ANESTHESIA FOR KIDNEY TRANSPLANTATION
Indications
• Polycystic kidney disease
• Diabetes mellitus–related kidney failure
• Hypertensive kidney disease
• Glomerular disease
• Tubulointerstitial disease
• Other familial or congenital diseases
Preoperative Evaluation
• Check electrolytes the morning of surgery (delay surgery if K+ >6.0 mEq/L)
• Should have dialysis within 24 hrs of surgery
• Typical comorbidities
CAD = major cause of death in ESRD pts before & after transplant
Electrolyte abnl, HTN, DM, delayed gastric emptying, acidosis, anemia
CHF (from vol overload & compensatory concentric cardiomyopathy)
Coagulopathies (qualitative platelet defect in uremic pts), pericarditis
Intraoperative Management
• Standard monitors (avoid placing BP cuff on fistula arm)
• Consider A-line (if indicated by comorbidities)
• Consider central line—CVP monitoring, ability to give thymoglobulin
May be difficult to place (prior dialysis lines)
Induction & Maintenance
• Usually GA (RSI if gastroparesis suspected—i.e., long-standing diabetes)
• Spinal & epidural not typically implemented (platelet dysfx in uremic pts)
• Avoid enflurane & sevoflurane (inorganic fluoride byproduct may accumulate)
• Paralytics
• Consider avoiding succinylcholine (may elev. K+ 0.5 mEq upon induction)
• Vecuronium & pancuronium may have prolonged effects
• Atracurium & cisatracurium not affected by ESRD (Hoffman degradation and nonenzymatic ester hydrolysis)
• Narcotics
• Morphine, meperidine, oxycodone metabolites can accumulate & prolong duration
• Fentanyl, sufentanil, alfentanil, remifentanil may be safer alternatives
Surgical Procedure
• 8–10 cm arced incision from pubic symphysis to anterior superior iliac spine
• Graft anastamoses usually made to external iliac vein & artery
External iliac artery & vein clamped for anastamoses
• Graft warm ischemia time is usually about 15–30 min
• Bladder filled via Foley catheter (to facilitate ureteral anastomosis to bladder)
• Native kidney only removed if pt has intractable HTN or chronic infection
Specific Intraoperative Considerations
• Hypotension may ensue with unclamping of iliac vessels & graft reperfusion
Avoid α-adrenergic agents that cause graft vessel vasoconstriction (phenylephrine)
Low-dose dopamine (3–5 mcg/kg/min) may be a better option
• Heparin may be requested before clamping of iliac vessels
• ↑ preload (CVP of 12–15 & MAP >60) before unclamping/reperfusion by administering 0.9 NS (3–5 L may be needed) or colloid
• Mannitol may act as free radical scavenger & help diurese kidney after reperfusion (furosemide also used); goal urine output >0.5 mL/kg/hr
• Ca-blocker admin before vessel anastomosis may prevent reperfusion injury
• Consider bicarbonate infusion for significant metabolic acidosis (pH <7.2)
Immunosuppressive Agents
• Typical combination: Corticosteroids, cyclosporine (or tacrolimus), & azathioprine (or mycophenolate mofetil)
• Can delay cyclosporine & tacrolimus a few days & use antithymocyte globulin instead
Postoperative Management
• Pt usually extubated
• Goal urine output >0.5 mL/kg/hr
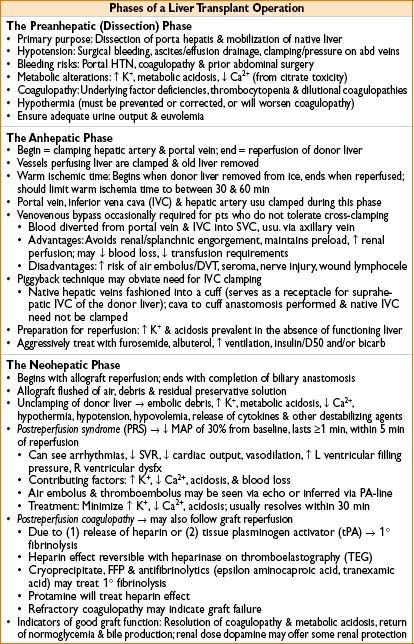
ANESTHESIA FOR LIVER TRANSPLANTATION (ALSO SEE CHAPTER 18, ANESTHESIA FOR GENERAL SURGERY)
General
• 1-yr survival following transplant 80–90%; 5-yr survival: 60–80%
• Organ allocation: Based on MELD (model of end-stage liver dz) or PELD (pediatric) score
• Increasing use of Non-Heart Beating Donation (NHBD), although still a small minority; also more use of extended donor criteria organs (age >70, DM, HTN, atherosclerotic heart dz) requiring more rapid reperfusion
Preoperative Evaluation
• Underlying diagnoses of recipients
Hepatitis C (28%), EtOH (18%), cryptogenic cirrhosis (11%), primary biliary cirrhosis (9%), primary sclerosing cholangitis (8%), fulminant (6%), autoimmune (6%), hep B (4%), EtOH + hep C (4%), HCC (2%), metabolic (4%), other (4%)
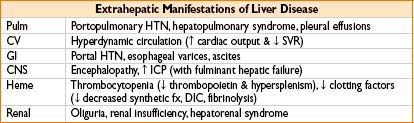
• Extrahepatic manifestations of liver disease: correctible problems include coagulopathy (platelet & FFP admin) pleural effusions (thoracentesis)
Intraoperative Management
• Venous access
• Large-bore peripheral access (RICC line or 8.5 Fr peripheral IV)
• 8.5 or 9 Fr central venous catheter
• May need additional access if PA catheter is in lumen of 8.5 or 9 Fr central catheter
• Standard monitors; A-line preinduction; CVP; consider PA catheter & TEE
• Equipment
• Stat lab must be close by & available
• Rapid infuser systems (Level I, Belmont, etc.) set up & available
• Blood products available (usually 10 U FFP, 10 U PRBCs, & platelets)
• Venovenous bypass machine (with perfusionist) available
• Cell saver
Induction and Maintenance
• Usually RSI (for “full stomach” precautions) or awake intubation
• Pts often coagulopathic (use care when placing lines, ETT, NG tube)
• Inhalational agents, narcotics, & muscle relaxants during maintenance
• Avoid ketamine—can ↑ seizure activity
• Moderate coagulopathy is permissible, provided there is no clinical bleeding
• Aggressive use of blood products may worsen outcome
• Conservative fluid management in selected patients
• Maintain normothermia
Postoperative Management
• Peripheral nerve injuries commonly due to positioning
• Following skin closure, patient brought to ICU (usually intubated)
ANESTHESIA FOR LUNG TRANSPLANTATION
Indications
• COPD, idiopathic pulmonary fibrosis, cystic fibrosis (CF), α1-antitrypsin deficiency, PPH (primary pulmonary HTN)
• Terminally ill patients with end-stage lung disease
• Less frequently: Sarcoidosis, retransplantation, Eisenmenger’s syndrome
Indications for Heart–Lung Transplantation (HLT)
• Pts with lung transplant indication & significant left ventricular dz
• Most commonly PPH, CF, & Eisenmenger’s syndrome
Single-Lung Transplantation (SLT) vs. Bilateral Sequential Lung Transplantation (BSLT)
• BSLT = 1 lung transplanted (start with native lung with worse function) followed by a repeat procedure on contralateral side
Preoperative Evaluation
• Lab values: ABO compatibility of donor & recipient
• Radiography, echocardiography (RV failure)
• Functional data (including PFTs) & left heart cath (exclude CAD and intracardiac shunt)
• Pts may have difficulty lying flat (poor pulm function)
Intraoperative Considerations
• Standard monitors + A-line, central line, PA catheter; consider TEE (assess RV fx)
• Lung isolation techniques (fiberoptic scope necessary)
• 2 large-bore IVs; ± epidural catheter
• Be ready for emergent initiation of cardiopulmonary bypass
Induction and Maintenance
• Lung isolation: Double-lumen tube, univent tube, or ETT + bronchial blocker
• Avoid N2O (presence of bullous emphysematous dz, pulm HTN, intraop hypoxemia)
• Fluid management usually conservative (helps with postop management)
• Permissive hypercapnea
• Be vigilant for cardiac instability or pneumothorax on nonoperative side
Surgical Procedure for Single-Lung Transplantation
• Posterolateral thoracotomy position (need for rapid access to cannulation sites for emergent cardiopulmonary bypass may affect positioning)
• Incision usually anterior thoracotomy with partial sternotomy
• Sequence of surgical events:
1. Structures for lung to be resected are dissected free
2. Pneumonectomy completed
3. Bronchial anastomosis first, PA anastomosis, atrial/pulm vein anastomosis last
4. Pulmonary circulation flushed & ventilation begun
5. Process repeated for other side during bilateral sequential lung transplantation
Specific Anesthetic Considerations
• Lung recipients susceptible to pulm HTN & R ventricular dysfx during 1-lung ventilation
• Hypoxemia common in 1-lung ventilation; consider using:
• FiO2 of 100%
• PEEP of 10 as tolerated to dependent lung
• CPAP to nondependent lung
• Nitric oxide (NO)
• Advantages:
• ↓ pulm vascular resistance & improves oxygenation
• NO preferentially reaches ventilated areas, causing ↑ blood flow, improvements in V./Q. mismatch & improved oxygenation
• ↓ inflammatory response to surgery or trauma
• Impedes microbial growth
• Activates guanylate cyclase in platelets to attenuate platelet aggregation & adhesion
• Disadvantages:
• Methemoglobinemia, NO metabolite–related lung injury, ↓ sensitivity of exhaled N2O monitoring
• Rapid discontinuation of NO in pulm vasculature prevents systemic vasoconstriction & results in systemic hypotension
• Cardiopulmonary bypass (CPB) indications
• Adequate oxygenation cannot be maintained despite ventilatory/pharmacologic interventions & PA clamping by surgeons
• Inability to ventilate
• Development of RV dysfx
• CI <2 L/min/m2, SvO2 <60%, MAP <50–60 mm Hg, SaO2 <85–90%, pH <7
• May see hypotension with restoration of graft blood flow after anastomosis
• At end of procedure, eval of pt for tube exchange to single lumen is performed, although high PEEP requirements & oropharyngeal edema may preclude it
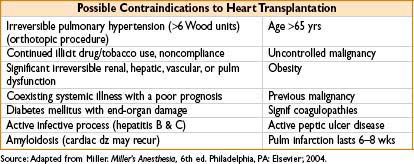
ANESTHESIA FOR HEART TRANSPLANTATION
General Information
• 1-yr survival = 87%, 2-yr survival 78% from 1997–2004
• Poor survival due to paucity of donor organs, devices (e.g., left ventricular-assist devices—LVAD) used to provide a bridge to transplant
Most Common Indications
• New York Heart Association class III/IV heart failure (despite optimal therapy)
• Heart failure survival scores high risk
• Peak VO2 <10 mL/kg/min after anaerobic threshold
• Severely symptomatic ventricular arrhythmias refractory to medical, ICD, surgical Tx
• Severely limiting ischemia unresponsive to interventional or surg revascularization
Perioperative Assessment
• Donor heart function worsens with ischemic time >6 hrs
• Pt usually not NPO (owing to short notice of graft availability)
• Pt may receive extensive levels of cardiovascular support
• Meds—warfarin, vasopressor support, ACE inhibitor, dobutamine, milrinone
• Devices—LVAD, pacemaker/AICD, IABP
• Immunosuppressive meds & antibiotics
• Ensure blood products available
Intraoperative Management
• Large-bore IV access, std monitors, preinduction A-line, CVP & PA catheter, TEE
• Induction and maintenance
• Consider high-dose narcotic rapid sequence induction
• Also etomidate (0.3 mg/kg), fentanyl 1 mcg/kg), succinylcholine (15 mg/kg)
• Neuromuscular blockade with nondepolarizing agent
• May need inotropic support upon induction
• Standard heparin dosing for pre-CPB anticoagulation
• See Chapter 16, Anesthesia for Cardiac Surgery, for detailed notes on CPB
• Separation from CPB
• Transplanted heart denervated (will not mount tachy-/bradycardic responses)
• Only direct-acting sympathomimetics work for inotropic/chronotropic effects
• Isoproterenol, epinephrine, milrinone, dobutamine
• LV function is generally adequate, however, RV dysfunction often seen
• Strategies to lower PVR
• High FiO2; avoid hypercapnia/hypothermia
• Optimize airway pressures & tidal volumes
• Use nitrates, PGE1, prostacyclin, & inhaled NO as indicated
• Use CVP/TEE to guide fluid management
• Consider use of RV assist device
Surgical Procedure
• Incision median sternotomy
• Aortic cannulation high, near the arch
• Recipient heart excised (except for L atrial tissue with pulmonary veins)
• Biatrial approach—excises both atria (mandating bicaval anastomosis)
• Classic approach—atria transected at grooves
Specific Anesthetic Considerations
• Anticipate previous cardiac surgery (redo sternotomy)
• Structures may be adhesed to sternum & ruptured upon entry
• Presence of LVAD/RVAD
• Pts with hemodynamic instability may need extracorporeal membrane oxygenation (ECMO) prior to induction
• Immunosuppressive agents need to be given including methylprednisolone 500 mg as last anastomosis is being completed
• No specific anesthetic strategies for posttransplant anesthesia delivery
• May see a delayed response to catecholamines
• Anticipate a denervated heart with absence of vagal tone
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


