the surgeon with an enlarged, clear or minimally impeded, and undistorted view of the endolarynx, facilitating surgical access and eliminating flammable material (i.e., ETT) from the patient’s airway during laser surgery.24,115 Although supraglottic and subglottic ventilation techniques can use low-frequency jet ventilation (LFJV), HFJV, or superimposed high-frequency jet ventilation (SHFJV) modes,34,86,111,123–125 the use of these modes in clinical practice is usually more restrictive (Table 38-1).
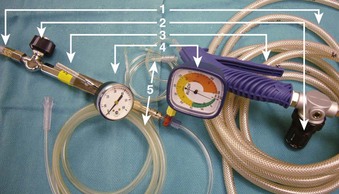
The use of manual supraglottic LFJV (i.e., Venturi jet ventilation) at a rate of less than 60 breaths/min continues to predominate in clinical practice,111 probably because of the low cost and easy accessibility of manual JV devices (Fig. 38-19) (a manual mode also can be preset on commercially available jet ventilators, where available).59,111,126,127 Although an overall incidence of complications with manual supraglottic LFJV may be low (0.42%),120 a survey of 229 U.K. centers revealed that it was responsible for most major complications (e.g., significant hypoxemia, barotrauma, unplanned admission to the intensive care unit) and for all deaths, especially when applied subglottically.111 This suggests that LFJV should be reserved for uncomplicated, elective procedures of short duration and that it may not be regarded as a standard of practice for microlaryngeal surgery.24 For increased safety, LFJV should be started with a low driving pressure (≤10 psi), which is gradually increased until visible chest excursions are observed, and adequate oxygen saturation is maintained.24,59,111
The subglottic HFJV mode (respiratory rate of 100 to 300 breaths/min; tidal volumes [VT] of 1 to 3 mL/kg), delivered through specialized automated jet ventilators, is typically used.24,34 Compared with supraglottic LFJV, in which intermittent apnea is frequently required due to significant vocal cord movement, subglottic HFJV significantly reduces laryngeal motion and affords a quiet surgical field without the need for interrupting ventilation.125 If vocal cord movement becomes a problem, HFJV driving pressure can be decreased, and the respiratory frequency can be increased to provide a smoother gas flow, or the ventilator can be turned off during particularly delicate parts of the procedure.24,125
Despite very small VT values, CO2 elimination during subglottic HFJV is facilitated by the upstream turbulent convective flow of CO2 along the decreasing gradient from the alveoli to the conducting airways.34 The alveolar-arterial CO2 gradient in patients with normal lung function is largely maintained within normal range.34,128 Monitoring EtCO2 during HFJV can be accomplished by briefly switching to LFJV mode on the ventilator to get a reliable signal or by using transcutaneous Pco2 monitoring.24 Administration of subglottic HFJV also results in a higher inspired O2 concentration, because entrainment of air is reduced deep inside the airway.24,86 Improved oxygenation is further enhanced by generation of continuous positive end-expiratory pressure in small airways (auto-PEEP), leading to alveolar recruitment and increased functional residual capacity (FRC).24,34,119 Nevertheless, patients with severely restricted lung compliance,  mismatch or shunting, and reduced FRC (e.g., morbid obesity) remain at increased risk for hypoxemia.86
mismatch or shunting, and reduced FRC (e.g., morbid obesity) remain at increased risk for hypoxemia.86
In contrast to supraglottic LFJV, with which contamination of the lower airway due to air entrainment is possible,34,81 a continuous, upward-directed flow of gas during subglottic HFJV creates a positive-pressure build-up, preventing blood and surgical debris from being directed down an unprotected airway.111,119,129 However, increased airway pressure creates concern about air trapping and barotrauma, mandating maintenance of adequate gas outflow at all times.130
Before the suspension laryngoscope is secured, with the patient anesthetized and a subglottic JV catheter or cannula in place, strategies for minimizing the risk of barotrauma on initiation of subglottic HFJV may include starting ventilation with low driving pressures (<15 to 30 psi), allowing sufficient exhalation time by avoiding high-frequency ventilation (i.e., starting with LFJV first), and maintaining the patient’s airway patency with the assistance of an oral airway or providing a jaw lift, if needed.74,86,87,125,131 Alternatively, initiation of the subglottic HFJV can be held off until the suspension laryngoscope is deployed, and ventilation is supported conventionally through a face mask or the LMA. It may be prudent to confirm absence of the subglottic catheter or cannula obstruction by the EtCO2 return and to check the catheter or cannula position endoscopically before subglottic HFJV commences.86,125
On emergence from anesthesia, small VT values and low peak and mean airway pressures associated with subglottic HFJV enable the patient to breathe spontaneously, facilitating a transition to adequate spontaneous ventilation.24,34,86,132,133 This transition can be further assisted at the end of surgery by increasing the frequency of ventilation to 300 breaths/min, increasing FIO2 to 1.0, and setting a ventilator driving pressure at about 10 psi (0.8 bar), which enables almost continuous flow of O2 and apneic oxygenation, as well as a rise in the carbon dioxide (CO2) level.24 If the conversion to spontaneous ventilation through a small subglottic catheter proves difficult, the patient’s airway can be supported through a face mask, LMA, or ETT, as required; these conventional bridge airway strategies equally apply to transitioning from supraglottic JV. If obstructive airway lesions exist, subglottic HFJV must be used with extreme caution. If upper airway obstruction is greater than 50%, the position of the jet nozzle should be proximal to the site of the obstruction to prevent barotrauma, or the obstruction must be bypassed by a rigid bronchoscope first.24,79
Total outflow obstruction with resultant barotrauma during subglottic HFJV can be quickly precipitated by surgical instrumentation, glottic edema, laryngospasm, or closure of the vocal cords due to inadequate depth of anesthesia or inadequate muscle relaxation.81,86,130 Modern automated jet ventilators (e.g., Monsoon III Universal Jet Ventilator [Acutronic Medical Systems AG, Hirzel, Switzerland], Twin Stream [Carl Rainer GmbH, Vienna, Austria]) incorporate multiple safety features, including automatic ventilator shutdown, if the user-preset pressure limits are exceeded.24,74 This design has enabled some experienced providers to successfully use high-frequency TTJV in patients with massive supraglottic lesions and severe airway compromise,74 for which the use of supraglottic or subglottic JV was not possible or surgically feasible. The presence of a second anesthesiologist to facilitate monitoring and maintenance of an upper airway was required and deemed an important safety factor in preventing intraoperative pressure-related complications in all cases.74 Although no major complications were observed in this series of 50 patients,74 the incidence of minor complications reached 20%, a more than threefold increase compared with the instances when high-frequency TTJV has been used in patients with less severe airway compromise.87 Study results hold some promise that a simple,134,135 portable expiratory ventilation assistance (EVA) device may be able to facilitate egress of gas through the jet catheter during TTJV, thereby increasing the safety of this technique; however EVA suitability for microlaryngeal surgery remains to be established.
Compared with the transglottal approach, high-frequency TTJV is associated with a significantly higher combined major and minor (e.g., transient hypoxemia) complication rate (see “Intraoperative Complications”),86,87 and it represents an independent risk factor for complications during JV for microlaryngeal surgery.87 Modern automated JV may not be able to remediate all possible causes of barotrauma associated with high-frequency TTJV; complications may be related to the TTJV catheter insertion problems, laryngospasm, and high-pressure episodes (e.g., coughing, active expiration) during the recovery period.80,86 Notwithstanding the attractive features of high-frequency TTJV, such as a motionless surgical field and a particularly easy transition to spontaneous respiration,86 it may be advisable to reserve the elective use of this technique (especially in cases of severe supraglottic airway obstruction) for the most complicated patients74 and to designate operators with significant clinical experience and expertise.74,80,86,111
SHFJV, which combines high-frequency and low-frequency ventilation modes, has been used effectively in surgical treatment of high-grade laryngeal and tracheal stenosis, even with a remaining glottic opening as small as 2 to 3 mm.136 SHFJV is delivered supraglottically through a specialized jet laryngoscope, which incorporates welded low-frequency and high-frequency jet nozzles (Fig. 38-20).113,136,137 As the streams (LFJV of 12 to 20 breaths/min; HFJV of 100 to 900 breaths/min) get simultaneously directed from the ventilator toward the center of the distal end of the jet laryngoscope, LFJV entrains air (Fig. 38-21) and produces cyclic changes in VT (similar to supraglottic LFJV), facilitating maintenance of PaCO2 at near-normal limits and allowing HFJV to be adjusted as needed.136,137 HFJV builds up a continuous PEEP and promotes alveolar recruitment, maintaining PaCO2 even in the presence of the low FIO2 required for laser surgery.136–139 Safety of SHFJV is enhanced by an integrated port for continuous pressure (PIP and PEEP) and gas (FIO2 and EtCO2) monitoring at the end of the jet laryngoscope (see Fig. 38-21)137 and of an automatic pressure-triggered ventilator shutdown feature, similar to an isolated HFJV mode.

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


