25 Pediatric Orthopedic Emergencies
 Key Points
Key Points• Ligaments are stronger than bones in young children.
• The history should be consistent with the injury and the developmental stage of the child.
• Children are poor at localizing pain and often refer symptoms to neighboring joints. The pathologic site in knee pain may be the hip.
• Growth plate injuries are subtle but have the potential to lead to growth arrest.
• Radiographs of the contralateral side are useful as comparison views for the investigation of subtle fractures.
Radial Head Subluxation
Presenting Signs and Symptoms
A number of reduction techniques are used, including the hyperpronation method and the supination-flexion method. The hyperpronation method has proved more effective and appears to be less traumatic.1 With the arm held in extension, the wrist is hyperpronated and a click is sometimes heard. In the supination-flexion approach the examiner places the thumb of one hand over the radial head and provides countertraction. Next, while holding the wrist, the elbow is pulled into extension. The final phase is supination and flexion at the elbow. Most children return to full functioning within 15 minutes, and the child should be observed until full range of motion is regained.
Fractures
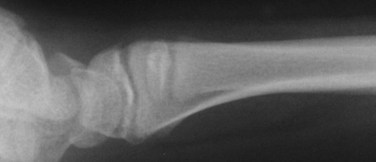
Pediatric bones are less dense and therefore more prone to compression or bending when an axial load is applied. Falls onto an outstretched arm may result in torus or buckle fractures (Fig. 25.1). Greenstick fractures are incomplete, with the cortex remaining intact on one surface. To obtain complete reduction, completion of the fracture is necessary. Bowing fractures result when the force is insufficient to cause a complete break but results in deformation of the osseous structure (Fig. 25.2). Cosmetic deformity and functional abnormality will result without complete reduction. Repair is often difficult because both cortices remain intact.

Salter-Harris Classification of Fractures
The most commonly used system to identify physeal injuries is the Salter-Harris classification. Fractures are categorized as types I through V, with the higher numbers having the greater risk for growth abnormalities. All such injuries require pediatric orthopedic follow-up.2
Type II fractures, the most common type, occur when a piece of the metaphysis remains attached to the epiphysis (Fig. 25.3). They require splinting and generally carry a good prognosis. Types III and IV are intraarticular fractures that also involve the growth plate. In a type III injury, the fracture line extends through the epiphysis into the physis. In type IV, the fracture passes through the epiphysis, physis, and metaphysis. Types III and IV carry a risk for growth retardation, altered joint mechanics, and functional impairment and thus require urgent orthopedic evaluation. Type V fractures are compression injuries and are difficult to visualize on radiographs. The diagnosis is often made retrospectively following a case of growth arrest.









