Fig. 17.1
The layout of the C4 cervical nerve root and the corresponding branch. MB medial branch, LB lateral branch, AP articular pillar (Reproduced with permission from Philip Peng Educational Series)
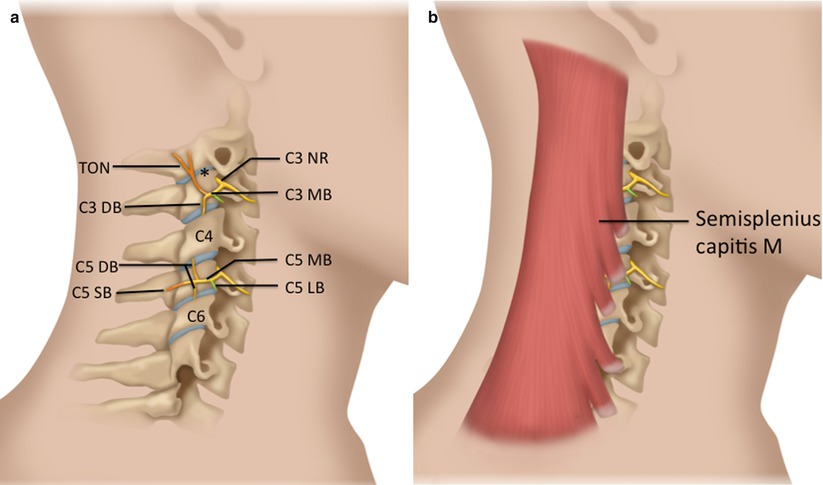
Fig. 17.2
(a) Schematic diagram to show the branches of cervical nerve root. NR nerve root, MB medial branch, LB lateral branch, TON third occipital nerve, DB deep branch of medial facet nerve, SB superficial branch of medial facet nerve. (b) Same diagram showing the overlying semispinalis capitis muscle (Reproduced with permission from Philip Peng Educational Series). * C2-3 facet joint
The superficial branch of C3 nerve root is well developed (the third occipital nerve, TON) and supplies C2–3 facet joint as it crosses the midportion of the C2–3 joint cleft. The medial branches’ cervical dorsal rami are bound to the periosteum by an investing fascia and held against the articular pillar by tendons of semispinalis capitis (Fig. 17.2).
Technique
The classic technique of performing both diagnostic facet nerve blocks and RF neurotomy involves fluoroscopic needle guidance (Fig. 17.3).

Fig. 17.3
X-ray picture showing the target of the facet medial branch block. The target is the intersection of the diagonal lines of the trapezoid (articular pillar). SP spinous process. (With permission of Dr. Andreas Siegenthaler)
Ultrasound imaging offers the advantage of being able to visualize the actual target nerves [10], which obviously is not possible with fluoroscopy. In a previous feasibility study performed on ten volunteers, the third occipital nerve was visible with ultrasound imaging and could reliably be anesthetized in most of the cases [11]. This opened the perspective of applying ultrasound imaging as an alternative to fluoroscopy in interventional diagnosis and treatment of neck pain. The important anatomic structures can reliably be identified with ultrasound imaging, even in a real chronic neck pain population, as determined in first exploratory study [10]. Not only the bony target can be identified, but also the medial branch itself, due to its superficial course (as opposed to the lumbar region). Further studies demonstrated the accuracy of ultrasound-guided cervical medial branch blocks, both in healthy volunteers [12] and in chronic neck pain patients [13–15].
Since the medial branch can be identified in most cases, it is expected that ultrasound imaging could facilitate the procedure of radiofrequency neurotomy in patients diagnosed with facet joint-mediated pain. The classic technique of radiofrequency neurotomy using fluoroscopy is to perform a matrix of about six thermal lesions in order to increase the chance of successful coagulation of the nerve [4], since the exact course of the nerve due to its variable course is not known. Being able to exactly determine the nerve course using ultrasound imaging is expected to decrease the number of thermal lesions needed. In 15 consecutive neck pain patients diagnosed with facet joint-mediated pain, radiofrequency neurotomy according to a shortened protocol based on prior ultrasound localization of the nerves reached the benchmark of the standard technique [8]. The author would like to emphasize that the radiofrequency procedure per se was performed solely under fluoroscopic imaging with a reduced number of thermal lesions performed according to the information of the exact nerve course gained by the prior ultrasound examination. Ultrasound is a subjective imaging technique, and verification of the exact electrode position, not least for legal reasons, is limited as compared to fluoroscopy.
Practical Aspects of Ultrasound-Guided Technique
With the patient placed in a lateral position, the lateral region of the neck first is scanned in a transverse plane in the area of the mastoid process, and by slowly moving the transducer in a caudal direction, the vertebral artery is identified and followed until it enters the transverse foramen of C2. Posterior the transverse foramen C2, the facet joint C2–3 is located. Here the transducer is turned 90° until it lies in a longitudinal plane to the neck. Here the typical image of the cervical facet joint region appears with each “hill” being a facet joint and each “groove” in between the joints corresponding to the articular pillar, where the medial branch can be identified as a hypoechoic structure, very much resembling a blood vessel (Fig. 17.4). The third occipital nerve (joint supplying nerve of the facet joint C2–3) is located on the joint cleft of the facet joint C2–3 (Fig. 17.5).

Fig. 17.4
Ultrasound anatomy of the cervical facet joint region cut in a longitudinal plane. * facet joint cleft. Arrows medial branch, which appears as a hypoechoic oval structure located in the middle of the “groove” between two facet joints. (With permission of Dr. Andreas Siegenthaler)










