53 Lung Transplant Complications
 Key Points
Key Points• All lung transplant recipients with respiratory complaints should be assessed for the possibility of rejection and parenchymal lung infection. In most cases, assessment leads to admission to the hospital.
• Rejection and pulmonary infection are frequently indistinguishable. The clinical manifestation of pneumonia and lung allograft rejection may be subtle, and admission is required to address both entities.
• Lung rejection is common and can occur anytime after transplantation.
• Transplanted lungs are highly susceptible to pneumonia. Cytomegalovirus pneumonia is the most common opportunistic pulmonary infection after lung transplantation.
Scope
More than 1500 lung transplants are performed each year in the United States; worldwide, approximately 3000 were performed in 2009.1 Survival rates had been rising in recent years because of technologic advances in surgical technique and immunobiology, but they seem to have reached a plateau. The current survival rate 1 year after transplantation is 79%.1 Multiple conditions necessitate lung transplantation, including cystic fibrosis, end-stage chronic obstructive lung disease, and interstitial lung disease (Box 53.1).2 The primary reason for bilateral lung transplantation is chronic obstructive pulmonary disease.3
Box 53.1
Reasons for Lung Transplantation
Emphysema/chronic obstructive pulmonary disease
Primary pulmonary hypertension
Lung retransplantation (rejection, graft failure)
From United Network for Organ Sharing, 2007. Available at www.unos.org.
The number of patients who have undergone solid organ transplantation increases every year. In 2008 alone, 27,281 organ transplantations were performed in the United States.2 This figure represents a large number of patients who might seek medical care in an ED. In addition, current survival rates are rising. In 1998, 1-, 3-, and 5-year survival rates were 70.7%, 54.8%, and 42.6%, respectively, for lung transplant recipients. In 2009, the rates were 79%, 63%, and 52%.1 Although survival rates for lung transplantation lag behind those for other solid organ transplantations, enhancements in immunotherapy will probably continue to advance.4,5
Complications Related to the Surgical Procedure
The type of transplant (single lung, double lung, combined heart and lung, lobar) depends on the recipient’s disease and the particular transplant center where the procedure is performed.6 Single-lung transplantation requires a lateral thoracotomy incision, and double-lung transplantation requires a double thoracotomy (“clamshell”) incision. The heart may be transplanted along with one or both lungs. In some cases, a lobar segment of donor lung is transplanted. The surgical procedure includes anastomosis of the pulmonary arteries, veins, and bronchus.
Emergency Department Presentation
Patients who have undergone lung transplantation should be considered high risk when seen in an ED for evaluation. Because many patients live far from the facility where their surgery was performed, they are likely to go the nearest ED when problems arise. In a retrospective review of 131 lung and heart-lung transplant patients who visited an ED, the most common complaints were fever (37%), shortness of breath (13%), gastrointestinal symptoms (10%), and chest pain (9%).6,7
Differential Diagnosis
Patients who have undergone lung transplantation may come to the ED with myriad complaints. Among the most important complications are acute or chronic allograft rejection and infections. To make matters more complex, the required use of immunomodulating agents may diminish or mask objective findings. In addition to rejection and infection, patients in the early postoperative period are at risk for mechanical complications such as bronchial dehiscence. It is important to ascertain the procedure that was performed and the technique that was used. Patients who have received single-lung transplants are at risk for infection, cancer, and other complications in both the transplanted and the native lung.8
Rejection
Lung allograft rejection is one of the most feared life-threatening complications of lung transplantation; in some cases, the emergence of rejection necessitates retransplantation. The majority of transplant recipients experience at least one episode of rejection. Patients who experience repeated episodes of allograft rejection are at increased risk for chronic rejection (bronchiolitis obliterans syndrome).9–11
The clinical findings in patients with lung allograft rejection can be nonspecific or even silent12 (Box 53.2). Patients may report a dry cough, subjective fevers, varying degrees of shortness of breath, or any combination of these symptoms. Episodes of rejection cannot be distinguished from pulmonary infection on clinical grounds alone.9 The important point for EPs to remember is that the symptoms of allograft dysfunction or rejection may be subtle. Patients may not appear ill or seem to have anything more than a viral upper respiratory tract infection.13,14
During the first 6 months after transplantation, chest radiographs may show pleural effusions, interstitial edema, or perihilar infiltrates. Episodes of rejection occurring after this time tend to not lead to abnormalities on the chest radiograph. Normal chest film findings do not rule out the presence of underlying rejection. In the ED, chest radiographs may help in the evaluation of entities that would require immediate therapy, such as pneumothorax or a large pleural effusion.13,14
Lung allograft rejection is not usually diagnosed in the ED. Typically, patients are admitted and must undergo fiberoptic bronchoscopy and biopsy for diagnosis. Treatment of suspected lung transplant rejection begins with clinical suspicion. In all cases of suspected rejection, the patient’s pulmonologist or lung transplant surgeon should be contacted. This potentially life-threatening entity should be treated before the results of bronchoscopy become available. The biopsy indicates the presence and degree of tissue rejection and inflammation. The complex and histologically directed scale of rejection is beyond the scope of this chapter. The main ED treatment for patients with rejection is high-dose intravenous corticosteroids. Patients are usually given intravenous methylprednisolone at a dose of 0.5 to 1.0 g/day for 3 days, with the first dose given in the ED. If rejection is present, the symptoms should resolve rapidly. The therapy is then switched to oral corticosteroids. It is essential that rejection be diagnosed and treated in the ED in consultation with the patient’s transplant physician.9 Other interventions for acute rejection include methotrexate, muromonab-CD3, antithymocyte globulin, total lymphoid irradiation, and extracorporeal photopheresis.15–18
Infectious Complications
Despite or possibly as a result of advances in immunosuppression, infection is a common complication after any solid organ transplantation, particularly of the lung.19–21 Because of the lung parenchyma’s interaction with the environment, the most common infection is pneumonia, but any opportunistic infection can occur.
Infectious complications after organ transplantation have been studied extensively and are related to multiple factors, the most important being the time since transplantation. Infections in organ recipients can be broken down into three periods (Fig. 53.1).
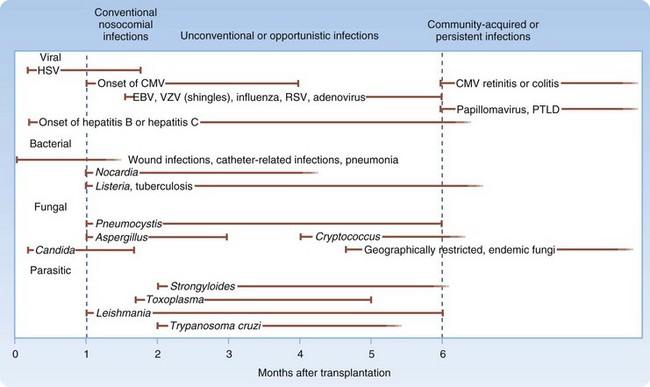
During the first month after transplantation, nosocomial infections predominate. Wound infections, urinary tract infections, pneumonia, and vascular access infections are common in this period. Opportunistic infections, such as those caused by Pneumocystis and Nocardia species, do not usually occur in the first month after transplantation.22 Infections that emerge 1 to 6 months after solid organ transplantation include many of the opportunistic infections, such as those caused by Pneumocystis carinii and Listeria monocytogenes. In addition, immunomodulating viruses (particularly cytomegalovirus [CMV]) become important pathogens. Epstein-Barr virus, hepatitis B virus, hepatitis C virus, and human immunodeficiency virus can also produce infection during this time frame.22
Viral infections that emerge after the first month following transplantation may be associated with chronic or progressive infection and may cause significant injury to the affected transplanted organ. Patients who experience chronic or recurrent bouts of organ rejection are invariably exposed to higher and prolonged periods of immunosuppressive therapy and thus tend to be vulnerable to these opportunistic pathogens.1
Pulmonary Infections
The lungs are particularly vulnerable to infection after solid organ transplantation. The highest risk for posttransplantation pulmonary infection occurs in lung transplant recipients. Pulmonary infections are the most common infectious complication in heart and lung transplant recipients19–21 and the least common in kidney transplant recipients.23 Multiple factors explain this higher incidence of lung infections (Box 53.3).








