78 Thoracic Trauma
 Key Points
Key Points• Emergency life-threatening conditions that need to be detected during the primary survey include airway obstruction, tension pneumothorax, open pneumothorax, massive hemothorax, flail chest, and pericardial tamponade (Table 78.1).
• Urgent life-threatening conditions to detect during the secondary survey include simple pneumothorax, hemothorax, pulmonary contusion, tracheobronchial injury, blunt cardiac injury, traumatic aortic injury, diaphragmatic injury, and esophageal injury.
• Common thoracic cage injuries are not always associated with serious injury, but some individuals, especially pediatric and elderly patients, may require admission for associated injuries and respiratory therapy.
Epidemiology
Head and thoracic injuries from moving vehicle collisions (MVCs) and firearms account for the majority of the more than 160,000 injury-related deaths in the United States each year. Most fatalities occur immediately as a result of massive cardiac or vascular injury. Rib fractures are the most common thoracic cage injury following blunt thoracic trauma. Isolated first and second rib, sternum, and scapula fractures are no longer considered markers of traumatic aortic injury.1 However, rib fractures must still be considered markers of significant injury. Most patients seen in trauma centers with rib fractures will have hemothorax, pneumothorax, or a pulmonary contusion. Three or more rib fractures at any anatomic site dramatically increases the risk for spleen and liver injury. Likewise, scapula fractures are uncommon yet signify a high-energy mechanism of injury, almost always with important associated injuries.
Seat belts have increased the incidence of sternum fractures while reducing the number of lives lost in MVCs. Isolated nondisplaced sternum fractures are no longer considered markers of blunt cardiac injury.2 More complicated fracture patterns predict associated injuries. Fractures of the manubrium, manubrium-sternum synchondrosis, and proximal part of the sternum and severely displaced sternum fractures are associated with an increased incidence of spinal fractures. Displaced fractures of the body of the sternum are associated with a higher incidence of intrapulmonary and cardiac injuries.3
Thoracic Cage Injuries: Rib, Sternum, and Scapula Fractures
All thoracic cage injuries result in significant pain, splinting, atelectasis, and increased risk for pneumonia. Multiple rib fractures interfere directly with the mechanics of ventilation. Fracture fragments may penetrate the pleura and lungs and result in pneumothorax and hemothorax. Traditionally, fractures of the 6th to 12th rib on the right suggest liver injury and on the left suggest splenic injury. However, any fracture, especially multiple fractures, increases the risk for liver and splenic injuries.4
Because children have more elastic chest walls, more energy is transmitted to the underlying lung, and greater force is required for fractures. Excluding other major trauma, 71% of rib fractures in children younger than 2 years result from abuse.5
Differential Diagnosis and Medical Decision Making
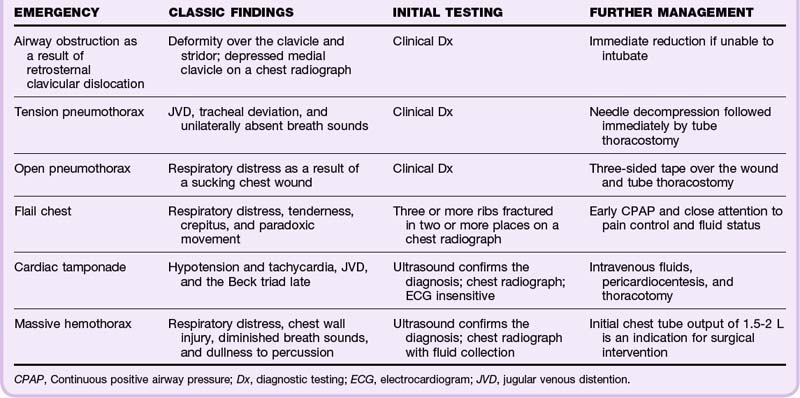
Sternum fractures are best detected on the lateral chest radiograph. Associated rib fractures and mediastinal abnormalities may be evident on the PA view. In experienced hands, bedside ultrasound may be more sensitive than radiographs for detection of both rib and sternum fractures, as well as associated hemothorax or pneumothorax.6,7 The electrocardiogram (ECG) should be examined for evidence of cardiac injury. Scapula fractures are often missed on the initial chest radiograph unless the scapular outline is specifically inspected. Shoulder radiographs can confirm suspected fractures (Fig. 78.1).
Helical computed tomographic (CT) angiography should be performed on hemodynamically stable patients when clinically significant underlying injury is suspected. An abdominal CT scan can rule out intraabdominal injury in patients with tenderness or fracture of the sixth rib or below, three or more rib fractures, hypotension noted in the field or emergency department (ED), abdominal or flank tenderness, pelvic or femoral fractures, or gross hematuria.8
Flail Chest
Flail chest occurs when three or more ribs are fractured in two or more places and a discontinuous segment of the thoracic wall is produced and moves paradoxically with respiration. Flail chest is diagnosed in approximately 5% of thoracic trauma patients seen in level I trauma centers, typically in the setting of multisystem trauma. Mechanisms include MVCs, crush injuries, assault, falls, and even minimal trauma in elderly patients. Respiratory insufficiency results primarily from the underlying pulmonary contusion. Pneumothorax occurs in 50% of cases and pulmonary contusion in 75%.9
Treatment
Immediate chest tube placement is required for assessment and management of other injuries, including pneumothorax and hemothorax. Continuous positive airway pressure is the first-line treatment in awake and cooperative patients with worsening oxygenation or ventilation.10 Criteria for intubation include airway obstruction, respiratory distress, shock, closed head injury, and need for surgery. Endotracheal intubation should be performed only when necessary to avoid the increased mortality associated with nosocomial pneumonia.
Fluid replacement should be managed carefully to avoid overhydration and worsening of lung injury. Analgesia is titrated so that patients are more willing to make sufficient inspiratory effort, but excessive sedation should be avoided. Intercostal nerve blocks, epidural anesthesia, or even surgical fixation of the flail segment may be beneficial.11 Stabilization of the flail segment in the ED or prehospital setting has not been shown to be helpful, and aggressive stabilizing efforts impede overall thoracic mechanics.
Pneumothorax and Hemothorax
Presenting Signs and Symptoms
Patients with a simple pneumothorax classically have chest pain, diminished breath sounds, crepitus, hyperresonance, and mild to moderate respiratory distress. Patients with tension pneumothorax are classically seen in extremis and exhibit jugular venous distention, tracheal deviation, unilaterally absent breath sounds, or tachycardia followed by hypotension immediately before death (or any combination thereof).12 Patients with open pneumothorax have chest wall wounds that produce sonorous sounds and are in severe respiratory distress. Typical symptoms of hemothorax are respiratory distress, chest pain, and diminished breath sounds with dullness to percussion.
Atypical manifestations are more common than classic ones. Respiratory distress may occur as a result of multiple other causes. Patients can have severe pain from distracting injuries. Breath sounds may be difficult to hear in a noisy environment. Physical examination in patients with penetrating thoracic trauma is unreliable for the detection of pneumothorax or hemothorax.13 Patients with simple pneumothorax may be minimally symptomatic or may be cyanotic and in severe respiratory distress. Tension pneumothorax most commonly occurs in intubated patients as a result of positive pressure ventilation, sometimes after overzealous bagging.
Differential Diagnosis and Medical Decision Making
In an upright patient, a hemothorax appears as a fluid layer in the affected hemithorax. Early collections are noted to blunt the costophrenic angles on the AP and lateral radiographic views. Hemothorax often appears as only a diffuse hazy infiltrate in a supine trauma patient. Hemopneumothorax has a fluid layer with a flat superior border, in contrast to the round meniscus of an isolated hemothorax (Figs. 78.2 and 78.3). Decubitus views better demonstrate a small hemothorax.

Fig. 78.2 Chest radiograph showing obvious left-sided tension pneumothorax with mediastinal shift.
(From Ullman EA, Donley LP, Brady WJ. Pulmonary trauma emergency department evaluation and management. Emerg Med Clin North Am 2003;21:291-313.)
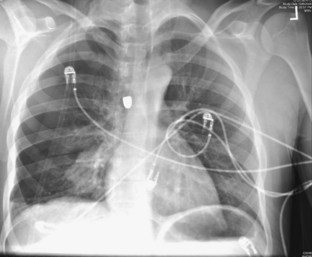
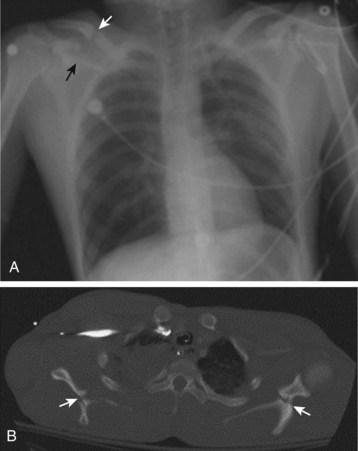
Fig. 78.3 Chest radiograph showing right hemopneumothorax along with a bullet.
(Image courtesy Dave Andreski, MD.)
An extended focused assessment with sonography for trauma (FAST) scan can diagnose pneumothorax and hemothorax with higher sensitivity than portable chest radiography can in experienced hands. An extended FAST scan is especially helpful when chest radiography is not immediately available and in mass casualty situations.14
Treatment
Tension pneumothorax and open pneumothorax are both clinical diagnoses that require immediate treatment with needle thoracostomy followed by tube thoracostomy, even when based on clinical evaluation, before radiographic confirmation. All suspicious open chest wounds should be covered with petrolatum gauze secured on three sides to prevent the entry of air during inspiration and allow the exit of air during expiration. Postprocedure radiographs should be obtained to confirm placement, drainage of air and blood, and reexpansion of lung. Prophylactic antibiotics with chest tube insertion do not reduce the risk for empyema or pneumonia.15
Follow-up, Next Steps in Care, and Patient Education
Occult traumatic pneumothorax detected on a CT scan requires only close observation for respiratory distress, progression, and the development of complications. Tube thoracostomy must be immediately available but is not required even with positive pressure ventilation.16 Any prolonged surgery, diagnostic testing, or transport preventing immediate tube thoracostomy requires prophylactic placement.
In patients with penetrating injuries and a negative initial chest radiograph, upright PA and lateral chest radiographs should be repeated in 3 to 4 hours.17 Patients with normal findings on repeated radiographs and no significant associated injuries are discharged with wound care and follow-up instructions. Patients with asymptomatic blunt chest trauma and normal findings on the initial chest radiographs do not require repeated films before discharge. All patients with chest tubes are admitted to the trauma, cardiothoracic, or general surgery service in the care of personnel experienced in managing chest tube equipment.
Pulmonary Contusion
Differential Diagnosis and Medical Decision Making
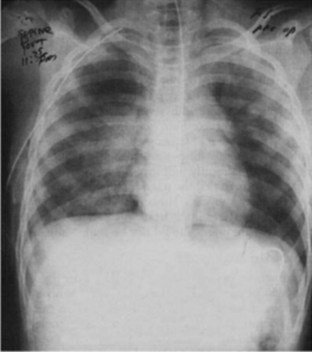
The patchy or diffuse air space opacification above the site of injury with pulmonary contusion is often present on the initial chest radiograph and typically progresses over the first 6 hours (Fig. 78.4). Initial CT scanning is more sensitive than chest radiography but seldom changes the initial management of pulmonary contusion. Pulse oximetry is essential to detect early clinical deterioration.
Follow-up, Next Steps in Care, and Patient Education
Patients with pulmonary contusion require admission to the intensive care unit for oxygen administration, chest physical therapy, incentive spirometry, suctioning, analgesia, and close monitoring. Overhydration must be avoided to prevent iatrogenic worsening of capillary leak and lung function. Prophylactic steroids and antibiotics are not recommended.18 Isolated pulmonary contusions typically resolve within 14 days without long-term complications. Disability and mortality rates are higher in patients with larger areas of contusion, flail chest, acute respiratory distress syndrome, and pneumonia.







