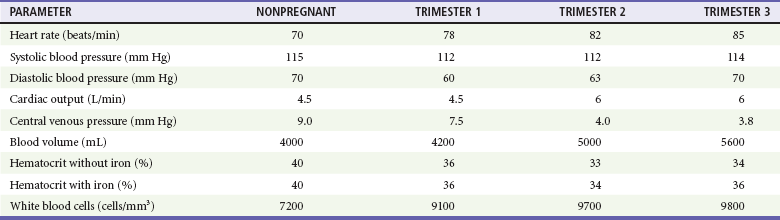
Chapter 37 Trauma occurs in 6 to 7% of all pregnancies. It is the leading nonobstetric cause of maternal death, accounting for close to 50% of fatalities in pregnant women.1 The most common causes of injury in pregnancy, in order of frequency, that result in emergency department (ED) visits are motor vehicle collisions (MVCs), interpersonal violence, and falls.2–5 Patients with penetrating injuries are seen more frequently in EDs in inner city medical centers.6 Of note, 8% of women aged 15 to 40 admitted to a trauma center do not yet know they are pregnant.7 Commonly used thresholds of fetal viability are an estimated gestational age of 24 to 26 weeks or an estimated fetal weight of 500 g. Only viable fetuses are monitored, because no obstetric intervention will alter the outcome with a previable fetus.8 Counseling on proper seatbelt and alcohol use and screening for interpersonal violence may help to reduce the morbidity and mortality rates for pregnant patients. Although the essential principles of trauma management remain unchanged in the pregnant patient, a number of special points need to be considered. Pregnancy causes alterations in physiology and anatomy that affect multiple organ systems. Although there are two lives involved, maternal life takes priority. The normal cardiovascular changes of pregnancy can alter the presentation of shock and vascular events (Table 37-1). Table 37-1 Hemodynamic Changes of Pregnancy (Mean Values) Data from de Swiet M: The cardiovascular system. In Hytten F, Chamberlain G, eds: Clinical Physiology in Obstetrics. Oxford, UK: Blackwell Scientific Publications, 1980, pp 3-42; Colditz RB, Josey WE: Central venous pressure in supine position during normal pregnancy. Comparative determinations during first, second and third trimesters. Obstet Gynecol 36:769, 1970; Letsky E: The haematological system. In Hytten RF, Chamberlin G, eds: Clinical Physiology in Obstetrics. Oxford, UK: Blackwell Scientific Publications, 1980, pp 43-78; and Cruikshank DP: Anatomic and physiologic alterations of pregnancy that modify the response to trauma. In Buchsbaum HJ, ed: Trauma in Pregnancy. Philadelphia: WB Saunders, 1979, pp 21-39. Some Alterations Mimic Shock.: Blood pressure declines in the first trimester, levels out in the second trimester, and then returns to nonpregnant levels during the third trimester. The decline in systole is small, 2 to 4 mm Hg, whereas diastole falls 5 to 15 mm Hg. Heart rate increases in pregnancy but does not rise by more than 10 to 15 beats per minute above baseline (mean of approximately 90 beats/min). A major contributor to maternal hypotension is the supine hypotensive syndrome. After 20 weeks’ gestation, the uterus has risen to the level of the inferior vena cava, resulting in compression when the mother is supine. Such caval obstruction diminishes cardiac preload, which can decrease cardiac output by as much as 28%, resulting in reduced systolic blood pressure by 30 mm Hg. In late pregnancy, it is common for the inferior vena cava to become completely occluded when the pregnant patient is supine. Attempts at resuscitation will be improved if compression is relieved. In determining whether observed hypotension is related to positioning, the pregnant woman’s pelvis can be tilted so that the uterus is displaced from the inferior vena cava, (i.e, tilt the patient onto her left side unless otherwise prevented because of other injuries). The uterus can also be manually pushed to the left by with two hands, pushing the uterus toward the patient’s head. One early study found that tilting limited to only about 15 degrees may only partially resolve vena caval obstruction9; thus, maintaining a position between 15 and 30 degrees is optimal. Elevating the patient’s legs, where blood may pool owing to increased capacitance, will improve venous return. Alterations That May Mask Hypovolemic Shock.: Blood volume gradually increases during pregnancy, starting at 6 to 8 weeks’ gestation, to as much as 45% above normal, peaking at 32 to 34 weeks’ gestation. Blood volumes become increasingly larger for multigravidas, twins, triplets, and quadruplets. With this increased circulatory reserve, clinical signs of maternal hypotension from acute traumatic bleeding may be delayed. Some Alterations Can Exacerbate Traumatic Bleeding.: By the beginning of the second trimester and throughout the remaining pregnancy, cardiac output is increased 40%, to 6 L/min. Blood flow to the uterus increases from 60 mL/min before pregnancy to 600 mL/min at term. This hyperdynamic state is needed to maintain adequate oxygen delivery to the fetus. Because the mother’s total circulating blood volume flows through the uterus every 8 to 11 minutes at term, this organ can be a major source of blood loss when injured. By the third trimester, there is also marked venous congestion in the pelvis and lower extremities, increasing the potential for hemorrhage from both bony and soft tissue pelvic injuries. The pregnant woman at term has a significantly reduced oxygen reserve. This effect comes from a reduction in functional residual capacity caused by diaphragm elevation and an increase in oxygen consumption related to the growing fetus, uterus, and placenta. In a classic study, Archer and Marx observed that mean arterial oxygen tension dropped by 29% in pregnant women at term during 60 seconds of apnea but just 11% in nonpregnant women. Labor accelerates this decline by a further 7%.10 In addition, minute ventilation increases, leading to hypocapnea. Therefore an arterial partial pressure of carbon dioxide (PaCO2) of 35 to 40 mm Hg may indicate inadequate ventilation and impending respiratory decompensation in the pregnant patient. At signs of respiratory compromise or hypoxia, endotracheal intubation should be considered, as maternal hypoxia rapidly leads to fetal hypoxia, distress, and possibly demise. There are no contraindications to rapid sequence intubation during pregnancy. Bag-valve-mask ventilation is more difficult in the pregnant patient. Fetal mortality rates range from 4 to 40% after maternal trauma, with most likely causes of fetal death occurring from placental abruption, maternal shock, and maternal death, in order of decreasing incidence.11 Risk factors significantly predictive of fetal death include ejections, motorcycle and pedestrian collisions, maternal death, maternal tachycardia, abnormal fetal heart rate, lack of restraints, and an Injury Severity Score greater than 9.8 Unbelted or improperly restrained pregnant women are twice as likely to experience excessive maternal bleeding, and fetal death is three times more likely to occur.11–13 For low- to moderate-severity crashes (constituting 95% of all MVCs), proper restraint use, with or without air bag deployment, generally leads to acceptable fetal outcomes. For high-severity crashes, even proper restraint does not improve fetal outcome.14 Pregnant crash-test-dummy trials show that improper placement of the lap belt over the pregnant abdomen causes a threefold to fourfold increase in force transmission through the uterus. The lowest force transmission readings through the uterus occur when a three-point seat belt is used properly. For correct position, the lap belt should be placed under the gravid abdomen, snugly over the thighs, with the shoulder harness off to the side of the uterus, between the breasts and over the midline of the clavicle.15 Women who receive information on seat belt use during pregnancy from a health care worker are statistically more likely to use seat belts and to use them properly than uninformed controls.15 Although it has been previously documented that intimate partner violence against women affects one in four U.S. women, and numerous health consequences have been associated with being a victim of such violence, a 2006 study by Silverman and colleagues conclusively demonstrated that physical abuse from husbands or boyfriends compromises a woman’s health during pregnancy, as well as her likelihood of carrying a child to term and the health of her newborn.16 Women experiencing abuse in the year before or during a pregnancy were 40 to 60% more likely than nonabused women to report high blood pressure, vaginal bleeding, severe nausea, kidney or urinary tract infections, and hospitalization during that pregnancy. Abused pregnant women were 37% more likely to deliver preterm, and children of abused pregnant women were 17% more likely to be born underweight. These conditions pose grave health risks to newborns, and children born to abused mothers were over 30% more likely than other children to require intensive care at birth.16–18 Physicians detect only a minority of cases, which supports the need for routine screening for interpersonal violence in pregnant patients. Falls become more prevalent after the 20th week of pregnancy.2 Protuberance of the abdomen, loosening of pelvic ligaments, strain on the lower back, and fatigability contribute to this problem. In a given pregnancy, about 2% of pregnant women sustain repeated direct blows to the abdomen because of falling more than once. Although repeated falls often trigger premature contractions, they seldom result in immediate labor and delivery. The gravid uterus alters injury patterns to the mother. There is an increased probability of harm (approaching 100%) to the bowel, liver, or spleen if the entrance of the penetrating object is in the upper abdomen. When the entry site is anterior and below the uterine fundus, visceral injuries are less likely. Although the enlarging uterus can act as a shield against intra-abdominal injuries in the mother, it makes the fetus more susceptible to injury. A high fetal death rate from penetrating trauma to the uterus has been reported, but a lower fetal death rate for maternal injuries above the uterus.19 Pregnancy does not alter rates of maternal mortality caused by trauma. However, trauma is associated with a high risk of fetal loss. When the mother sustains a severe level of injury, poor fetal outcome is predicted by maternal hypotension and acidosis (hypoxia, lowered pH, lowered bicarbonate) and a fetal heart rate of less than 110 beats/min.5,6,20 When the mother sustains life-threatening injuries, there is a 40% chance of fetal demise, compared with a less than 2% chance in cases of non–life-threatening maternal injuries. Maternal age and gestational age may also be important factors in determining fetal outcome.21 Maternal disseminated intravascular coagulation (DIC), which may be caused by placental products entering the maternal circulation, is a significant predictor of fetal mortality.11 For women with less severe trauma, fetal outcome is not predicted by maternal vital signs, abdominal tenderness, blood tests, or ultrasonography (US) results. Only cardiotocographic monitoring for a minimum of 4 hours is useful in predicting fetal outcome.3 Fatal in utero fetal injuries from blunt trauma usually involve intracranial hemorrhage and skull fractures. Such head injury is often secondary to fractured maternal pelvic bones striking the fetal skull as a result of vertex lie. Pelvic and acetabular fractures during pregnancy are associated with a high maternal (9%) and a higher fetal (38%) mortality rate.22 With penetrating trauma, gunshot wounds to the uterus are associated with a high incidence of fetal injury and fetal mortality. Stab wounds to the uterus produce substantial morbidity and mortality to the fetus.11 In blunt trauma, 50 to 70% of all fetal losses result from placental abruption.19,23 It is the leading cause of fetal death after blunt trauma. Placental separation results when the inelastic placenta shears away from the elastic uterus during sudden deformation of the uterus. Because deceleration forces can be as damaging to the placenta as direct uterine trauma, abruption can occur with little or no external sign of injury to the abdominal wall. Because all gas exchange between the mother and fetus occurs across the placenta, abruption inhibits the flow of oxygen to the fetus and causes in utero carbon dioxide (CO2) accumulation. Such hypoxia and acidosis can lead to fetal distress. Sustained uterine contractions induced by intrauterine hemorrhage also inhibit uterine blood flow, further contributing to fetal hypoxia.24 The diagnosis of abruption is a clinical one, and US and the Kleihauer-Betke test are of limited value.24 Classic clinical findings of abruption may include vaginal bleeding, abdominal cramps, uterine tenderness, maternal hypovolemia (up to 2 L of blood can accumulate in the gravid uterus), or a change in the fetal heart rate. However, many cases of placental abruption after trauma show no evidence of vaginal bleeding.11 The most sensitive indicator of placental abruption is fetal distress. Therefore prompt fetal monitoring is a very important assessment technique in trauma during pregnancy. There is also a close linkage of abruption to uterine activity, with increased frequency of contractions associated with abruption. US is less than 50% accurate as a first-line test in detecting placental abruption.19,25 If the abruption bleeds externally, not enough blood collects to be seen sonographically. Even with significant intrauterine blood accumulation, accurate US diagnosis may be difficult because of placental position (i.e., posterior) and confounding uterine or placental structural conditions. Placental abruption is associated with an overall 8.9-fold increased risk of stillbirth (>20 weeks) and a 3.9-fold increased risk of preterm delivery (before 37 weeks). The extent of placental separation affects stillbirth rates. At 50% separation, there is a fourfold increased risk of stillbirth, and a more profound 31.5-fold increased risk of stillbirth is present at 75% separation. The risk of preterm delivery is substantially increased with even mild abruptions; a 25% separation carries a 5.5-fold increased risk of preterm delivery.24,25 When mother and fetus are stable, expectant management can be tried for partial placental abruptions of less than 25%. This usually applies to fetuses of less than 32 weeks’ gestation in which the likelihood of morbidity and mortality associated with prematurity makes delivery management risky. Expectant care in stable patients may allow further fetal maturation and improved outcome. If expectant management is pursued, close maternal and fetal monitoring is needed to ensure the well-being of both patients. The ability to perform an immediate cesarean section is necessary because there may be little time between the appearance of fetal distress from further placental separation and the occurrence of fetal death. After 32 weeks’ gestation the risk of further placental separation outweighs the benefits of further fetal maturation, so intervention may be indicated.11,25 Women with placental abruption are more likely to have coagulopathies than those without abruption. The injured placenta can release thromboplastin into the maternal circulation, resulting in DIC, whereas the damaged uterus can disperse plasminogen activator and trigger fibrinolysis. The precipitation of DIC is directly related to the degree of placental separation. Severe clotting disorders rarely occur unless separation of the placenta is significant enough to result in fetal demise.24,25
Trauma in Pregnancy
Perspective
Principles of Disease—Changes of Pregnancy
Cardiovascular
Pulmonary
Clinical Features of Trauma in Pregnancy
Interpersonal Violence
Falls
Penetrating Trauma
Fetal Injury
Placental Injury
![]()
Stay updated, free articles. Join our Telegram channel





Full access? Get Clinical Tree


