Common Ultrasound-Guided Truncal and Cutaneous Blocks
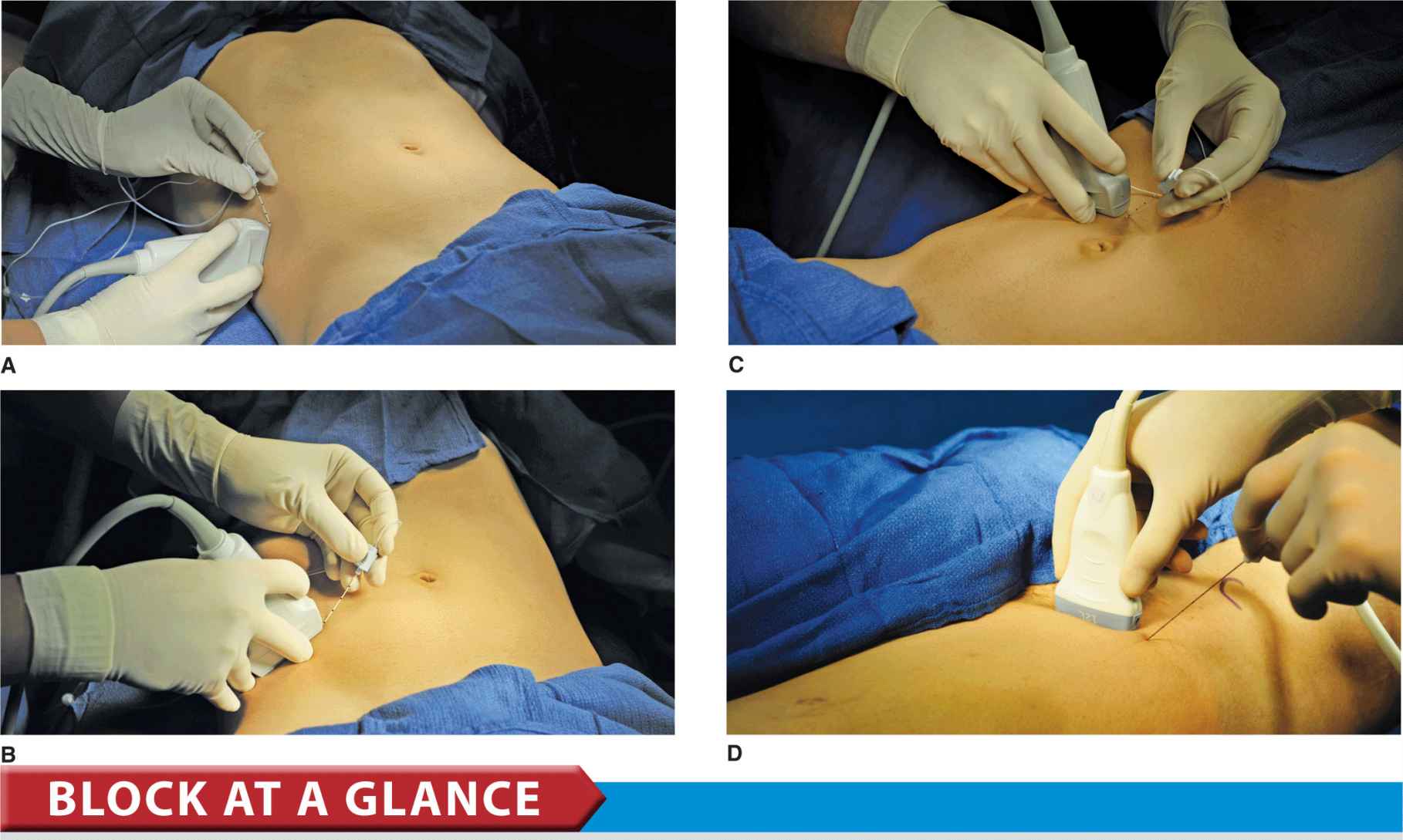
FIGURE 42.1-1. (A) Transducer position and needle insertion to accomplish a transverse abdominal plane block. (B) Transducer position and needle insertion to accomplish iliohypogastric and ilioinguinal nerve blocks. (C) Transducer position and needle insertion to accomplish rectus sheath block. (D) Transducer position and needle insertion to accomplish a lateral femoral cutaneous nerve (LFCN) block.
PART 1: ULTRASOUND-GUIDED TRANSVERSUS ABDOMINIS PLANE BLOCK
General Considerations
The ultrasound-guided transversus abdominis plane block, or TAP has become a commonly used regional anesthesia technique for a variety of indications. It is largely devoid of complications and can be performed time-efficiently, either at the beginning or the end of surgery for use as postoperative analgesia. Similar to ilioinguinal and iliohypogastric nerve blocks, the method relies on guiding the needle with ultrasound to the plane between the transversus abdominis and internal oblique muscles, to block the anterior rami of the lower six thoracic nerves (T7-T12) and the first lumbar nerve (L1). Injection of local anesthetic within the TAP potentially can provide unilateral analgesia to the skin, muscles, and parietal peritoneum of the anterior abdominal wall from T7 to L1, although in clinical practice, the extent of the block is variable.
Ultrasound Anatomy
The anterior abdominal wall (skin, muscles, and parietal peritoneum) is innervated by the anterior rami of the lower six thoracic nerves (T7-T12) and the first lumbar nerve (L1). Terminal branches of these somatic nerves course through the lateral abdominal wall within a plane between the internal oblique and transversus abdominis muscles. This intermuscular plane is called the transversus abdominis plane. Injection of local anesthetic within the TAP can result in unilateral analgesia to the skin, muscles, and parietal peritoneum of the anterior abdominal wall. The exact cephalad-caudad spread and extent of anesthesia and analgesia obtained with the TAP block is variable. This subject is not well researched; the actual coverage is likely dependent on the technique details, place of needle insertion (lateral-medial) and volume of local anesthetic injected. Additionally, the patient’s anatomical characteristics may also influence the spread of the injected solutions.
Imaging of the abdominal wall between the costal margin and the iliac crest reveals three muscle layers, separated by a hyperechoic fascia: the outermost external oblique (EOM), the internal oblique (IOM), and the transversus abdominis muscles (TAM) (Figures 42.1-2 and 42.1-3). Immediately below this last muscle is the transversalis fascia, followed by the peritoneum and the intestines below, which can be recognized as moving structures because of peristalsis. The nerves of the abdominal wall are not visualized consistently, although this is not necessary to accomplish a block.
FIGURE 42.1-2. Innervation of the anterior and lateral abdominal wall. IH, iliohypogastric nerve; IL, ilioinguinal nerve.
FIGURE 42.1-3. Schematic representation of the abdominal wall muscles.
Distribution of Blockade
The exact distribution of abdominal wall anesthesia following a TAP block has not been well documented or entirely agreed on by practitioners. The most fervent proponents of TAP technique maintain that reliable blockade of dermatomes T10-L1 can be achieved with moderate volumes of local anesthetic (e.g., 20–25 mL). Claims of blockade up to T7 after single injection of large volume have been made, but these results are not consistently reproduced in clinical practice. In our practice, some TAP blocks have resulted in complete anesthesia for inguinal herniorrhaphy; at other times, the results have been less consistent. Additional research is indicated to clarify the spread of anesthesia and factors that influence it.
Equipment
Equipment needed is as follows:
• Ultrasound machine with linear transducer (6–18 MHz), sterile sleeve, and gel (in very obese patients, and when a more posterior approach is used, a curved transducer might be needed)
• Standard nerve block tray
• Two 20-mL syringes containing local anesthetic
• A 50- to 100-mm, 20- to 21-gauge needle
• Sterile gloves
Landmarks and Patient Positioning
This block typically is performed with the patient in the supine position. The iliac crest and costal margin should be palpated and the space between them in the mid-axillary line (usually 8–10 cm) identified as the initial transducer location. The block is almost always performed under general anesthesia in pediatric patients; a common option for adults as well.
Technique
With the patient supine, the skin is disinfected and the transducer placed on the skin (Figure 42.1-4). The three muscle layers should be identified (Figures 42.1-5A and B). Sliding the transducer slightly cephalad or caudad will aid the identification. Once the transverse abdominal plane is identified, a skin wheal is made 2 to 3 cm medial to the medial aspect of the transducer, and the needle is inserted in-plane in a medial to lateral orientation (Figures 42.1-1A and 42.1-6). The needle is guided through the subcutaneous tissue, EOM, and IOM. A “pop” may be felt as the needle tip enters the plane between the two muscles. After gentle aspiration, 1 to 2 mL of local anesthetic is injected to verify the location of the needle tip (Figure 42.1-6). When injection of the local anesthetic appears to be intramuscular, the needle is advanced or withdrawn carefully 1 to 2 mm and another bolus is administered. This gesture is repeated until the correct plane is achieved.

FIGURE 42.1-4. Transducer position in the transverse abdominal, at the anterior axillary line, between the costal margin and the iliac crest.
FIGURE 42.1-5. (A) Ultrasound anatomy of the abdominal wall layers. (B) Labeled ultrasound anatomy of the abdominal wall layers, EOM, external oblique muscle; IOM, internal oblique muscle; TAM, transverse abdominis muscle.
FIGURE 42.1-6. Simulated needle insertion (1) and distribution of LA (blue shaded area) to accomplish transversus abdominis plane (TAP) block. Shown are the external oblique muscle (EOM), internal oblique muscle (IOM), and the transverse abdominal muscle (TAM). Needle tip is positioned in the tissue sheath between IOM and TAM.
In an adult patient, 20 mL of local anesthetic per side is usually sufficient for successful blockade. We most commonly use ropivacaine 0.25%. In children, a volume of 0.4 mL/kg per side is adequate for effective analgesia when using ultrasound guidance.
SUGGESTED READING
Abrahams MS, Horn JL, Noles LM, Aziz MF: Evidence-based medicine: ultrasound guidance for truncal blocks. Reg Anesth Pain Med 2010;35:S36-42.
Belavy D, Cowlishaw PJ, Howes M, Phillips F. Ultrasound-guided transversus abdominis plane block for analgesia after Caesarean delivery. Br J Anaesth. 2009;103:726-730.
Carney J, McDonnell JG, Ochana A, et al. The transversus abdominis plane block provides effective postoperative analgesia in patients undergoing total abdominal hysterectomy. Anesth Analg. 2008;107(6):2056.
Chiono J, Bernard N, Bringuier S, Biboulet P, Choquet O, Morau D, Capdevilla X: The ultrasound-guided transversus abdominis plane block for anterior iliac crest bone graft postoperative pain relief: a prospective descriptive study. Reg Anesth Pain Med 2010;35:(6)520-524.
Finnerty O, Carney J, McDonnell JG: Trunk blocks for abdominal surgery. Anaesthesia 2010; 65 Suppl 1:76-83.
Griffiths JD, Middle JV, Barron FA, Grant SJ, Popham PA, Royse CF: Transversus abdominis plane block does not provide additional benefit to multimodal analgesia in gynecological cancer surgery. Anesth Analg 2010;111(3):797-801.
Hebbard P. Subcostal transversus abdominis plane block under ultrasound guidance. Anesth Analg. 2008;106(2):674.
Hebbard P, Fujiwara Y, Shibata Y, Royse C. Ultrasound-guided transversus abdominis plane (TAP) block. Anaesth Intensive Care. 2007;35:616-617.
Hebbard PD, Royse CF: Lack of efficacy with transversus abdominis plane block: is it the technique, the end points, or the statistics? Reg Anesth Pain Med 2010;35:324.
Heil JW, Ilfeld BM, Loland VJ, Sandhu NS, Mariano ER: Ultrasound-guided transversus abdominis plane catheters and ambulatory perineural infusion for outpatient inguinal hernia repair. Reg Anesth Pain Med 2010;35(6):556-558.
Kanazi GE, Aouad MT, Abdallah FW, Khatib MI, Adham AM, Harfoush DW, Siddik-Sayyid SM: The Analgesic Efficacy of Subarachnoid Morphine in Comparison with Ultrasound-Guided Transversus Abdominis Plane Block After Cesarean Delivery: A Randomized Controlled Trial. Anesth Analg 2010;111:475-481.
Lancaster P, Chadwick M. Liver trauma secondary to ultrasound-guided transversus abdominis plane block. Br J Anaesth. 2010;104:509-510.
Lee TH, Barrington MJ, Tran TM, Wong D, Hebbard PD. Comparison of extent of sensory block following posterior and subcostal approaches to ultrasound-guided transversus abdominis plane block. Anaesth Intensive Care. 2010;38:452-460.
McDonnell JG, Curley G, Carney J, et al. The analgesic efficacy of transversus abdominis plane block after cesarean delivery: a randomized controlled trial. Anesth Analg. 2008;106(1):186.
McDonnell JG, O’Donnell B, Curley G, et al. The analgesic efficacy of transversus abdominis plane block after abdominal surgery: a prospective randomized controlled trial. Anesth Analg. 2007;104(1):193.
McDonnell JG, O’Donnell BD, Farrell T, et al. Transversus abdominis plane block: a cadaveric and radiological evaluation. Reg Anesth Pain Med. 2007;32(5):399.
Mukhtar K, Khattak I: Transversus abdominis plane block for renal transplant recipients. Br J Anaesth 2010;104:663-664.
Niraj G, Kelkar A, Fox AJ. Application of the transversus abdominis plane block in the intensive care unit. Anaesth Intensive Care. 2009;37:650-652.
O’Connor K, Renfrew C: Subcostal transversus abdominis plane block. Anaesthesia 2010;65:91-92.
Petersen PL, Mathiesen O, Torup H, Dahl JB. The transversus abdominis plane block: a valuable option for postoperative analgesia? A topical review. Acta Anaesthesiol Scand. 2010;54:529-535.
Rafi AN. Abdominal field block: a new approach via the lumbar triangle. Anaesthesia. 2001;56(10):1024.
Rozen WM, Tran TM, Ashton MW, et al. Refining the course of the thoracolumbar nerves: a new understanding of the innervation of the anterior abdominal wall. Clin Anat. 2008;21(4):325.
Shibata Y, Sato Y, Fujiwara Y, et al. Transversus abdominis plane block. Anesth Analg. 2007;105(3):883; author reply 883.
Suresh S, Chan VW. Ultrasound guided transversus abdominis plane block in infants, children and adolescents: a simple procedural guide for their performance. Paediatr Anaesth. 2009;19:296-299.
Tran TM, Ivanusic JJ, Hebbard P, et al. Determination of spread of injectate after ultrasound-guided transversus abdominis plane block: a cadaveric study. Br J Anaesth. 2009;102(1):123.
Walker G: Transversus abdominis plane block: a note of caution! Br J Anaesth 2010;104:265.
Walter EJ, Smith P, Albertyn R, et al. Ultrasound imaging for transversus abdominis blocks. Anaesthesia. 2008;63(2):211.
PART 2: ULTRASOUND-GUIDED ILIOHYPOGASTRIC AND ILIOINGUINAL NERVE BLOCKS
General Considerations
Ilioinguinal and iliohypogastric nerves are contained in a well-defined tissue plane between the transversus abdominis and internal oblique muscles. The ability to easily image the musculature of the abdominal wall makes blocking these two nerves much more exact than the “feel-based” blind technique.
Ultrasound Anatomy
Imaging of the abdominal wall medial and superior to the ASIS reveals three muscle layers, separated by hyperechoic fascia: the outermost external oblique (EOM), the internal oblique (IOM), and the transversus abdominis muscles (TAM) (Figures 42.2-1A and B). Immediately below transversus abdominus muscle is the fascia transversalis, located just above the peritoneum and the abdominal cavity below, easily recognized as moving structures due to peristalsis. The hyperechoic osseous prominence of the anterior-superior iliac spine (ASIS) is a useful landmark which can be used as a reference, and is seen on the lateral side of the US image in Figure 42.2-1. The iliohypogastric and ilioinguinal nerves pierce the TAM above the ilium and lie in the plane between the TAM and the IOM. They are often seen side by side or up to 1 cm apart, and they typically appear as hypoechoic ovals. Use of color Doppler may be useful to identify the deep circumflex iliac artery, which lies adjacent to the nerves in the same plane as an additional landmark useful in identifying the nerves.
FIGURE 42.2-1. (A) Ultrasound anatomy of the iliohypogastric and ilioinguinal nerve. (B) Labeled ultrasound anatomy of the iliohypogastric and ilioinguinal nerve, ASIS, anterior superior iliac spine; EOM, external oblique muscle; IOM, internal oblique muscle; TAM, transverse abdominal muscle; IiN, ilioinguinal nerve; IhN, iliohypogastric nerve.
Distribution of Blockade
Block of the iliohypogastric and ilioinguinal nerves results in anesthesia of the hypogastric region, the inguinal crease, the upper medial thigh, the mons pubis, part of the labia, the root of the penis, and the anterior part of the scrotum. There is considerable variation in sensory distribution between individuals.
Equipment
Equipment needed is as follows:
• Ultrasound machine with linear transducer (6–18 MHz), sterile sleeve, and gel
• Standard nerve block tray
• Syringe(s) with 20 mL of local anesthetic
• 50-100 mm, 21-22 gauge needle
• Sterile gloves
Landmarks and Patient Positioning
The block of the iliohypogastric and ilioinguinal nerves is done in supine position. Palpation of the ASIS provides the initial landmark for transducer placment. This block is often performed under general anesthesia, particularly in pediatric patients.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


