CHAPTER 7 TRAUMA SYSTEMS AND TRAUMA TRIAGE ALGORITHMS
Trauma is a major national health care problem that affects one of four U.S. citizens annually. Traumatic injury, both accidental and intentional, is the leading cause of death in the United States for people aged 1 to 34 years. There are as many as 150,000 trauma deaths and approximately 80,000 others who sustain long-term disability each year with annual costs of more than $260 billion for trauma injury and treatment when loss of future productivity is considered. The most common fatal injuries in the country result form motor vehicle crashes, followed closely by gunshot wounds. Driving while impaired by alcohol is the most frequent cause of fatal motor vehicle crashes and accounts for 40% of traffic fatalities. The causes of traumatic death vary considerably depending on demographics. Urban and politically unstable areas typically have a higher incidence of penetrating trauma, whereas rural and stable communities have a predominance of blunt injuries, usually vehicular accidents. Nonetheless, causes of death after injury are remarkably similar. Central nervous system injury accounts for approximately half of all fatalities; hemorrhage for 35%; and sepsis, multiple organ failure, and pulmonary embolism combine for approximately 15%. With the introduction of trauma systems during the last three decades, the incidence of preventable death has dropped from approximately 25% to less than 5%. This is the result of improvements in care both for acute head injuries and for control of hemorrhage. In addition, the incidence of late death attributable to sepsis and multiple organ failure has diminished, possibly as a result of better and early resuscitation. The responsibility of the trauma surgeon encompasses the early recognition of injury, resuscitation, and then definitive care of the patient. As we improve the operative and intensive care rendered to trauma patients, we are beginning to reach the flat portion of the outcome curve. The area of injury prevention is still open to substantial improvement. To reduce the morbidity and mortality from trauma, surgeons must take a more active role in the prevention of trauma at the community level. Studies have shown the effect of these systems on the improvement of trauma care, with outcomes better than those predicted for some study populations. The necessary elements of a trauma system have been defined. These include four primary patient needs—access to care, prehospital care, hospital care, and rehabilitation. In addition, five issues require social and political solutions to supplement medical efforts: prevention, disaster medical planning, patient education, research, and rational financial planning. Recent federal legislation (The Trauma Care Systems Planning and Development Act) authorized planning, implementation, and development of statewide trauma care systems.
TRAUMA SYSTEMS
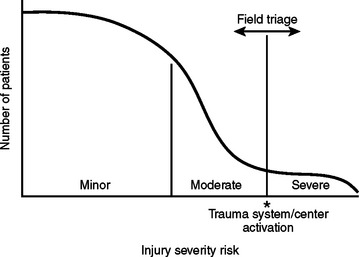
Major trauma patients are those with either a severe injury or a risk for severe injury. A severe injury is one that could result in morbidity or mortality, and is classically defined as an injury with an Injury Severity Score (ISS) of 16 or higher. On initial evaluation, these patients typically have abnormal vital signs or a significant anatomical injury. However, triage is often inexact due to patients’ variable physiological responses to trauma. In some patients, minor injuries can result in morbidity or mortality due to the patient’s age and/or comorbid factors, and some patients may have a delayed physiological response to trauma. Patients involved in a high-energy event are at risk for severe injury. Five to 15% of these patients, despite normal vital signs and no apparent anatomical injury on initial evaluation, will have a severe injury discovered after full trauma evaluation with serial observations (Figure 1).
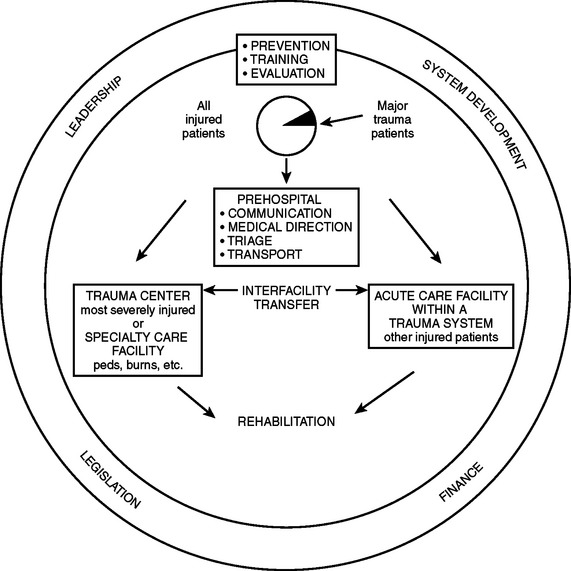
Current systems (“exclusive systems”) often rely on overtriage to trauma centers, and often an exaggerated and unnecessary response from trauma professionals. Such systems may cause overtreatment of certain patients, unnecessary expenses, burnout of participants, and underutilization of certain health care resources, including personnel. In spite of these excesses, such systems may still run the risk of not treating all injured patients, including not appropriately treating all major trauma patients. Undertriage runs the obvious risk of excluding some major trauma patients from receiving appropriate care. An inclusive system uses a tiered response to provide appropriate delivery, evaluation, and care for all patients, including the major trauma patient, in a cost-effective manner. One example of an inclusive trauma system is patient triage designed to care for major trauma patients by matching patient severity to facility in a timely manner. Considerations in triage include injury severity, injury severity risk, time and distance from site of injury to definitive care, inter-hospital transfers considering guidelines for immediate versus postintervention transports, and factors that activate the regional system (Figure 2).
SUPPORT FOR REGIONALIZED TRAUMA CARE
Although regionalization of trauma care has the inevitable consequence of increased prehospital transport times, particularly in rural areas removed from large trauma centers, some states have designed inclusive systems in which a large number of smaller centers have been designated as lower-level trauma centers. One of the primary functions of a statewide trauma system is to oversee the initiation of standardized protocols intended to ensure the timely triage and transfer of severely injured patients to facilities with appropriate therapeutic resources. Several studies document increased trauma center use and enhanced patient outcomes among metropolitan trauma centers after implementation of a regionalized trauma system.
INITIAL APPROACH TO THE CRITICALLY INJURED PATIENT
Prehospital Care: Intervention at Injury Site
Resuscitation and evaluation of the trauma patient begins at the injury site. The goal is to get the right patient to the right hospital at the right time for definitive care. First responders (typically, firefighters and police) provide rapid basic trauma life support (BTLS) and are followed by paramedics and fight nurses with advanced trauma life support (ATLS) skills. Medical control is ensured by pre-established field protocols, radio communication with a physician at the base hospital, and subsequent trip audits. Management priorities of BTLS on the scene are (1) to access and control the scene for the safety of the patient and the prehospital care providers, (2) to tamponade external hemorrhage with direct pressure, (3) to protect the spine after blunt trauma, (4) to clear the airway of obstruction and provide supplemental inspired oxygen, (5) to extricate the patient, and (6) to stabilize long-bone fractures. Whereas the benefits of BTLS are undisputed, the merits of the more advanced interventions remain controversial.1,2 Airway access, once considered a major asset of the care provided by paramedics and flight nurses, has now been questioned, not only because missed tracheal intubation is a concern but also because unintentional hyperventilation (hypocarbia) is detrimental in the setting of traumatic brain injury (TBI) and during cardiopulmonary resuscitation (CPR).3–5 Moreover, the value of intravenous fluid administration remains controversial.6,7
Field Triage
Prehospital trauma scores have been devised to identify critically injured trauma victims, who represent about 10%–15% of all injured patients. When it is geographically and logistically feasible, critically injured patients should be taken directly to a designated Level I trauma center or to a Level II trauma center if a Level I trauma center is more than 30 minutes away. The currently available field trauma scores, however, are not entirely reliable for identifying critically injured patients8: to capture a sizable majority of patients with life-threatening injuries, a 50% overtriage is probably necessary. Advance transmission of key patient information to the receiving trauma center facilitates the organization of the trauma team and ensures the availability of ancillary services9 (Figures 3 and 4).
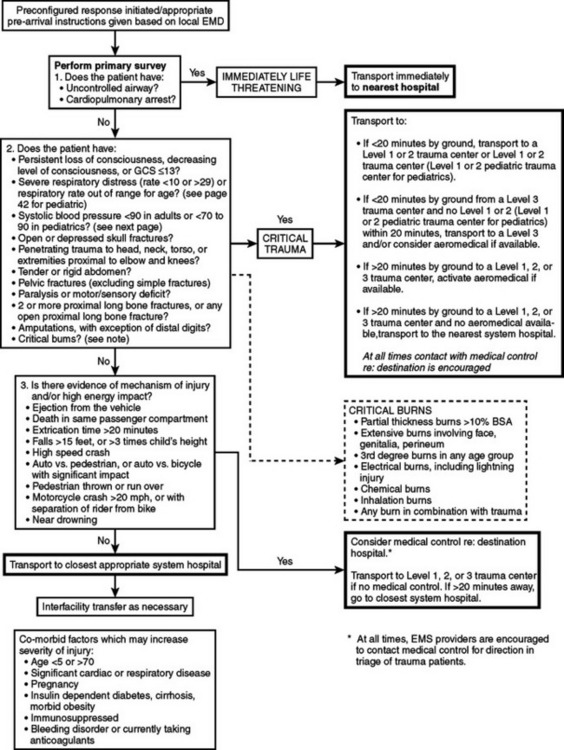
Figure 3 Trauma field triage criteria and point-of-entry plan for adult patients.
(From Commonwealth of Massachusetts, Department of Public Health.)
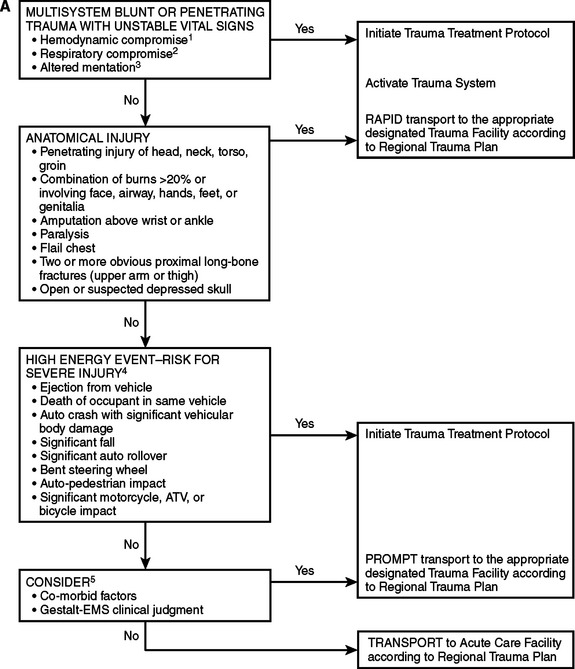
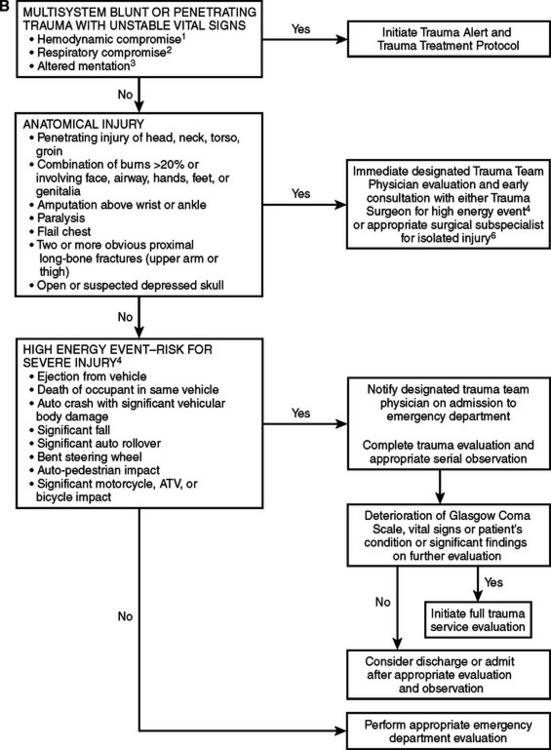
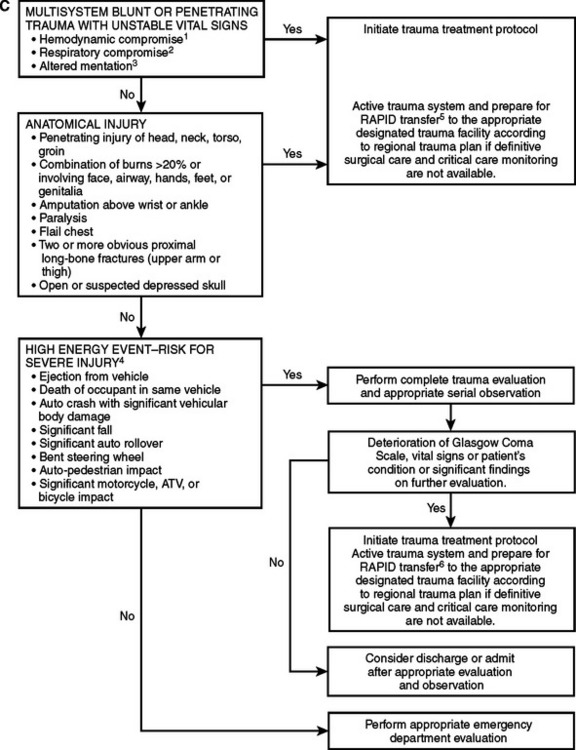
Figure 4 Adult triage, transport, and transfer guidelines: Oklahoma model trauma triage algorithms for (A) prehospital, (B) Level I/II trauma center, and (C) Level III/IV trauma center. For prepubescent patients, refer to the pediatric trauma algorithm (Figure 5). 1. In addition to hypotension, other early signs of hypovolemia may include pallor, tachycardia, or diaphoresis. 2. Tachypenia (hyperventilation) alone will not necessarily initiate this level of response. 3. Altered sensorium secondary to sedative-hypnotic will not necessarily initiate this level of response. 4. High-energy event signifies a large release of uncontrolled energy. Patient is assumed injured until proven otherwise, and multisystem injuries might exist. Determinants to be considered by medical professionals are direction and velocity of impact, patient kinematics and physical size, and the residual signature of energy release (e.g., major vehicle damage). 5. Clinical judgment must be exercised and may upgrade to a high level of response and activation. Age and comorbid conditions should be considered in the decision. 6. Isolated blunt or penetrating trauma not associated with a high-energy event with a potential for multisystem injury.
(Based on American College of Emergency Physicians Guidelines. Approved by the Triage, Transport, and Transfer Committee of the Oklahoma State Trauma Advisory Council, October 27, 1995, and the Oklahoma Emergency Medical Services Advisory Council on January 24, 1997.)
GUIDELINES FOR WITHHOLDING OR TERMINATION OF RESUSCITATION IN PREHOSPITAL CARDIOPULMONARY ARREST
Injury is the leading cause of death for Americans between age 1 and 44 years. The EMS system is the portal into the medical system for many of the most seriously injured trauma victims. Some of these patients will be unsalvageable due to the extent of their injuries. In order to preserve dignity and conserve precious human and financial resources, as well as to minimize risks to the health care workers involved, patients who can be predicted to be unsalvageable should not be transported emergently to the emergency department (ED) or trauma center. The National Association of EMS Physicians (NAEMSP) and the American College of Surgeons Committee on Trauma (COT) support out-of-hospital withholding or termination of resuscitation for adult traumatic cardiopulmonary arrest (TCPA) patients who meet specific criteria. The literature review of prehospital TCPA is extrapolated from emergency thoracotomy research. This research is retrospective in nature, therefore limiting the validity of the conclusions. The guidelines appear in Table 1.
Table 1 Guidelines for Withholding or Termination of Resuscitation in Prehospital Cardiopulmonary Arrest
| Resuscitation efforts may be withheld in any blunt trauma patient who, based on out-of-hospital personnel’stient assessment, is found apneic, pulseless, and without organized ECG activity upon the arrival of EMS at the scene. |
| Victims of penetrating trauma found apneic and pulseless by EMS, based on their patient assessment, should be rapidly assessed for the presence of other signs of life, such as papillary reflexes, spontaneous movement, or organized ECG activity. If any of these signs are present, resuscitation should be performed and the patient transported to the nearest emergency department or trauma center. If these signs of life are absent, resuscitation efforts may be withheld. |
| Resuscitation efforts should be withheld in victims of penetrating or blunt trauma with injuries obviously incompatible with life, such as decapitation or hemi-corpectomy. |
| Resuscitation efforts should be withheld in victims of penetrating or blunt trauma with evidence of a significant time lapse since pulselessness, including dependent lividity, rigor mortis, and decomposition. |
| Cardiopulmonary arrest patients in whom the mechanism of injury does not correlate with clinical condition, suggesting a nontraumatic cause of the arrest, should have standard resuscitation initiated. |
| Termination of resuscitation efforts should be considered in trauma patients with EMS-witnessed cardiopulmonary arrest and 15 minutes of unsuccessful resuscitation and cardiopulmonary resuscitation (CPR). |
| Traumatic cardiopulmonary arrest patients with transport time to an emergency department or trauma center of more than 15 minutes after the arrest is identified may be considered nonsalvageable, and termination of resuscitation should be considered. |
| Guidelines and protocols for TCPA patients who should be transported must be individualized for each EMS system. Consideration should be given to factors such as the average transport time within the system, the scope of practice of the various EMS providers within the system, and the definitive care capabilities (trauma centers) within the system. Airway management and intravenous line placement should be accomplished during transport when possible. |
| Special consideration must be given to victims of drowning and lightning strike and in situations where significant hypothermia may alter prognosis. |
| EMS providers should be thoroughly familiar with the guidelines and protocols affecting the decision to withhold or terminate resuscitative efforts. |
| All termination protocols should be developed and implemented under the guidance of the system EMS medical director. On-line medical control may be necessary to determine the appropriateness of terminating resuscitation. |
| Policies and protocols for terminating resuscitation efforts must include notification of the appropriate law enforcement agencies and notification of the medical examiner or coroner for final disposition of the body. |
| Families of the deceased should have access to resources, including clergy, social workers, and other counseling personnel, as needed. EMS providers should have access to resources for debriefing and counseling as needed. |
| Adherence to policies and protocols governing termination of resuscitation should be monitored through a quality review system. |
Initial Electrocardiographic Rhythm
There is some evidence that the initial ECG rhythm obtained at the scene by EMS may be predictive of survival. All of the studies combined by Batistella et al.,10 Fulton et al., Esposito et al.,9 and Aprahamian suggest that the presence of an ECG rhythm such as asystole, idioventricular rhythm, or severe bradycardia is indicative of an unsalvageable patient. Patients with a sinus-based pulseless electrical activity may represent a potentially salvageable subset of TCPA patients. Given that the TCPA is a critical event, the presence of any abnormal ECG pattern as an indicator of survival has limited significance. Blunt and penetrating injury as the cause of the TCPA was not distinguished in these studies, and given that blunt injury causing TCPA is associated with a very poor survival rate, it may be that survivors of TCPA may have penetrating trauma as their inciting event.
Related posts:
 THE DEVELOPMENT OF TRAUMA SYSTEMS
THE DEVELOPMENT OF TRAUMA SYSTEMS
 DELIVERING MULTIDISCIPLINARY TRAUMA CARE: CURRENT CHALLENGES AND FUTURE DIRECTIONS
DELIVERING MULTIDISCIPLINARY TRAUMA CARE: CURRENT CHALLENGES AND FUTURE DIRECTIONS
 GASTRIC INJURIES
GASTRIC INJURIES
 PALLIATIVE CARE IN THE TRAUMA INTENSIVE CARE UNIT
PALLIATIVE CARE IN THE TRAUMA INTENSIVE CARE UNIT
 TRAUMATIC BRAIN INJURY: PATHOPHYSIOLOGY, CLINICAL DIAGNOSIS, AND PREHOSPITAL AND EMERGENCY CENTER CARE
TRAUMATIC BRAIN INJURY: PATHOPHYSIOLOGY, CLINICAL DIAGNOSIS, AND PREHOSPITAL AND EMERGENCY CENTER CARE
 NOSOCOMIAL PNEUMONIA
NOSOCOMIAL PNEUMONIA
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


