Airway management is tailored to the type of injury, the nature and degree of airway compromise, and the patient’s hemodynamic and oxygenation status.
 Fast computed tomography technology with the capability of sagittal image reconstruction is replacing conventional multiple view plain radiographic evaluation of cervical spine injury. Further, magnetic resonance imaging is replacing flexion/extension plain radiographic evaluation of the relatively infrequent ligamentous injuries of the cervical spine.
Fast computed tomography technology with the capability of sagittal image reconstruction is replacing conventional multiple view plain radiographic evaluation of cervical spine injury. Further, magnetic resonance imaging is replacing flexion/extension plain radiographic evaluation of the relatively infrequent ligamentous injuries of the cervical spine.
 Penetrating neck injuries usually present with obvious clinical manifestations, whereas blunt cervical trauma may be more subtle.
Penetrating neck injuries usually present with obvious clinical manifestations, whereas blunt cervical trauma may be more subtle.
 Morbidity and mortality of flail chest is primarily related to underlying pulmonary contusion that develops over a period of a few hours after injury. A liberal indication for tracheal intubation of these patients may be associated with increased morbidity and mortality.
Morbidity and mortality of flail chest is primarily related to underlying pulmonary contusion that develops over a period of a few hours after injury. A liberal indication for tracheal intubation of these patients may be associated with increased morbidity and mortality.
 Head injury and hemorrhagic shock are the most common causes of traumatic death.
Head injury and hemorrhagic shock are the most common causes of traumatic death.
 Lethal triad or bloody vicious cycle refers to the development of acidosis, hypothermia, and coagulopathy, which, if untreated, may lead to death.
Lethal triad or bloody vicious cycle refers to the development of acidosis, hypothermia, and coagulopathy, which, if untreated, may lead to death.
 Approximately 10% of patients with hemorrhagic shock may have severe coagulopathy at the time of admission and the early operative phase, requiring hemostatic resuscitation with plasma, platelets, and coagulation factors.
Approximately 10% of patients with hemorrhagic shock may have severe coagulopathy at the time of admission and the early operative phase, requiring hemostatic resuscitation with plasma, platelets, and coagulation factors.
 The most important therapeutic maneuvers in head injured patients are normalization of intracranial pressure, cerebral perfusion pressure, and oxygen delivery.
The most important therapeutic maneuvers in head injured patients are normalization of intracranial pressure, cerebral perfusion pressure, and oxygen delivery.
 Brain ischemia is the most threatening consequence of head injury. By causing cerebral vasoconstriction, hyperventilation further aggravates ischemia.
Brain ischemia is the most threatening consequence of head injury. By causing cerebral vasoconstriction, hyperventilation further aggravates ischemia.
 The term blunt cardiac injury has replaced myocardial contusion and encompasses varying degrees of myocardial damage, coronary artery injury, and rupture of the cardiac free wall, the septum, or a valve.
The term blunt cardiac injury has replaced myocardial contusion and encompasses varying degrees of myocardial damage, coronary artery injury, and rupture of the cardiac free wall, the septum, or a valve.
 Transesophageal echocardiography is very useful in the trauma setting, providing information about right and left ventricular volume, ejection fraction, wall motion abnormalities, pulmonary hypertension, cardiac output, acute ischemia, blunt cardiac injury, cardiac septal or valvular damage, coronary artery injury, pericardial tamponade, and aortic injury.
Transesophageal echocardiography is very useful in the trauma setting, providing information about right and left ventricular volume, ejection fraction, wall motion abnormalities, pulmonary hypertension, cardiac output, acute ischemia, blunt cardiac injury, cardiac septal or valvular damage, coronary artery injury, pericardial tamponade, and aortic injury.
 In the trauma patient persistent hypotension is usually a result of bleeding, tension pneumothorax, neurogenic shock, and/or cardiac injury such as pericardial tamponade or myocardial contusion.
In the trauma patient persistent hypotension is usually a result of bleeding, tension pneumothorax, neurogenic shock, and/or cardiac injury such as pericardial tamponade or myocardial contusion.
 Inspired by military experience, many studies of civilian trauma have demonstrated the benefit of hemostatic resuscitation involving high ratios of fresh frozen plasma or platelets to packed red blood cell transfusion. However, many of these studies have been found to have survivor bias, necessitating further work in this area.
Inspired by military experience, many studies of civilian trauma have demonstrated the benefit of hemostatic resuscitation involving high ratios of fresh frozen plasma or platelets to packed red blood cell transfusion. However, many of these studies have been found to have survivor bias, necessitating further work in this area.
 Monitoring of blood coagulation status with thromboelastography is useful in bleeding patients receiving massive transfusion.
Monitoring of blood coagulation status with thromboelastography is useful in bleeding patients receiving massive transfusion.
 Prothrombin complex concentrates containing factors II, VII, IX, and X are available in the United States and are used primarily to reverse the effects of warfarin in acute trauma patients.
Prothrombin complex concentrates containing factors II, VII, IX, and X are available in the United States and are used primarily to reverse the effects of warfarin in acute trauma patients.
Multimedia
 Management of the Major Trauma Patient
Management of the Major Trauma Patient
 Nail Trachea Case
Nail Trachea Case
 Pneumothorax
Pneumothorax
Injury is responsible for 9% of the total annual mortality (5 million people) in the world.1 Traffic accidents alone killed 3,500 people every day in 2009; almost half of the victims were pedestrians, cyclists, and motorcyclists.2 Violence, encompassing homicides, suicides, and war-related injuries, is also estimated to kill about 1.5 million people every year in the world of whom the vast majority reside in low- and middle-income countries.3
In the United States, according to data from the National Safety Council intentional injuries (suicide, homicide, and assault) claimed 55,000 lives in 2008, while in 2010, unintentional (motor vehicle, falls, drowning, poisoning, etc.) mortality claimed 126,000 lives. Trauma, with an estimated 181,000 deaths per year, was the third leading cause of death after heart disease and cancer. Unintentional injuries were the fifth, suicides the tenth, and assault the fifteenth leading causes of death overall. For the age range between 15 and 31, accidents, suicide, and homicide were the three leading causes of death. Morbidity caused by injuries is far in excess of mortality; in 2010, a total of 37.9 million emergency room visits were related to unintentional injuries. The estimated cost of unintentional injuries alone that year was $731 billion, including the costs of fatal and nonfatal injuries, employer costs, vehicle damage, and fire losses.4
Approximately 75% of the hospital deaths from high-energy trauma such as motor vehicle accidents, falls, and gunshot or stab wounds occur within 48 hours after admission, most commonly from central nervous system (CNS), thoracic, abdominal, retroperitoneal, or vascular injuries.5 CNS injury and hemorrhage are the most common causes of early trauma mortality.6 Nearly one-third of these patients die within the first 4 hours after admission, representing the majority of operating room (OR) trauma deaths. Of the hospital deaths, 5% to 10% occur between the third and seventh day of admission, usually from CNS injuries, and the rest in subsequent weeks, most commonly as a result of multiorgan failure.5 Pulmonary thromboembolism and infectious complications may also contribute to mortality during this phase.5 Interestingly, injuries caused by low energy impacts, mainly from falls usually in the elderly, also produce significant mortality from head injury and complications of skeletal injuries. Of these deaths, 20% occur within 48 hours, 32% after 3 to 7 days, and 48% after 7 days. Pre-existing conditions such as congestive heart failure, cirrhosis, warfarin, and/or β-blocker usage increase the mortality rate in trauma patients.7
INITIAL EVALUATION AND RESUSCITATION
The strategy of initial management can be defined as a continuous, priority-driven process of patient assessment, resuscitation, and reassessment. The general approach to evaluation of the acute trauma victim has three sequential components: rapid overview, primary survey, and secondary survey (Fig. 52-1). Resuscitation is initiated, if needed, at any time during this continuum. Rapid overview takes only a few seconds and is used to determine whether the patient is stable, unstable, dying, or dead. The primary survey involves rapid evaluation of functions that are crucial to survival. The ABCs of airway patency, breathing, and circulation are assessed. Then a brief neurologic examination is performed, and the patient is examined for any external injuries that might have been overlooked.
Resuscitation is initiated, if needed, at any time during this continuum. Rapid overview takes only a few seconds and is used to determine whether the patient is stable, unstable, dying, or dead. The primary survey involves rapid evaluation of functions that are crucial to survival. The ABCs of airway patency, breathing, and circulation are assessed. Then a brief neurologic examination is performed, and the patient is examined for any external injuries that might have been overlooked.
FIGURE 52-1. Clinical sequence for initial management of the major trauma patient. CT, computed tomography; ER, emergency room; ICU, intensive care unit.
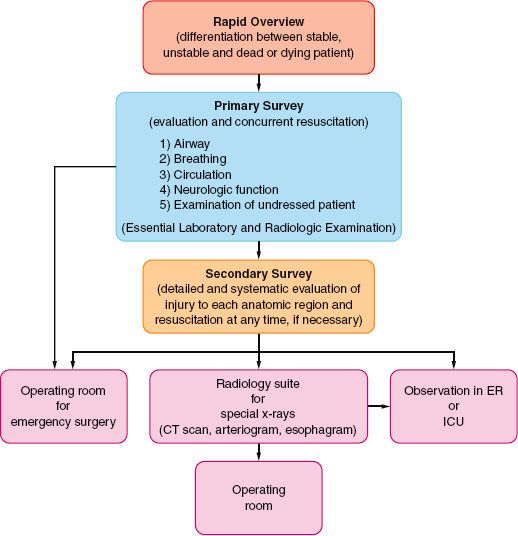
The secondary survey involves a more elaborate systematic examination of the entire body to identify additional injuries. Radiographic and other diagnostic procedures may also be performed if the stability of the patient permits. Within this general framework the anesthesiologist, aside from managing the airway, contributes as part of the team for evaluation and resuscitation, while gathering information needed for possible future anesthetic management.
Injuries may be missed during initial evaluation and even during emergency surgery, resulting in significant pain, complications, residual disability, delay of treatment, or death.8 Reported missed diagnoses include cervical spine, thoracoabdominal, pelvic, nerve, and external soft tissue injuries, and extremity fractures. Some of these injuries may present during administration of anesthesia, such as spinal cord damage in a patient with unrecognized cervical spine injury, massive intraoperative bleeding from an unrecognized thoracoabdominal injury during extremity surgery, or sudden intraoperative hypoxemia in a patient with unrecognized pneumothorax.
A tertiary survey within the first 24 hours after admission (which may include a period of anesthesia) can potentially diagnose the majority of clinically significant injuries missed during initial evaluation by repeating the primary and secondary examinations and reviewing the results of radiologic and laboratory testing.8
Airway Evaluation and Intervention
 Airway evaluation involves the diagnosis of any trauma to the airway or surrounding tissues, recognition and anticipation of the respiratory consequences of these injuries, and prediction of the potential for exacerbation of these or other injuries by any contemplated airway management maneuvers (see Chapter 27). Although nontraumatic causes of airway difficulty, such as pre-existing factors may be present, only the management of trauma-related problems is discussed in this section. Generally, the American Society of Anesthesiologists’s (ASA) difficult airway algorithm can be applied with certain modifications to various trauma airway management scenarios. For instance, cancellation of airway management when difficulty arises may not be an option. Likewise awake rather than asleep intubation or a surgical airway from the outset may be the preferred technique in some situations. The ASA’s difficult airway algorithm as modified for various trauma conditions is available.9 Airway management is tailored to the type of injury, the nature and degree of airway compromise, and the patient’s hemodynamic and oxygenation status.
Airway evaluation involves the diagnosis of any trauma to the airway or surrounding tissues, recognition and anticipation of the respiratory consequences of these injuries, and prediction of the potential for exacerbation of these or other injuries by any contemplated airway management maneuvers (see Chapter 27). Although nontraumatic causes of airway difficulty, such as pre-existing factors may be present, only the management of trauma-related problems is discussed in this section. Generally, the American Society of Anesthesiologists’s (ASA) difficult airway algorithm can be applied with certain modifications to various trauma airway management scenarios. For instance, cancellation of airway management when difficulty arises may not be an option. Likewise awake rather than asleep intubation or a surgical airway from the outset may be the preferred technique in some situations. The ASA’s difficult airway algorithm as modified for various trauma conditions is available.9 Airway management is tailored to the type of injury, the nature and degree of airway compromise, and the patient’s hemodynamic and oxygenation status.
Airway Obstruction
Airway obstruction is probably the most frequent cause of asphyxia and may result from posteriorly displaced or lacerated pharyngeal soft tissues; cervical or mediastinal hematoma; bleeding, secretions, or foreign bodies within the airway; and/or displaced bone or cartilage fragments. Bleeding into the cervical region may produce airway obstruction not only because of compression by the hematoma, but also from venous congestion and upper airway edema as a result of compression of neck veins. Signs of upper and lower airway obstruction include dyspnea, cyanosis, hoarseness, stridor, dysphonia, subcutaneous emphysema, and hemoptysis. Cervical deformity, edema, crepitation, tracheal tug and/or deviation, or jugular venous distention may be present before these symptoms appear and may help indicate that specialized techniques are required to secure the airway.
The initial steps in airway management are chin lift, jaw thrust, clearing of the oropharynx, placement of an oropharyngeal or nasopharyngeal airway, and, in inadequately breathing patients, ventilation with a self-inflating bag. Immobilization of the cervical spine and administration of oxygen should be applied simultaneously. Blind passage of a nasopharyngeal airway or a nasogastric or nasotracheal tube should be avoided if a basilar skull fracture is suspected because it may enter the anterior cranial fossa. A cuffed oropharyngeal airway (Combitube or King’s airway) or a laryngeal mask airway (LMA) may permit ventilation with a self-inflating bag, although neither provides protection against aspiration of gastric contents. They may be used as temporary measures and can serve as a bridge for a brief period to re-establish the airway patency or to facilitate intubation aided by a flexible fiberoptic bronchoscope (FOB). If they do not provide adequate ventilation, the trachea must be intubated immediately using either direct laryngoscopy or a cricothyroidotomy, depending on the results of airway assessment.
Maxillofacial, neck, and chest injuries, as well as cervicofacial burns, are the most common trauma-related causes of difficult tracheal intubation. Airway assessment should include a rapid examination of the anterior neck for feasibility of access to the cricothyroid membrane. Tracheostomy is not desirable during initial management because it takes longer to perform than a cricothyroidotomy and requires neck extension, which may cause or exacerbate cord trauma in patients with cervical spine injuries. Conversion to a tracheostomy should be considered later to prevent laryngeal damage if a cricothyroidotomy will be in place for more than 2 to 3 days. Possible contraindications to cricothyroidotomy include age younger than 12 years and suspected laryngeal trauma. Permanent laryngeal damage may result in the former, and uncorrectable airway obstruction may occur in the latter situation.
Full Stomach
A full stomach is a background condition in acute trauma: the urgency of securing the airway often does not permit adequate time for pharmacologic measures to reduce gastric volume and acidity. Thus, rather than relying on these agents, the emphasis should be placed on selection of a safe technique for securing the airway when necessary: rapid-sequence induction with cricoid pressure for those patients without serious airway problems, and awake intubation with sedation and topical anesthesia, if possible, for those with anticipated serious airway difficulties.
In agitated and uncooperative patients, topical anesthesia of the airway may be impossible, whereas administration of sedative agents may result in apnea or airway obstruction, with an increased risk of aspiration of gastric contents and inadequate conditions for tracheal intubation. After locating the cricothyroid membrane and denitrogenating the lungs, a rapid-sequence induction may be used to allow securing of the airway with direct laryngoscopy or, if necessary, immediate cricothyroidotomy. Personnel and material necessary to perform translaryngeal ventilation or cricothyroidotomy must be in place before induction of general anesthesia.
Head, Open Eye, and Contained Major Vessel Injuries
The principles of tracheal intubation are similar for these injuries. Apart from the need to ensure adequate oxygenation and ventilation, these patients require deep anesthesia and profound muscle relaxation before airway manipulation. This helps prevent hypertension, coughing, and bucking, and thereby minimizes intracranial, intraocular, or intravascular pressure elevation, which can result in herniation of the brain, extrusion of eye contents, or dislodgment of a hemostatic clot from an injured vessel, respectively. The preferred anesthetic sequence to achieve this goal in patients who are not hemodynamically compromised includes preoxygenation and opioid loading, followed by relatively large doses of an intravenous anesthetic and muscle relaxant. Hemodynamic responses to this sequence should be carefully monitored and promptly corrected. Systemic hypotension, intracranial pressure (ICP) elevation, and decreased cerebral perfusion pressure (CPP; CPP equals mean arterial pressure minus ICP) may occur whether cerebral autoregulation is present or absent in patients with head injuries, and if untreated it can produce secondary ischemic insults. Ketamine is probably contraindicated in patients with head and vascular injuries because it may increase both intracranial and systemic vascular pressures. However, no significant increase in intraocular pressure (IOP) has been documented. Any muscle relaxant, including succinylcholine, may be used as long as the fasciculation produced by this agent is inhibited by prior administration of an adequate dose of a nondepolarizing muscle relaxant. Alternatively, rocuronium can provide intubating conditions within 60 seconds with a dose of 1.2 to 1.5 mg/kg; neuromuscular blockade produced by this dose lasts approximately 2 hours. Of course, neither muscle relaxants nor intravenous anesthetics are indicated when initial assessment suggests a difficult airway. As in any other trauma patient, hypotension dictates either reduced or no intravenous anesthetic administration.
Cervical Spine Injury
Overall, 2% to 4% of blunt trauma patients have cervical spine (C-spine) injuries, of which 7% to 15% are unstable.10 The most common causes include high-speed motor vehicle accidents, falls, diving accidents, and gunshot wounds. Head injuries, especially those with low Glasgow coma scores (GCS) and focal neurologic deficits, are likely to be associated with C-spine injuries. Approximately 2% to 10% of head trauma victims have C-spine injuries, while 25% to 50% of patients with C-spine injuries have an associated head injury.10 The incidence of assault-related injuries depends on the mechanism, being highest after gunshot wounds (1.35%), lowest after stab wounds (0.12%), and intermediate after blunt trauma (0.4%) to the cervicothoracic region.
Initial Evaluation
Accurate and timely evaluation is important because 2% to 10% of blunt trauma induced C-spine injury patients develop new or worsening neurologic deficits after admission, partly attributable to delayed diagnosis and improper C-spine protection and/or manipulation.10 Often there is no time to evaluate the injury, and emergency airway management may have to be performed without ruling out C-spine injury while the patients are in a rigid collar and neck stabilizing devices. Clearance of the neck at the earliest possible time after airway management should be performed to minimize the complications associated with the collar, such as pressure ulceration, ICP elevation in head injured patients, compromised central venous access, and airway management challenges if reintubation is needed.
In the conscious patient with a suspected injury, diagnosis is relatively easy. According to the American National Emergency X-Radiography Utilization Study (NEXUS), a clinical evaluation revealing no posterior midline tenderness in the neck and no focal neurologic deficit in an injured patient with a normal level of alertness, no evidence of intoxication, and absence of painful distracting injury indicates a low probability of a C-spine injury, and there is thus no need for radiographic evaluation.11 Recently, however, it has been shown that a significant number of major trauma patients cleared by these criteria had clinically important unstable C-spine injuries requiring treatment. Therefore, routine computerized tomography (CT) in addition to clinical evaluation is recommended to rule out C-spine injury in major trauma victims.12 Probably the reason for the lower reliability of the NEXUS criteria is difficulty in evaluating distracting injuries.
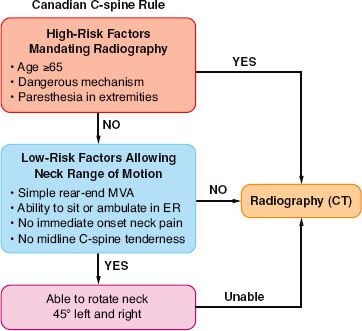
The Canadian C-spine rule for radiography after trauma is another tool designed to identify low-risk patients.10 With this diagnostic tool, proper answers to the following three questions eliminate the possibility of injury and the need for radiographic studies: (a) Is there any high-risk factor mandating radiography? (b) Are there low-risk factors that permit safe evaluation of the range of motion of the neck? (c) Can the patient rotate the neck laterally for 45 degrees in each direction without pain? (Fig. 52-2). Comparison of these two sets of criteria showed that the Canadian rule is more reliable than those for NEXUS in diagnosing C-spine injury in responsive patients.13
FIGURE 52-2. Canadian cervical spine rule designed to diagnose cervical spine injury and identify patients who require further radiographic (computed tomography) evaluation. (Adapted with permission from Stiell IG, Clement CM, McKnight RD, et al. The Canadian C-spine rule versus the NEXUS low-risk criteria in patients with trauma. N Engl J Med. 2003;349:2510.)
 For those patients who cannot be cleared clinically and thus require radiographic evaluation, it is now clear that the diagnostic capability of three-view plain films is inferior to that provided by modern multidetector CT scans. Currently in modern trauma centers radiographic evaluation of the C-spine is performed using thin cut CT images with sagittal and coronal reconstruction. There is, however, a subset of patients with a normal CT scan who are either comatose, obtunded or are awake but have neck pain. Given the fact that CT is not sensitive in picking up soft tissue and ligamentous injury, ruling out ligamentous C-spine injury in these patients is difficult and the diagnostic strategy is somewhat controversial. Dynamic fluoroscopy to obtain flexion/extension series has limited value because it is extremely low yield, relatively dangerous, and cost ineffective.14 It requires repeat examinations, it is difficult to identify specific ligamentous injury, and often the lower cervical spine cannot be visualized. In many trauma centers it is no longer performed.
For those patients who cannot be cleared clinically and thus require radiographic evaluation, it is now clear that the diagnostic capability of three-view plain films is inferior to that provided by modern multidetector CT scans. Currently in modern trauma centers radiographic evaluation of the C-spine is performed using thin cut CT images with sagittal and coronal reconstruction. There is, however, a subset of patients with a normal CT scan who are either comatose, obtunded or are awake but have neck pain. Given the fact that CT is not sensitive in picking up soft tissue and ligamentous injury, ruling out ligamentous C-spine injury in these patients is difficult and the diagnostic strategy is somewhat controversial. Dynamic fluoroscopy to obtain flexion/extension series has limited value because it is extremely low yield, relatively dangerous, and cost ineffective.14 It requires repeat examinations, it is difficult to identify specific ligamentous injury, and often the lower cervical spine cannot be visualized. In many trauma centers it is no longer performed.
Magnetic resonance imaging (MRI) is a reliable tool; a normal examination can conclusively exclude C-spine injury.15 It is thus the gold standard for ruling out C-spine injury. However, it is so sensitive that it can detect subtle injuries that are clinically insignificant. It cannot be performed in multiple trauma patients who have metallic skeletal fixators. It is expensive and requires patient transport. Finally, it cannot be performed in the first few days after injury, the period when airway management is most commonly performed. A more recently proposed approach, which is practiced in many countries and in many, but not all, trauma centers in the United States, is to rely on the CT study performed using multidetector devices with <3-mm cuts. The diagnostic capability of this method is excellent, with the possibility of missing 1 unstable C-spine injury in about 5,000 patients not cleared by clinical examination.16
There are certain situations that theoretically could be missed with CT examination. Acute rupture of a transverse atlantal ligament produces significant instability despite the absence of a neurologic deficit and normal alignment while the patient is supine on a CT scanner. Likewise, in a head-injured patient, a mild to moderate central cord syndrome, which is referred to as spinal cord injury without radiological abnormality, may be difficult to discern with a CT scan. Familiarity with these diagnostic strategies may help in the assessment of patients with C-spine injury before airway management.
Interestingly, published series describe very few instances of neurologic deficits related to airway management in C-spine–injured patients. Recently, Hindman et al.17 reviewed the closed claims data for perioperative cervical cord, nerve root, and spine injury between 1970 and 2007, which showed that overall airway management–related neurologic damage represented 11% of 48 claims. Nine patients in the series had unstable spines preoperatively and developed neurologic deficits. In two of these patients the injury was attributed to airway management following direct laryngoscopy and intubation without C-spine precautions. McLeod and Calder18 reviewed nine allegedly intubation-related cervical spinal cord injuries. Of these, three patients in two reports developed increased neurologic deficit after laryngoscopy and intubation without stabilization of the neck. It is likely that two of these patients are the same patients described by Hindman et al.17 Thus it is possible that airway management–related cervical cord injury in C-spine injured patients can occur, but if it does, it is rare.
Airway Management
Almost all airway maneuvers, including jaw thrust, chin lift, head tilt, and oral airway placement, result in some degree of C-spine movement.10 To secure the airway with direct laryngoscopy, manual in-line stabilization (MILS) of the neck is the standard care of these patients in the acute stage. A hard cervical collar alone, which is routinely placed, does not provide absolute protection, especially for rotational movements of the neck. MILS is best accomplished by having two operators in addition to the physician who is actually managing the airway. The first operator stabilizes and aligns the head in neutral position without applying cephalad traction. The second operator stabilizes both shoulders by holding them against the table or stretcher. The anterior portion of the hard collar, which limits mouth opening, may be removed after immobilization.
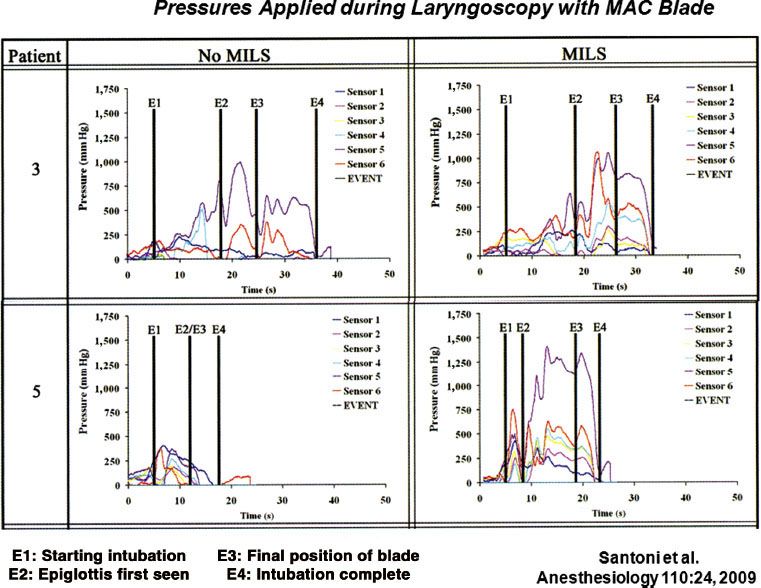
In the presence of MILS, the glottic view may be suboptimal in 10% to 15% of patients during direct laryngoscopy because of limitation of neck extension. Airway management may be further compromised in some patients because of enlargement of the prevertebral space by a hematoma from the vertebral fracture. Consequently, greater anterior pressure needs to be applied to the tongue by the laryngoscope blade to visualize the larynx. This increased anterior pressure is transmitted to the spine and can increase the movement of the unstable vertebral segment. Thus, the more the restriction of the glottic view during direct laryngoscopy, the greater the pressure on the tongue, the spine, and the unstable segment with potential displacement of the unstable fragment. Santoni et al.19 demonstrated that during various phases of direct laryngoscopy and intubation, the pressures exerted on the tongue and indirectly to the spine were greater with MILS than without MILS (Fig. 52-3). This finding confirmed the results of a videofluoroscopic study by Lennarson et al.20 who demonstrated significant anteroposterior displacement when MILS was applied to cadavers with destabilized C-spines.
FIGURE 52-3. Pressures applied by the MacIntosh laryngoscope blade on the tongue and indirectly on the cervical spine during various phases of direct laryngoscopy and intubation in two patients. Note that applied pressure is greatest from the time of final position of the blade to the completion of intubation, especially with application of manual in line stabilization of the head and neck. (Reproduced with permission from Santoni BG, Hindman BJ, Puttlitz CM, et al. Manual in line stabilization increases pressures applied by the laryngoscope blade during direct laryngoscopy and orotracheal intubation. Anesthesiology. 2009;110:24.)
Although convincing, these data should not eliminate the current standard practice of applying MILS during airway management of these patients. Currently, there is no scientifically rigorous clinical trial to show conclusively that airway management without MILS is associated with a favorable spinal cord outcome. Based on the available data, it is, however, reasonable to allow some relaxation of the MILS to improve the glottic view when visualization of the larynx is restricted.
Other measures and techniques, including the McCoy laryngoscope, rigid fiberoptic video laryngoscopes (Glidescope, Verathon, Bothell, Washington; Airtraq, Airtraq LLC, Fenton, Missouri; McGrath, LMA North America, San Diego, California), FOB, lightwand, translaryngeal (retrograde) intubation, and cricothyroidotomy, can be used to secure the airway in the acute phase in patients requiring cervical spine immobilization. So far the existing data suggest that neck motion with modern video laryngoscopes is similar to that produced by the Macintosh blade, although they provide better glottic views. A gum elastic bougie passed through the endotracheal tube, or a satin-sheathed stylet placed through its Murphy aperture, may also be helpful. They can be inserted through the larynx more easily than the tube itself because their small diameter does not block the view of the glottis during direct laryngoscopy. Cricoid pressure may optimize the view, but it should be applied with great care as it may produce undue motion of the unstable spine if excessive force is used. Supraglottic intubating airways with or without the aid of FOB can be used, but neck movement with these devices appears to be comparable to that produced by conventional laryngoscopes. Flexible fiberoptic laryngoscopy, lightwand, and possibly translaryngeal-guided intubation (see “Maxillofacial Injuries” section) cause almost no neck movement, but blood or secretions in the airway, a long preparation time, and difficulty in their use in comatose, uncooperative, or anesthetized patients reduce their utility during initial management. Nasotracheal intubation carries the risks of epistaxis, failure of intubation, and the possibility of entry of the endotracheal tube into the cranial vault or the orbit if there is damage to the cranial base or the maxillofacial complex. Absence of the usual signs of cranial base fracture (battle sign, raccoon eyes, or bleeding from the ear or the nose) cannot be relied on to exclude the possibility of its occurrence because with rapid prehospital transport, these signs may not be immediately apparent.
In the subacute phase of C-spine injury when time constraints, full stomach, and patient cooperation issues do not exist, the use of FOB in the awake, sedated patient with appropriate topical anesthesia is preferred. Advantages of this technique are minimal movement of the neck, positioning of the patient awake, maintenance of protective reflexes, and the ability to assess the neurologic status after intubation.
Direct Airway Injuries
Direct airway damage can occur anywhere between the nasopharynx and the bronchi. Sometimes more than one site may be involved, resulting in persistent airway dysfunction after one of the problems is corrected.21 Head, face, and neck injuries are more common in military personnel in combat than in the civilian population; effective torso protection by body armor used in combat leaves these regions unprotected.22
Maxillofacial Injuries
In addition to soft tissue edema of the pharynx and peripharyngeal hematoma, blood or debris in the oropharynx may be responsible for partial or complete airway obstruction in the acute stage of these injuries. Occasionally, teeth or foreign bodies in the pharynx may be aspirated into the airway causing some degree of obstruction, which may occur or be recognized only during attempts at tracheal intubation. Another problem is the dynamic nature of soft tissue injuries in this region. A hematoma or edema in the face, tongue, or neck may expand during the first several hours after injury and ultimately occlude the airway. Serious airway compromise may develop within a few hours in up to 50% of patients with major penetrating facial injuries or multiple trauma, caused by progressive inflammation or edema resulting from liberal administration of fluids.
The face, head, and neck are vulnerable to missile and explosion injuries.22 Although rare, massive hemorrhage, most frequently from the internal maxillary artery or its branches, and less frequently from the facial, external carotid, or sphenopalatine arteries and other small branches, may be life threatening, requiring anterior, posterior, or anteroposterior packing, intermaxillary fixation, and, when these measures are ineffective, angioembolization.23,24 Tracheal intubation or a surgical airway is necessary as an initial measure to avert airway compromise in these circumstances.
Fracture-induced encroachment on the airway or limitation of mandibular movement, pain, and trismus may limit mouth opening. Fentanyl in titrated doses of up to 2 to 4 μg/kg over a period of 10 to 20 minutes may produce an improvement in the patient’s ability to open the mouth if mechanical limitation is not present.
The selection of an airway management technique in the presence of a maxillofacial fracture is based on the patient’s presenting condition. Most patients with isolated facial injuries do not require emergency tracheal intubation. Surgery may be delayed for as long as a week with no adverse effect on the repair. Patients who present with airway compromise may be intubated using direct laryngoscopy; the decision about the use of anesthetics and muscle relaxants is based on the results of airway evaluation. When there is bleeding into the oropharynx, a flexible fiberoptic laryngoscope may be useless because of obstruction of the view. A retrograde technique, using a wire or epidural catheter passed through a 14-gauge catheter introduced into the trachea through the cricothyroid membrane, may be used if the patient can open his or her mouth. A surgical airway is indicated when there is airway compromise, when direct laryngoscopy has failed or is considered impossible, when the jaws will be wired, or when a tracheostomy will be performed anyway after definitive repair of the fracture.25 Tracheostomy may be indicated as an emergency procedure in the emergency room within a few minutes of arrival, as a delayed procedure in the OR for airway control within 12 hours of arrival, or as an elective procedure during definitive surgery in the OR more than 12 hours following admission to the hospital.22 Comminuted mandibular, midfacial bilateral LeFort III, and panfacial fractures are likely to be managed with tracheostomy for definitive surgery.25 To avoid the possible complications of tracheostomy, submental or submandibular intubation, which involves externalizing the proximal end of an orotracheal flexible armored tube through a small submental incision has been performed. Thus, the trachea remains surgically intact.26 Nasogastric or nasotracheal intubation should be avoided when a basilar skull or maxillary fracture is suspected because of the possibility that the tube may enter the cranium or the orbit. Hemorrhagic shock and life-threatening cranial, laryngotracheal, thoracic, and cervical spine injuries may accompany major facial fractures, and airway management must be tailored accordingly. The likelihood of cranial injury increases in midface fractures involving the frontal sinus, as well as the orbitozygomatic and orbitoethmoid complexes.
Cervical Airway Injuries
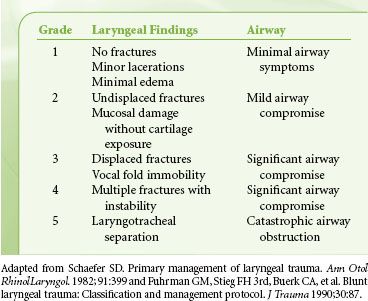
Injury to the cervical air passages can result from blunt or penetrating trauma. The incidence of blunt and penetrating laryngotracheal injuries admitted to major trauma centers is 0.34% and 4%, respectively.27 Similarly to maxillofacial injuries, wartime laryngotracheal injuries are more severe and occur more frequently (5% to 6%) than peacetime injuries (0.91%).28 Although the pharynx and esophagus are close to the cervical air passages, their involvement in peacetime trauma is less likely than airway injuries (0.08% after blunt and 0.9% after penetrating trauma).27 Clinical signs such as air escape, hemoptysis, and coughing are present in almost all patients with penetrating injuries, facilitating the diagnosis. In contrast, major blunt laryngotracheal damage may be missed, either because the patient is asymptomatic or unresponsive, or because suggestive signs and symptoms are missed in the initial evaluation. The typical presentation includes hoarseness, muffled voice, dyspnea, stridor, dysphagia, odynophagia, cervical pain and tenderness, ecchymosis, subcutaneous emphysema, and flattening of the thyroid cartilage protuberance (Adam’s apple). Whether the trauma is blunt or penetrating, attempts at blind tracheal intubation may produce further trauma to the larynx and complete airway obstruction if the endotracheal tube enters a false passage or disrupts the continuity of an already tenuous airway.29 Thus, whenever possible, intubation of the trachea should be performed using an FOB, or the airway should be secured surgically. A CT scan of the neck provides valuable information and should be performed before any airway intervention in all stable patients without respiratory and hemodynamic compromise. Originally, the severity of laryngeal injury was classified based on endoscopic findings. With modern CT equipment, information similar to that provided by FOB can be obtained with CT scanning. A classification of laryngeal injuries is depicted in Table 52-1.30,31
In contrast, major blunt laryngotracheal damage may be missed, either because the patient is asymptomatic or unresponsive, or because suggestive signs and symptoms are missed in the initial evaluation. The typical presentation includes hoarseness, muffled voice, dyspnea, stridor, dysphagia, odynophagia, cervical pain and tenderness, ecchymosis, subcutaneous emphysema, and flattening of the thyroid cartilage protuberance (Adam’s apple). Whether the trauma is blunt or penetrating, attempts at blind tracheal intubation may produce further trauma to the larynx and complete airway obstruction if the endotracheal tube enters a false passage or disrupts the continuity of an already tenuous airway.29 Thus, whenever possible, intubation of the trachea should be performed using an FOB, or the airway should be secured surgically. A CT scan of the neck provides valuable information and should be performed before any airway intervention in all stable patients without respiratory and hemodynamic compromise. Originally, the severity of laryngeal injury was classified based on endoscopic findings. With modern CT equipment, information similar to that provided by FOB can be obtained with CT scanning. A classification of laryngeal injuries is depicted in Table 52-1.30,31
TABLE 52-1. CLASSIFICATION OF LARYNGEAL INJURIES
The strategy for tracheal intubation depends on the clinical presentation.29 The tracheas of some patients with penetrating airway injuries, especially stab wounds, may be intubated through the airway defect without the need for anesthetics or optical equipment. The presence of cartilaginous fractures or mucosal abnormalities necessitates awake intubation with an FOB or awake tracheostomy.21 Laryngeal damage precludes cricothyroidotomy. Tracheostomy should be performed with extreme caution because up to 70% of patients with blunt laryngeal injuries may have an associated cervical spine injury.29 Uncooperative or confused patients may not tolerate awake airway manipulation. It may be best to transport these patients to the OR, induce anesthesia with inhalational agents, and intubate the trachea without muscle relaxants.29 Episodes of airway obstruction during spontaneous breathing under an inhalational anesthetic can be managed by positioning the patient upright in addition to the usual maneuvers.
Complete transection of the trachea is rare but when it occurs it is life threatening. The distal segment of the trachea retracts into the chest, causing airway obstruction either spontaneously or during airway manipulation. Surgery involves pulling up the distal end and performing an end-to-end anastomosis to the proximal segment or suturing it to the skin as a permanent tracheostomy. In extreme situations, such as complete or near-complete transection of the larynx and trachea, femorofemoral bypass or percutaneous cardiopulmonary support may be considered if time permits.32
Thoracic Airway Injuries
Whereas penetrating trauma can cause damage to any segment of the intrathoracic airway, blunt injury usually involves the posterior membranous portion of the trachea and the mainstem bronchi, usually within approximately 3 cm of the carina. A significant number of these injuries result from iatrogenic causes such as tracheal intubation.33 Pneumothorax, pneumomediastinum, pneumopericardium, subcutaneous emphysema, and a continuous air leak from the chest tube are the usual signs of this injury. They occur frequently but are not specific for thoracic airway damage. In patients intubated without the suspicion of a tracheal injury, difficulty in obtaining a seal around the endotracheal tube or the presence on a chest radiograph of a large radiolucent area in the trachea corresponding to the cuff suggests a perforated airway. Other radiographic findings include a radiolucent line along the prevertebral fascia due to air tracking up from the mediastinum, peribronchial air or sudden obstruction along an air-filled bronchus, and the “dropped lung” sign when complete intrapleural bronchial transection causes the apex of the collapsed lung to descend to the level of the hilum. Occasionally, simultaneous esophageal injury with a tracheoesophageal fistula may be present.34
Airway management is similar to that of cervical airway injury. Anesthetics, and especially muscle relaxants, may produce irreversible obstruction, presumably because of relaxation of structures that maintain airway patency in the awake patient. However, airway loss may also occur during attempts at awake intubation, often as a result of further distortion of the airway by the endotracheal tube, patient agitation, or rebleeding into the airway. After intubation of the trachea, the adequacy of airway intervention is evaluated mainly by auscultation and capnography. Pulmonary contusion, atelectasis, diaphragmatic rupture with thoracic migration of the abdominal contents, and pneumothorax may complicate the interpretation of chest auscultation. Likewise, carbon dioxide (CO2) elimination may be decreased or absent in shock and cardiac arrest.
The outcome after surgical repair of these injuries is often suboptimal and complicated by stump leak and empyema, suture line stenosis, or the need for tracheostomy or pneumonectomy. The recent trend is selective conservative management with an endotracheal tube placed using bronchoscopic guidance distal to the tracheal injury.35 Patients with lesions >4 cm, cartilaginous rather than membranous injuries, concomitant esophageal trauma, progressive subcutaneous emphysema, severe dyspnea requiring intubation and ventilation, difficulty with mechanical ventilation, pneumothorax with an air leak through the chest drains, and mediastinitis are still managed surgically. Those without these problems may be treated nonoperatively with a reasonable outcome.33,35
Management of Breathing Abnormalities
Of the several causes that may alter respiration after trauma, tension pneumothorax, flail chest, and open pneumothorax are immediate threats to the patient’s life and therefore require rapid diagnosis and treatment. Hemothorax, closed pneumothorax, pulmonary contusion, diaphragmatic rupture with herniation of abdominal contents into the thorax, and atelectasis from a mucous plug, aspiration, or chest wall splinting can also interfere with breathing and pulmonary gas exchange and deteriorate into life-threatening complications.
Although cyanosis, tachypnea, hypotension, neck vein distention, tracheal deviation, and diminished breath sounds on the affected side are the classic signs of tension pneumothorax, neck vein distention may be absent in hypovolemic patients and tracheal deviation may be difficult to appreciate. Diagnosis with an ultrasound probe placed on the second intercostal space on the suspected side to search for lung sliding and comet tail signs has the potential to provide rapid diagnosis; absence of these signs suggests the presence of pneumothorax.36 Inability to position most trauma patients upright and the likelihood of inadequate imaging decrease the diagnostic value of chest radiographs.37 In the supine position the “deep sulcus sign,” which results from the tendency of pleural air to track in the lateral and caudal regions, is usually the diagnostic chest radiographic sign of tension pneumothorax.37 The definitive diagnosis is made by CT scanning.36 However, in hypoxemic and hypotensive patients, immediate insertion of a 14-gauge angiocatheter through the fourth intercostal space in the midaxillary line or, at times, through the second intercostal space at the midclavicular line, is essential. There is no time for radiologic confirmation in this setting.
 A flail chest results from fractures of more than two sites of at least three adjacent ribs or rib fractures with associated costochondral separation or sternal fracture. An underlying pulmonary contusion with increased elastic recoil of the lung and work of breathing is the main cause of respiratory insufficiency or failure and resulting hypoxemia.38 It often develops over a 3- to 6-hour period, causing gradual deterioration of the chest radiograph and arterial blood gases (ABGs).38 Coexisting hemopneumothorax, paradoxical chest wall movement, and/or pain-induced splinting may contribute to the gas exchange abnormalities. Repeat evaluation by physical examination, chest radiograph, and ABG determinations is essential for early recognition of these complications. Preliminary bedside ultrasound examination showing replacement of the normal A lines with pathologic B lines also suggests pulmonary contusion.39 The fraction of lung volume contused, as determined by chest radiograph or CT scan, may be predictive of the subsequent development of acute respiratory distress syndrome (ARDS). The likelihood increases abruptly once the contusion volume exceeds 20% of total lung volume.40 Without significant gas exchange abnormalities, chest wall instability alone is not an indication for respiratory support. There is evidence that liberal use of tracheal intubation and mechanical ventilation in the presence of a flail chest or pulmonary contusion increases the rate of pulmonary complications and mortality and prolongs the hospital stay.38,41 Effective pain relief by itself can improve respiratory function and often prevents the need for mechanical ventilation. For this purpose, continuous epidural analgesia with local anesthetics and opioids, preferably directed to thoracic segments, provides better pain relief and ventilatory function than parenteral opioids, reducing morbidity and mortality in elderly patients with chest wall trauma.38 Other therapeutic measures include supplemental oxygen, continuous positive airway pressure (CPAP) of 10 to 15 cm water (H2O) by facemask, airway humidification, chest physiotherapy, incentive spirometry, bronchodilators, airway suctioning (using FOB, if necessary), and nutritional support.38 Overzealous infusion of fluids and transfusion of blood products may result in deterioration of oxygenation by worsening the underlying pulmonary injury.38
A flail chest results from fractures of more than two sites of at least three adjacent ribs or rib fractures with associated costochondral separation or sternal fracture. An underlying pulmonary contusion with increased elastic recoil of the lung and work of breathing is the main cause of respiratory insufficiency or failure and resulting hypoxemia.38 It often develops over a 3- to 6-hour period, causing gradual deterioration of the chest radiograph and arterial blood gases (ABGs).38 Coexisting hemopneumothorax, paradoxical chest wall movement, and/or pain-induced splinting may contribute to the gas exchange abnormalities. Repeat evaluation by physical examination, chest radiograph, and ABG determinations is essential for early recognition of these complications. Preliminary bedside ultrasound examination showing replacement of the normal A lines with pathologic B lines also suggests pulmonary contusion.39 The fraction of lung volume contused, as determined by chest radiograph or CT scan, may be predictive of the subsequent development of acute respiratory distress syndrome (ARDS). The likelihood increases abruptly once the contusion volume exceeds 20% of total lung volume.40 Without significant gas exchange abnormalities, chest wall instability alone is not an indication for respiratory support. There is evidence that liberal use of tracheal intubation and mechanical ventilation in the presence of a flail chest or pulmonary contusion increases the rate of pulmonary complications and mortality and prolongs the hospital stay.38,41 Effective pain relief by itself can improve respiratory function and often prevents the need for mechanical ventilation. For this purpose, continuous epidural analgesia with local anesthetics and opioids, preferably directed to thoracic segments, provides better pain relief and ventilatory function than parenteral opioids, reducing morbidity and mortality in elderly patients with chest wall trauma.38 Other therapeutic measures include supplemental oxygen, continuous positive airway pressure (CPAP) of 10 to 15 cm water (H2O) by facemask, airway humidification, chest physiotherapy, incentive spirometry, bronchodilators, airway suctioning (using FOB, if necessary), and nutritional support.38 Overzealous infusion of fluids and transfusion of blood products may result in deterioration of oxygenation by worsening the underlying pulmonary injury.38
Pulmonary contusion, respiratory insufficiency or failure despite adequate analgesia, clinical evidence of severe shock, associated severe head injury or injury requiring surgery, airway obstruction, and significant pre-existing chronic pulmonary disease are indications for tracheal intubation and mechanical ventilation. Outcome in these patients may be dependent on the pattern of ventilation. In head injury patients, unless the clinical evidence suggests imminent cerebral herniation, hyperventilation must be avoided because it increases cerebral vasoconstriction, thus decreasing perfusion with accumulation of cerebral lactic acid immediately after its institution.42 In hypovolemic patients, hyperventilation may interfere with venous return and cardiac output, leading to hypotension, further decrease in organ perfusion, and even cardiac arrest. Ventilation with low tidal volumes (6 to 8 mL/kg) and moderate positive end-expiratory pressure (PEEP), producing low inspiratory alveolar or plateau pressures, appears to be the best pattern to prevent deterioration of hemodynamics and decrease the likelihood of ARDS.43 In intubated, spontaneously breathing patients, airway pressure release ventilation, in which spontaneous breathing is superimposed on mechanical ventilation by intermittent sudden, brief decrease of CPAP, provides improved ventilation/perfusion (V./Q.) matching and systemic blood pressure, lower sedation requirements, greater oxygen (O2) delivery, shorter periods of intubation, and a decreased incidence of ventilator-associated pneumonia, which occurs in up to 30% of ventilated patients with pulmonary contusion.41,44,45 Severe unilateral pulmonary contusion unresponsive to these measures may be treated by differential lung ventilation via a double-lumen endobronchial tube. In bilateral severe contusions with life-threatening hypoxemia, high-frequency jet ventilation may enhance oxygenation and cardiac function, which may be compromised by concomitant myocardial contusion or ischemia.46
Systemic air embolism occurs mainly after penetrating lung trauma and blast injuries, or less frequently after blunt thoracic trauma that produces lacerations of both distal air passages and pulmonary veins.47 Positive-pressure ventilation after tracheal intubation may then result in entrainment of air into the systemic circulation. Hemoptysis, circulatory instability, and CNS dysfunction immediately after starting artificial ventilation, as well as detection of air in blood from the radial artery, establishes the diagnosis. Air bubbles may also be seen in the coronary arteries during thoracotomy. Surgical management involves immediate thoracotomy and clamping of the hilum of the lacerated lung. Respiratory maneuvers that minimize or prevent air entry into the systemic circulation include isolating and collapsing the lacerated lung by means of a double-lumen tube or ventilation with the lowest possible tidal volumes via a single-lumen tube.47 Transesophageal echocardiography (TEE) of the left side of the heart may permits visualization of air bubbles and their disappearance with therapeutic maneuvers.
Management of Shock
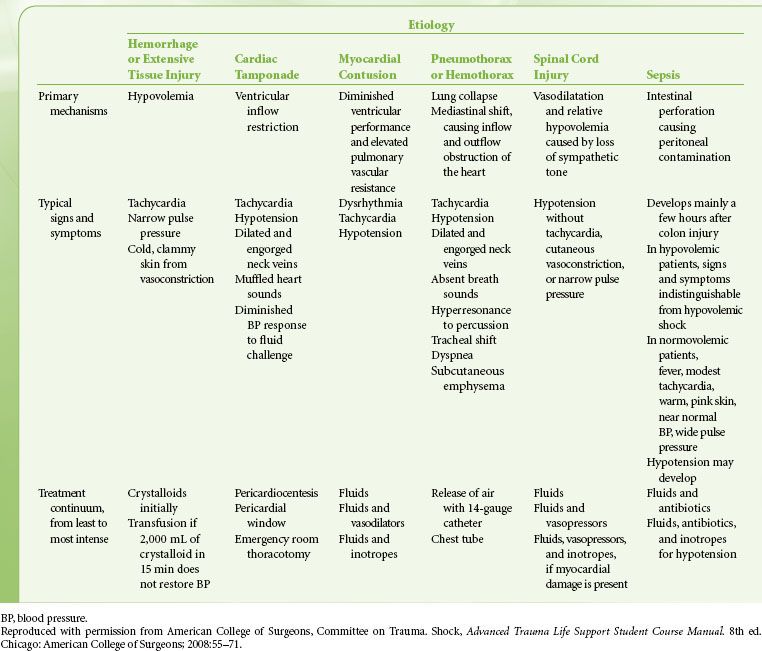
 Hemorrhage is the most common cause of traumatic hypotension and shock and is, after head injury, the second most common cause of mortality after trauma. Other causes are abnormal pump function (myocardial contusion, pericardial tamponade, pre-existing cardiac disease, or coronary artery or cardiac valve injury), pneumothorax or hemothorax, spinal cord injury, and rarely, anaphylaxis or sepsis (Table 52-2).
Hemorrhage is the most common cause of traumatic hypotension and shock and is, after head injury, the second most common cause of mortality after trauma. Other causes are abnormal pump function (myocardial contusion, pericardial tamponade, pre-existing cardiac disease, or coronary artery or cardiac valve injury), pneumothorax or hemothorax, spinal cord injury, and rarely, anaphylaxis or sepsis (Table 52-2).
TABLE 52-2. GUIDELINES FOR MANAGEMENT OF TRAUMATIC SHOCK
In bleeding patients the primary goal is the urgent surgical control of the source of bleeding. Certain types of bleeding sources, however, may be temporarily controlled with nonsurgical measures, such as finger compression of open neck injuries and tourniquet control of external bleeding from extremities. Tourniquets should be removed as soon as urgent surgical control is achieved to avoid pressure-induced nerve damage, skin necrosis, or limb ischemia.
Evaluation of the severity of hemorrhagic shock in the initial phase is based on the mechanism and anatomical pattern of injury, hemodynamic data, and the response to fluid resuscitation. Free falls from heights >6 m, high-energy deceleration impact, and high velocity gunshot wounds are very likely to produce major damage and bleeding. Thoracoabdominal and pelvic injuries also are likely to be associated with major bleeding. Immediate evaluation of these anatomical sites with radiographs of the chest and pelvis, focused abdominal sonography for trauma (FAST), CT, or rarely, diagnostic peritoneal lavage (DPL), is necessary. Patients with significant intra-abdominal fluid recognized with these tests and hemodynamic instability require immediate surgical intervention. Those who are suspected to have occult abdominal bleeding based on a high-risk mechanism of injury but who are hemodynamically stable must undergo further evaluation with CT. The modern multislice CT devices available in most trauma centers can provide early whole-body scanning with or without contrast within a few minutes.48 By using contrast, a delayed-phase CT can also demonstrate the active bleeding site.
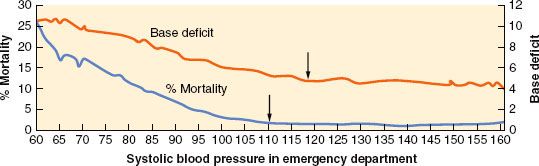
Clinical assessment using hemodynamic data is based on a few relatively insensitive and nonspecific clinical signs. For example, tachycardia, which is traditionally used as an index of hypovolemia, may be absent in up to 30% of hypotensive trauma patients because of increased vagal tone, chronic cocaine use, or other reasons.49 Inability of the patient to elevate the heart rate in the face of hypoperfusion is considered a predictor of increased mortality independent of severity of injury, systemic blood pressure, or the presence of a head injury.49 In contrast, by increasing catecholamine output, tissue injury and associated pain may maintain tachycardia and normal systemic blood pressure in the presence or absence of hypovolemia without necessarily increasing the cardiac index or tissue oxygen delivery. In fact, in this situation an increase in intestinal vascular resistance and a decrease in splanchnic blood flow may occur, and if prolonged, may allow entry of intestinal micro-organisms into the circulation and increase the likelihood of subsequent sepsis and organ failure.50–52 Thus, equating a normal heart rate and systemic blood pressure with normovolemia during initial resuscitation may lead to loss of valuable time for treating underlying occult hypovolemia or hypoperfusion. This is especially true in the elderly trauma population (age >65) in whom significant tissue hypoperfusion in the presence of normal blood pressure is more likely than in younger patients.53 Traditionally, the normal systolic blood pressure (SBP) is defined as 90 mm Hg. Recent findings suggest that trauma patients with this level or lower emergency department (ED) SBP have a higher mortality, higher blood lactate levels, and greater base deficits than civilian trauma patients with a SBP of 110 mm Hg and injured soldiers with a SBP of 100 mm Hg54,55 (Fig. 52-4). Thus, the optimal SBP in the trauma patient appears to be 100 to 110 mm Hg. Although traditional vital signs are relatively unreliable for recognizing life-threatening shock, heart rate, systemic blood pressure, pulse pressure, respiratory rate, urine output, and mental status are still used as early clinical indicators of the severity of hemorrhagic shock. (Table 52-3).50,56 Shock index (SI), a value derived by dividing the heart rate by the SBP, appears to be a more accurate indicator of early hemorrhagic shock and a predictor of mortality than the individual vital signs. In normal individuals, SI varies between 0.58 and 0.64 (mean 0.61) increasing from 0.70 to 0.80 (mean 0.75) after a moderate degree of blood loss. In the elderly, it has been demonstrated that age times SI identifies early shock and predicts mortality better than SI itself.57
FIGURE 52-4. Relationship between emergency department systolic blood pressure, base deficit, and overall mortality rate of trauma patients; head injury patients are not included. Note that mortality and base deficit decrease as systolic blood pressure increases, stabilizing at 110 mm Hg rather than at the generally accepted 90 mm Hg. BP, blood pressure. (Adapted with permission from Eastridge BJ, Salinas J, Wade CE, et al. Hypotension begins at 110 mm Hg: Redefining “hypotension” with data. J Trauma. 2007;63:291.)
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


