Type
Localization
Features
Technique
R1
Near the internal inguinal ring
First recurrence, reducible, thin patient, wall defect <2 cm
Gilbert with plug repair
R2
Above the pubic tubercle
First recurrence, reducible, thin patient, wall defect <2 cm
TOP
R3
Whole inguinal wall defect
Multirecurrence and/or irreducible and/or extended wall defect, femoral recurrence
TOP
R2: first recurrence, after plastic or prosthetic repair, medial (direct) reducible hernia with a small (<2 cm) defect above the pubic tubercle in a thin patient (possible also under local anaesthesia);
R3: large defect (inguinal eventration) or multi-recurrent hernias or nonreducible recurrent hernia.
6.2 6.2 Technique
The TOP technique can be done under local, spinal or general anaesthesia (the last of these is suggested during the learning curve) and requires a 5–8-cm-long suprapubic transverse lateral incision, 2 cm below the superior-anterior iliac spin (ASIS) (Fig. 6.1) [3, 10].
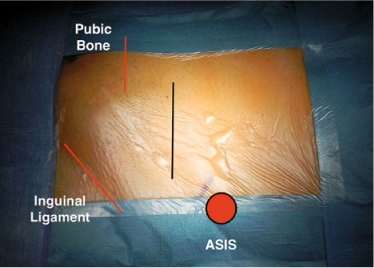
Fig. 6.1
Left inguinal region, landmarks in red (ASIS: anterior superior iliac spine) and incision line in black
After the subcutaneous space is cut, the external oblique muscle and rectus muscle aponeurosis are opened together and the fibers of the internal oblique and transversus muscle are split laterally (Fig. 6.2) [3, 10]. At this level it is sometimes possible to detect the ilioinguinal and iliohypogastric nerves: during the procedure for the treatment of chronic postoperative pain, these are tied, cut and buried in muscle (Fig. 6.2) [9].
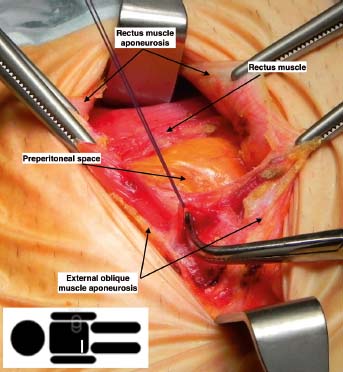
Fig. 6.2
Right inguinal region, the rectus muscle and the external oblique muscle aponeurosis are opened together and the fibers of the internal oblique and transversus muscle are split laterally. Here the ilioinguinal nerve has been found among the fibers of the internal oblique and transversus muscles and it is ready to be tied and cut
A retractor is placed so that the rectus muscle is pulled medially. The transversalis fascia is opened and the epigastric vessels are identified: they are normally retracted medially and, if necessary, they are tied and cut safely [10]. Then, following the avascular plane just underlying the epigastric vessels, the preperitoneal space is approached (Fig. 6.3).
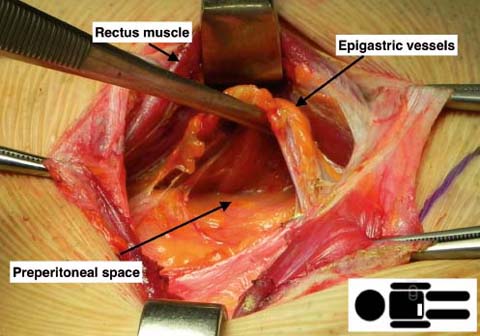
Fig. 6.3
Right inguinal region, a retractor pulls the rectus muscle medially, the epigastric vessels have been identified and the preperitoneal space is approached
The blunt dissection proceeds laterally and cranially and the psoas muscle is detectable in a deep position [3, 10] with the genitofemoral nerve running over it. Cranial to the psoas muscle, lies the quadratum lumborum muscle where the ilioinguinal and iliohypogastric nerves run (Fig. 6.4). During the procedure for the treatment of chronic postoperative pain, all the three nerves are tied, cut and buried (triple neurectomy) [9].
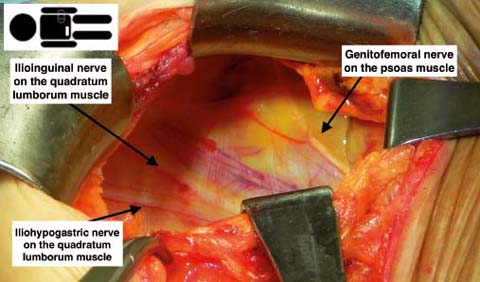
Fig. 6.4
Right preperitoneal region. Isolation of ilioinguinal and iliohypogastric nerves on the quadratum lumborum muscle and of the genitofemoral nerve on the psoas muscle
Proceeding with a blunt dissection at retropubic level, the Retzius space is reached and the Cooper’s ligament is identified (Fig. 6.5) [3, 10]: scar tissue may be present after a prostatectomy or hysterectomy or radiotherapy and consequently urinary bladder dissection from the pubic symphysis may prove difficult. If the urinary bladder has been injured during this step, an absorbable suture is done and the urinary catheter is kept in place for one week after surgery.
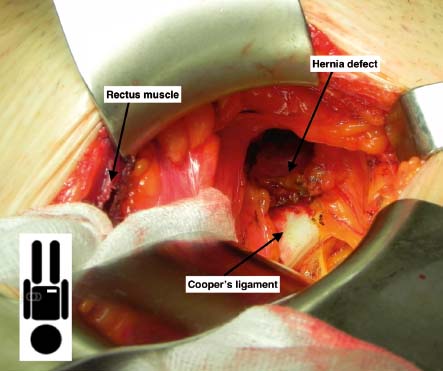
Fig. 6.5




Right preperitoneal region, isolation of the Cooper ligament and the hernia defect
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
