Chapter 82 Transfusion Medicine
Red Blood Cells
RBCs contain hemoglobin (Hb), which binds and carries oxygen (O2) to cells, thus facilitating efficient adenosine triphosphate (ATP) production via cellular respiration. Because energy expenditure is high in critically ill patients, it would seem rational to maintain their Hb level in the normal range. Anemia is observed in 74% of critically ill children.1 RBC transfusion is the only effective way to rapidly increase the Hb level. However, the safety of RBC transfusion has been questioned in recent years. Infections transmitted by blood products were the most important concern in the 1980s. In the 1990s, nosocomial infections and multiple organ dysfunction syndrome (MODS) observed in critically ill adults who received an RBC transfusion have become a cause of concern.2 Also transfusion-related immune modulation (TRIM),3 and transfusion reactions like transfusion-related acute lung injury (TRALI) and transfusion-associated cardiac overload (TACO)4 have become significant concerns. There are few data on these adverse events in PICU. Actually, the impact of RBC transfusion on risk/benefit and the cost/benefit ratios among critically ill children is not well characterized.
Red Blood Cell Transfusion: Why and Why Not
Anemia and O2 Delivery
O2 Delivery in the Critically Ill

In this formula, the Hb level is expressed in grams per deciliter, arterial O2 saturation (SaO2) is expressed as a fraction rather than a percentage, and PaO2 is expressed in mm Hg or torr. Because global DO2 is directly linked to the Hb concentration, the most rapid and effective way of increasing DO2 (within minutes) is by increasing the Hb concentration, and this represents the most common rationale underlying RBC transfusion in critically ill patients. More modest augmentation in global DO2 can be attained by increasing cardiac output and/or SaO2. Indeed, a prospective study conducted in 2005 involving 30 North American PICUs showed that about 50% of critically ill children received at least one transfusion of packed RBC unit during their PICU stay.1

in which CmvO2 is the mixed venous O2 concentration. VO2 depends on substrate availability and on metabolic demands; it can be amplified by increasing cellular O2 extraction rate (O2ER), or by increasing DO2 if there is VO2/DO2 dependence (Figure 82-1).
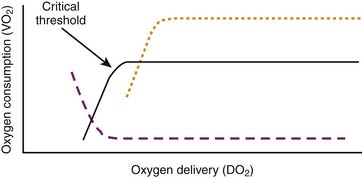
The relationship between O2 delivery and consumption is characterized by two phases: a directly linear relationship between VO2 and DO2 up to a “critical threshold” (often referred to as the critical DO2), and a flat section above this threshold (see Figure 82-1). Below the threshold, VO2 diminishes if DO2 decreases. Above this threshold, a fall in DO2 does not cause a drop in VO2 because it is compensated by mechanisms such as an increase in O2ER; these mechanisms are limited though, which explains why there is a critical threshold of DO2 under which O2ER cannot increase any further, and under which VO2 begins to fall.
Adaptive Mechanisms to Anemia
Anemia significantly decreases blood O2 carrying capacity. However, in the normal host, the amount of O2 delivered to tissues exceeds resting O2 requirements by a two- to fourfold factor.5 When the Hb concentration falls below 10 g/dL, several adaptive processes maintain VO2. These processes include (1) increased O2ER; (2) increased heart rate and stroke volume, which increase cardiac output; (3) redistribution of blood flow from nonvital organs toward the heart and brain, at the expense of O2 delivery to less vital vascular beds, such as the splanchnic vasculature; and (4) rightward shift of the oxy-Hb-dissociation curve, which decreases affinity between Hb and O2, thereby increasing the amount of O2 released to cells.
O2 Kinetics in the Critically Ill
Tissue hypoxia from low DO2 may be due to low Hb concentration (anemic hypoxia), low cardiac output (stagnant hypoxia) or low Hb saturation (hypoxic hypoxia).5 A significant number of intensivists use RBC transfusion to increase DO2 in critically ill children.6 RBC transfusion indeed increases DO2, but there is no clear evidence that RBC transfusion improves tissue VO2 in ICU patients.2 Many mechanisms may explain why VO2 does not always increase in such instances. Mitochondrial dysfunction is frequent in critically ill patients; this may prevent O2 utilization (see Chapter 74).7 Moreover, O2 delivery to tissue is impaired in ICU patients, and there is some evidence that RBC transfusion may worsen that problem.
Regulation by Red Blood Cells of DO2 to Tissue
Although RBC transfusion certainly increases systemic DO2 in the central circulation, it does not mean that local O2 delivery to tissues is improved. There is indeed evidence that RBC transfusion may disturb local DO2. For example, Kiraly et al.8 showed that tissue SO2 (StO2) in critically ill patients who received a transfusion of RBC units stored more than three weeks declined from about 89% to 81%, whereas this did not happen in controls. However, data on local DO2 are inconsistent, their clinical significance remains to be determined, and the mechanisms are not well characterized; blood viscosity, microcirculatory flow, local DO2, and cellular respiration may be involved.
Activation of white blood cells (WBC) in packed RBC units and cytokine generation in the supernatant of transfused RBC units may also have a microcirculatory effect: some cytokines can mediate vasoconstriction or thrombosis of small vessels and cause local ischemia.9 However, most packed RBC units are now prestorage leukocyte-reduced, which significantly decreases cytokine levels in the supernatant.10 The clinical impact of cytokines in the supernatant of prestorage leukocyte-reduced packed RBC units remains to be determined.
There is evidence that RBC transfusion can cause vasoconstriction of small blood vessels via a mechanism involving an interaction between the Hb in RBC and the nitric oxide released by small vessels. With local tissue hypoxia, Hb in the microvasculature releases nitric oxide and triggers local vasodilatation; conversely, if there is sufficient O2 in the microvasculature, Hb binds nitric oxide resulting in vasoconstriction. This regulatory mechanism is almost immediately lost once RBCs are stored: it has been shown that in vitro exposure of blood vessels to RBC units stored 3 hours or more causes vasoconstriction.11 However, the level of nitric oxide increases rapidly after transfusion.12 Although the clinical significance of these observations is not clear yet, these findings nonetheless suggest that local DO2 can be disturbed by RBC transfusion.
Packed RBC units undergo several changes during storage, which are generally referred to as “storage lesion.”13 For example, the level of 2,3-diphospho- glycerate (2,3-DPG) in stored RBC decreases over time and can induce a leftward shift in the oxy-Hb dissociation curve, which impedes O2 release to tissues even if DO2 is increased. In addition, RBC deformability decreases after 2 or 3 weeks of storage, which may alter their capacity to pass through the capillary bed. Furthermore, hemolysis in older packed RBC units releases substantial amounts of free Hb ranging from 0.5 mg/dL in a 1-day-old RBC unit to 250 mg/dL in a 25 day-old unit14; free intravascular Hb has the ability to bind nitric oxide and therefore likely mediates vasoconstriction.15
Transfusion of Red Blood Cells: Indications (When)
Blood is clearly indicated for the treatment of hemorrhagic shock.2 In such instances, the decision to prescribe RBC transfusions should be based on the physiologic state, the estimated amount of blood loss, and risk of ongoing hemorrhage, not on the Hb concentration.
RBC transfusion is more questionable if the hemorrhage is not clinically significant or if there is no hemorrhage. Pediatric intensivists have stated in two surveys that their decision to prescribe a RBC transfusion would be based on reasons such as a low DO2 or VO2, cardiovascular insufficiency, respiratory failure, or use of certain specific technologies such as extracorporeal membrane oxygenation (ECMO), hemodialysis, hemofiltration, plasmapheresis, or exchange transfusion; nonetheless, the most frequent reason to transfuse RBCs was reported to be a low Hb concentration.1,6 The Hb level that should prompt a pediatric intensivist to prescribe RBC transfusion remains a matter of debate, but there is some evidence in the medical literature that can guide practitioners.
Evidence-Based Medicine: Clinical Studies
Four case series are applicable to critically ill children: two in children with septic shock,16,17 another in postoperative cardiac surgery patients,18 and the last in children with cyanotic heart disease undergoing elective cardiac catheterization.19 These studies assessed hemodynamic parameters before and after a 0 to 20 mL/kg packed RBC transfusion; all reported a significantly increased Hb level as well as a greater DO2 after transfusion, but only one study reported an increase in VO2.16 These findings support the hypothesis that RBC transfusion increases systemic DO2, but does not necessarily increase VO2.
There is evidence that severe anemia increases mortality and morbidity among severely ill children. In two studies involving patients who refused blood products for religious reasons, the risk of mortality increased significantly with a postoperative Hb level less than 4 g/dL in healthy adults20 and less than 10 g/dL in adults with heart disease.21 There are three prospective descriptive studies addressing this issue in pediatrics. Lackritz et al.22 followed 2433 African anemic children younger than 12 years among whom 20% received a RBC transfusion. They reported that RBC transfusion was beneficial if the Hb level was below 4.7 g/dL and if the patient presented some respiratory distress. Lackritz et al.23 subsequently published another prospective study examining 1223 consecutively hospitalized children in Kenya. Local guidelines suggested that an RBC transfusion should be given to all children with an Hb level less than 5 g/dL. The Hb level was less than 5 g/dL in 303 cases; 116 (38%) did not receive a transfusion, mostly because packed RBC units were not available. Each child with severe anemia was paired with the next child hospitalized with an Hb greater than 5 g/dL. The death rates were: 19.5% in 303 patients with Hb greater than 5 g/dL who were not transfused, 21.4% in 187 patients with Hb less than 5 g/dL who were transfused, and 41.4%% in 116 patients with Hb less than 5 g/dL who were not transfused. English et al.24 completed a prospective cohort study of 1269 children with malaria hospitalized in Kenya; they reported that RBC transfusion decreased mortality if anemia was severe (Hb level <4 g/dL), or if a Hb level less than 5 g/dL was associated with dyspnea. These three studies suggest that the risk of mortality increases significantly in severely ill children requiring hospitalization if their Hb concentration is lower than 5 g/dL particularly if respiratory symptoms are present.
Two randomized clinical trials evaluated RBC transfusion strategies in children. The first trial was performed in Africa in 106 children with malaria crisis (hematocrit: 12% to 17%); RBC transfusion did not improve mortality rate (1/53 vs. 2/53) in patients without respiratory or cardiovascular compromise.25 In the TRIPICU study, a large multicenter international randomized clinical trial involving 637 stable critically ill children with Hb level lower than 9.5 g/dL, 320 patients were allocated to a RBC transfusion threshold of 7 g/dL of Hb (restrictive group) and 317 to a threshold of 9.5 g/dL (liberal group). A statistically significant noninferiority was found: 38 and 39 patients respectively developed new or progressive MODS, and there were 14 deaths in both strategy groups within 28 days postrandomization. The conclusion of this study was that a restrictive strategy is as safe as a liberal strategy in stable critically ill children. Moreover, given that 174 patients (54%) in the restrictive group received no RBC transfusion compared to 7 (2%) in the liberal group (P <.0001) and that patients in the restrictive group received 54% fewer RBC transfusions, the findings supported adopting a restrictive transfusion strategy for stabilized critically ill children.26 Subgroup analyses were subsequently undertaken in patients with sepsis27 and those having undergone noncardiac surgery28: both showed trends very similar to those reported in the original TRIPICU study.
Red Blood Cell Transfusion: Current Recommendations
Guidelines from many organizations emphasize that the decision to administer RBC should not be determined solely by an Hb value, but should be based on sound clinical judgment.2,29,30 RBC transfusion in PICU is indeed associated not only with a low Hb level, but also with admission for cardiac disease (odds ratio [OR], 8.07; 95% confidence interval [CI], 5.14 to 14.65), higher severity of illness (PRISM score >10: OR, 4.83; CI, 2.33 to 10.04), and presence of MODS (OR, 2.06; CI, 1.18 to 3.57).31 In a survey,6 pediatric intensivists declared that they might consider prescribing a RBC transfusion based on the following markers: Hb concentration, low SaO2, low PaO2, low cardiac output (poor DO2), high blood lactate level, low ScvO2 or SmvO2, poor VO2, high severity of illness, active bleeding, and emergency surgery. However, how these determinants of RBC transfusion interacted with each other was unclear.
Many physicians advocate “goal-directed transfusion therapy.”32,33 Although it is theoretically rational to base the decision to transfuse RBCs on physiologic need, it is still a matter of debate what parameters best determine that need. It has been suggested that a RBC transfusion is indicated for patients with symptomatic anemia, but most critically ill children are unable to report these symptoms. Some have suggested it would be better to use global markers of oxygenation deficit, such as systemic VO2, VO2/DO2 dependence, blood lactate level, ScvO2, SmvO2, or O2ER.34 Others propose the use of measurements that reflect local, regional, or tissue oxygenation deficit, such as brain tissue O2 pressure (PbtO2),35 gastric tonometry36 StO2 measured by near-infrared spectroscopy8 or digital O2 extraction rate measured by noninvasive devices. Actually, it is presently not known what markers are best suited for this purpose and what cutoff values should be used to determine the need for RBC transfusion in critically ill children. The concept of goal-directed transfusion therapy is laudable, but is presently vaguely defined, and not supported by hard data. Recommendations specific to goal-directed transfusion therapy remain undetermined at the present time.32
In practice, a low Hb concentration remains the most frequent and the primary justification for pediatric intensivists to prescribe a RBC transfusion.1 Therefore it makes sense that the Hb concentration be the first parameter assessed when a RBC transfusion is considered. Given the available evidence, RBC transfusion is recommended for all critically ill children who present with a Hb concentration below 5 g/dL. In stable patients, including septic patients,27 patients having undergone noncardiac surgery,28 and severely burned children,37 it is suggested by experts to consider a RBC transfusion if the Hb concentration is lower than 7 g/dL, but a transfusion is not recommended if the Hb concentration is above this level.2 These thresholds are not so far from current practice: Goodman et al.38 have reported that all critically ill children with a Hb ≤5.3 g/dL and that 93% of those with a Hb of 6.4 g/dL or less received at least one RBC transfusion. However, determinants other than the Hb concentration must be considered including age, severity of illness or evidence of organ dysfunction or O2 dependency, such as a high blood lactate level or low ScvO2. For example, it would seem appropriate to consider a higher threshold and a more aggressive RBC transfusion strategy in unstable patients, but the optimal and safe lower limit of the transfusion threshold has not been established for such patients. Moreover, any recommendations made must also factor in specific considerations for disorders such as sickle cell disease, hemolytic uremic syndrome, and some cardiac diseases.
Many experts in the field of pediatric cardiology and cardiac surgery believe that the optimal Hb concentration for patients in the postoperative phase of cardiac surgery should be significantly higher, and advocate levels as high as 14 to 18 g/dL in cases of uncorrected cyanotic congenital cardiopathy.39,40 Few clinical studies have addressed RBC transfusion in cyanotic heart disease. Experience with bloodless cardiac surgery for congenital heart disease in children whose families refuse transfusion for religious reasons seems to suggest that a lower Hb level may be well tolerated. This is supported by a randomized clinical trial involving 59 children with bidirectional Glenn or Fontan procedures. In this trial, patients were randomized either to a restrictive or liberal transfusion strategy (respective Hb concentration thresholds of 9 or 12 g/dL). The mean postoperative Hb was 11.1 ± 13 and 13.9 ± 0.5 g/dL, and the mean number of RBC transfusions was 0.47 ± 0.6 and 2.03 ± 1.2 per patient in the restrictive and liberal groups. No difference was found with respect to outcomes like peak blood lactate level (3.0 ± 1.5 vs. 3.1 ± 1.3 mmol/L), ventilator or pressor duration, ICU or hospital length of stay, or survival. More data are required before implementing a restrictive transfusion strategy in patients with cyanotic heart disease.41 Beekman’s 1985 statement that “The optimal Hb concentration for children with cyanotic heart disease has yet to be determined” remains true today.19
On the other hand, there is some evidence that a 7 g/dL threshold may be safe in the postoperative care of noncyanotic congenital heart disease in stabilized patients older than 28 days.42 Willems et al.43 analyzed a subgroup of 125 postoperative cardiac patients enrolled in the TRIPICU study after a cardiac surgery. No significant difference was found between the restrictive and liberal groups in new or progressive MODS (12.7% vs. 6.5%; P = .36), PICU length of stay (7.0 ± 5.0 vs. 7.4 ± 6.4 days) or 28-day mortality (two vs. two deaths). The British Society of Haematology30 supports the acceptance of a postoperative hemoglobin level of 7 g/dL in children when there is good postoperative cardiac function unless there is a cyanotic heart lesion persisting. The Society of Thoracic Surgeons makes a similar recommendation for all cardiac surgery patients.44 Data reported by Willems et al.43 support these recommendations.
There is a debate on the usefulness of blood transfusion as a preventive measure. Some evidence suggests that this may be appropriate in critically ill children who have certain forms of congenital anemia (for example, sickle cell disease,45 and in patients who require ECMO (a Hb threshold of 13 to 15 g/dL is suggested46) or surgery.47 However, there are few hard data to support such recommendations in the latter two groups.
Prevention of Red Blood Cell Transfusion
“Bloodless medicine” is a popular concept in many American hospitals; it refers to all the strategies that can be used to provide medical care without allogeneic RBC transfusion, including blood conservation.48 There are indeed many strategies that can prevent and/or significantly decrease the need for RBC transfusions and exposure to a transfusion. Adopting a restrictive RBC transfusion strategy in stable critically ill children is one of them; other possible means range from raising the Hb concentration before an elective surgery to using blood products only when necessary, limiting blood losses and administering the patient’s own blood.
Bloodless medicine begins before surgery. Among the possible strategies in the preoperative period, the use of erythropoietin and iron supplementation to optimize the preoperative Hb level, collection of autologous donations to prevent some allogeneic transfusion,49 avoidance of any medication that increases the risk of bleeding, including herbal medicine (e.g., garlic, ginseng, ginger33), and optimal control of any existing coagulation disorders just prior to surgery should be considered.
During surgery, maximal attention should be given to limiting blood loss50 and ensuring good hemostasis and rapid control of all bleeding. In some instances, desmopressin,51 fibrin sealants, or antifibrinolytic agents such as aprotinin or tranexamic acid48 may be used to stop a hemorrhage. Recombinant activated factor VII (rFVIIa) is also advocated by some practitioners, but it is associated with a significant risk of thrombosis; the cost/benefit ratio of rFVIIa in children is not well evaluated and its use should be limited to situations with uncontrolled bleeding that is life-threatening.52 The safety and cost-effectiveness of intraoperative blood conservation strategies such as normovolemic hemodilution,53 autologous blood cell salvage modalities,54 intraoperative autotransfusion, and deliberate hypotension50 remain to be determined in children.
Postoperative and ICU management of anemia and bleeding is also important. A restrictive transfusion strategy is in line with the concept of “permissive anemia” supported by the British Committee for Standards in Haematology Transfusion Task Force.30 A prospective study reported that 73% of blood loss in PICU is attributable to blood draws.1 The number and the frequency of blood tests must be limited, and the amount of blood collected reduced. Many devices can help to minimize blood loss, including the use of loop sampling, pediatric blood collection tubes, microanalysis techniques requiring small volumes of blood, and in-line measurement of parameters such as blood gases and Hb concentration.55–57 The erythropoietin response to anemia is blunted58 and poorer than expected in critically ill patients.59 In spite of this, there are data suggesting that erythropoietin can prevent anemia in critically ill adults,60 in low-birth-weight preterm infants61–63 and in the postoperative care of neonates.64 In critically ill children, there are no data to support the use of erythropoietin as a preventive measure because most RBC transfusions are administered within 2 or 3 days after PICU admission,1,65 a period of time too short to allow for a response to erythropoietin that generally requires several days.66 The standard use of erythropoietin is presently not recommended in PICU.65,67 In addition, iron supplementation is not indicated because most critically ill patients are not iron depleted.59
An RBC transfusion should be administered only if the anticipated benefit outweighs the potential risk. A threshold Hb concentration of 7 g/dL is adequate in most stable critically ill children.68 The optimal Hb concentration or transfusion threshold above which the benefits outweigh the risks and costs remains to be determined in unstable patients and in patients with congenital heart disease.
Types of Packed Red Blood Cell Units
Standard Packed RBC Units
Storage of RBC units is made possible by refrigeration at about 4° C and by storage in preservative anticoagulant solutions that contains dextrose, sodium citrate, citric acid, and sodium diphosphate. Erythrocytes use dextrose and phosphate to generate ATP, which is essential for their survival. Citrate blocks coagulate by chelating calcium; it is also transformed into bicarbonate, which stabilizes the stored RBC unit pH above 6.4. Citrate-phosphate-dextrose (CPD) solution can be stored up to 28 days. Citrate-phosphate-dextrose-adenine (CPDA-1) contains more dextrose (2 g vs. 1.6 g/63 mL) and more adenine (17.3 mg/63 mL) than CPD; it can be stored up to 35 days because the level of ATP remains normal after 21 days of storage and is about 50% after 35 days. Packed RBC units are prepared by removing 200 to 250 mL of plasma from one unit of whole blood by centrifugation. To support the nutrient needs of RBCs after plasma is removed, additive solutions were developed, such as AS-1 (Adsol), AS-3 (Nutricel), and AS-5 (Optisol), and saline-adenine-glucose (SAG) or SAG-mannitol (SAGM)69; these additive solutions further decrease RBC lysis and allow for storage up to 42 days.70
Other Types of Packed Red Blood Cell Units
Whole Blood
The use of whole blood has been advocated mostly for first-line therapy in hemorrhagic shock as it contains RBCs, coagulation factors, and platelets. However, it is generally not available. Additionally, refrigeration in storage solution for even several hours results in decreased levels of coagulation factors, oxygen-carrying capacity, as well as platelet function. In practice, component therapy is standard practice and it is usually easier to give one or more packed RBC units diluted with normal saline along with plasma and/or platelets. Whole blood units are also used by some for neonatal exchange transfusions, and in small children when priming for cardiac bypass procedures or continuous hemoperfusion. Whole blood is not recommended in normovolemic patients because it can cause a cardiac overload. The volume of a typical whole blood unit is about 450 mL.
Leukocyte-Reduced Packed Red Blood Cell Units
PackedRBC units contain some nonviable platelets, small amounts of coagulation factors, and WBCs that can release proinflammatory and antiinflammatory mediators during storage. Prestorage leukocyte reduction is a standard procedure for all blood components in many countries, such as Australia, Canada, and the United Kingdom; it can decrease the number of WBCs in packed RBC units from 1 × 109 to less 1 × 106 per product, and it decreases the concentration of cytokines in the supernatant, as well as some T cells that regulate immunomodulation.71 In 2005, 88% of packed RBC units given in American PICUs were leukocyte-reduced at collection.1 Transmission of intracellular viruses such as CMV and herpes is less frequent if there are fewer WBCs.
Irradiated Packed Red Blood Cell Units
Some WBCs remain in RBC and platelets units, even in prestorage leukocyte-reduced units. The objective of irradiation is to induce enough DNA damage to prevent leukocyte proliferation.72 Irradiation destroys the ability of transfused lymphocytes to divide and therefore to respond to host foreign antigens, thereby decreasing the risk of developing transfusion-associated graft versus host disease (TAGVH) in susceptible recipients. However, irradiation is not without some drawbacks. For example, it can damage the RBC membrane causing the release of significant amount of free Hb and potassium. Moreover, the shelf life of irradiated RBC units is reduced from 42 to 28 days.73
Cytomegalovirus-Negative Packed Red Blood Cell Units
A large proportion (30% to 70%) of blood donors are CMV positive. Most CMV infections are of little clinical consequence, but CMV can be fatal in patients with immunodeficiency. Fresh frozen plasma is not known to transmit CMV infection, but RBC units are. Although it would be ideal to administer only CMV-negative RBC units to CMV negative patients, the high prevalence of CMV infection among donors does not permit this.74 Nevertheless, prestorage leukocyte reduction of blood products decreases transmission of CMV to 1% to 2% (similar to the rate of infection following the transfusion of CMV negative units) compared to standard products for which transmission is 13% to 37%. Administration of a CMV positive RBC unit is generally not an issue for immunocompetent patients. Established indications for CMV-negative units include CMV-negative recipients of organ or bone marrow transplants from CMV-negative donors, CMV-negative bone marrow transplant recipients, and intrauterine transfusions. Less well-established indications include CMV-negative patients who are potential candidates for autologous or allogeneic bone marrow transplant, CMV-negative patients undergoing splenectomy, potential seronegative donors for bone marrow transplant and CMV-negative patients with HIV.
Directed Packed Red Blood Cell Units
Directed blood is donated by family members or friends. Parents frequently believe that giving their own blood decreases the risks of transfusion, which, in practice, is not the case. A small increase of transfusion-transmitted infectious diseases has been reported.46 Moreover, the risk of contracting a TAGVH is increased even in immunocompetent patients. In spite of this, directed blood donation remains popular; good clinical studies are warranted to better estimate the risk/benefit ratio of this practice. All directed RBC units must be irradiated pretransfusion.
Autologous Packed Red Blood Cell Units
Older healthy children can give their own blood a few weeks before elective surgery. It is frequently believed that autologous RBC units are free of risk, but this is untrue. These units are usually quite old by the time transfusion is required, which raises significant concerns with respect to RBC unit length of storage.75 Moreover, autologous RBC units are not leukocyte-reduced, at least in Canada. The risk/benefit ratio of autologous RBC units remains to be determined.
RBC substitutes and other alternatives to RBC transfusion
Hemoglobin-based oxygen carrier solutions (semisynthetic or synthetic preparations of Hb) and perfluorocarbon derivatives can carry O2.76,77 Both were developed as alternatives to RBCs, but there are serious concerns about their safety and usefulness. None can be recommended presently.
Transfusion of Packed Red Blood Cells: How
Erythrocyte transfusion is the best way to rapidly increase the Hb concentration. The practitioner must address a few questions after a decision is made to prescribe a RBC transfusion: what type of RBC unit (see the previous section), what blood type, how much (volume), how the unit is infused and what monitoring must be performed.
Blood Types
Table 82-1 describes the compatibility of different blood products. A completed cross-match is mandatory before any transfusion is given, with few exceptions. Transfusion of group O Rh negative RBC and/or group AB Rh positive plasma can be lifesaving, but this must be reserved for very severe and acute situations. It takes 15 to 20 minutes to complete ABO and Rh typing of a patient. If there are no RBC antibodies, fully compatible blood or immediate spin cross-match may be issued quickly. In the case of RBC antibodies or other anomalies, a full serologic cross-match is required, which will take more time. The risk of severe reaction to typed, but not cross-matched blood RBC units, is about 1 in 1000 if the patient has never received a transfusion; the risk is decreased by tenfold if a cross-match is done. If the patient has received at least one transfusion, the risks are respectively 1 in 100 with no cross-match and 1 in 1000 if a cross-match is done. It was recommended that similar units be used until patient recovery if a patient receives more than 20% of his blood volume with uncross-matched packed RBC units. However, this practice is a little outdated, as there is very little plasma in AS-3 and SAGM RBC units. If anti-A/B antibodies are detected on blood typing then antigen negative blood should be provided; otherwise ABO-identical units should be used when they become available. Repeat verification that the correct blood unit has been delivered to a given patient is essential because blood mismatch is the most important cause of severe transfusion reaction.
| Blood Product | Receiver | Donor |
|---|---|---|
| Packed RBC unit and whole blood | A, O | |
| B | B, O | |
| O | O | |
| AB | AB, A, B, O | |
| Rh+ | Rh+ or Rh− | |
| Rh− | Rh− | |
| Plasma or platelets | A, AB | |
| B | B, AB | |
| AB | AB | |
| Platelets | Rh+ | or Rh− |
| Rh− | Rh− or Rh+∗ |
∗ Give as an anti-D vaccine (Win Rho SDF) if the receiver is Rh− and the platelet concentration is Rh+.





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


