Immediate Assessment and Management
- Start with the ABCs as discussed in Chapter 1.
- Apply direct pressure to stop any bleeding.
- Expose the affected part; cut off clothes as necessary.
- Take a brief but comprehensive history.
- Confirm that the presenting problem is confined to the limb.
- Injuries around the shoulder and thigh may cause hypovolaemia
- Painful limb injuries may be associated with life-threatening, but less painful, trunk trauma
- Limb infection may have systemic effects
- Limb pain may be symptomatic of trunk pathology (e.g. cardiac pain, sciatica and herpes zoster infection)
- Confirm the presence of distal pulses and the integrity of the nerve supply.
- Splint fractures.
- Give analgesia early on; this may be systemic or local.
- Finally undertake a detailed local examination including a comparison with the opposite limb.
If there is a clear history of trauma, it is useful to reconstruct the incident to appreciate the forces applied and to consider the biomechanics of the injury:
- Healthy young bones will undergo considerable elastic deformation (e.g. the femoral shaft will bend over 10° before breaking). At breaking point, stored energy is released and the limb suddenly deforms further, inflicting secondary soft-tissue injury. Often, this is more important than the underlying fracture.
- Twisting tends to produce spiral fractures.
- Direct blows cause transverse fractures, which may be compound.
- Sheering forces raise contused skin flaps.
- Forces applied to the heel of the falling body and causing a fracture of the os calcis will be transmitted cranially and may produce a fracture of the lumbar spine or the base of the skull.
- An evident knee injury, sustained by a front-seat car passenger, may draw attention away from an occult hip dislocation.
Wounds
Wounds should not be explored at this stage. Sterile dressings or iodine soaks are the only necessary treatment. An instant photograph of the injury will prevent the need for frequent re-examination by attending doctors. Foreign bodies must be left alone, even if they are grossly protruding, until resuscitation has begun and the environment and staff are prepared for a careful, controlled assessment. Patients with grossly contaminated wounds and compound fractures should receive intravenous (IV) antibiotics (e.g. flucloxacillin) and antitetanus prophylaxis as soon as possible.
Pain
Splintage and reassurance are very important. Pain may be controlled by nitrous oxide while a splint is applied. Intravenous injection of opiates should be given as soon as contraindications have been excluded. In some situations a local anaesthetic block may be preferable.
Radiographs
Radiographs complement but do not replace a full clinical examination. Good radiographs demand good viewing facilities. The doctor should have a high-quality screen and charts showing the times of appearance and fusion of primary and secondary ossification centres.
Vascular Problems Related to Injury
Occlusion
Fractures around the elbow and the knee are commonly associated with vascular occlusion. Do not assume that distal ischaemia has been caused by transient vascular spasm. Urgent specialist referral is necessary. Limb viability is threatened if a major occlusion persists for 4 h or more.
Bleeding
Elevation is an effective first-aid measure for major venous haemorrhage but is often impossible to achieve because of associated bony injury. Applying artery clips to spurting vessels in the emergency department (ED) will usually inflict further injury, especially as most major limb vessels run alongside peripheral nerves. Instead, local pressure should be applied. Bleeding into damaged muscle is a much more common problem.
Compartment Syndrome
The closed fascial compartments of the limbs prevent contused muscles and haematomas from expanding indefinitely. Interstitial pressure rises causing pain and ischaemia (→ p. 110).
Plaster Casts
Application of a cast is the most common way of immobilising an injured area of a limb, be it an injury to the bone or to the soft tissue. However, acute injuries may swell considerably in the first 48 h and restriction of that expansion by a cast can cause severe ischaemia. The inelasticity of fascial compartments, particularly in the lower leg, can have a similar effect.
Splitting a cast (a single, longitudinal split is the best) or prescribing an incomplete slab-type plaster does not necessarily protect the limb from the underlying ischaemia. All ED plasters must be well padded, especially over bony protuberances, and the patient must have:
- instructions to elevate the limb and crutches or a sling if needed
- advice on the care of the cast and a written list of the signs of ischaemia (plaster instructions)
- early review.
All staff who deal with patients in casts must be aware of the need to look out for the signs of compartment syndrome (→ p. 110) as well as the more widely appreciated changes to the warmth, colour and capillary refill of the digits.
The National Institute for Health and Clinical Excellence (NICE) recommends that all patients who are being treated with a plaster cast on the lower limb should be risk assessed for venous thromboembolism (VTE). If they are found to be at significant risk of VTE, they should be offered thromboprophylaxis for the duration of the treatment.
Physiotherapy
The help of the physiotherapist can be invaluable in treating a wide range of soft-tissue injuries and other conditions. Particular benefits are seen with early physiotherapy and include the following:
- Reduction in pain, bruising and swelling
- Maintenance of muscle fibre length and range of movements
- Early mobilisation and restoration of function.
The physiotherapist also offers:
- Re-examination of the injury and the level of function
- Assessment for and training with walking aids
- Restoration of the patient’s confidence
- Skilled follow-up.
Crutches
Crutches are required for emergency patients with a large variety of differing problems. They may be designed to enable a limb to be:
- non-weight-bearing (axillary crutches)
- partial weight-bearing (elbow crutches).
All patients given crutches must be instructed about their safe care and usage and should also be observed in action.
Local Injection of Steroids
The injection of a long-acting steroid-type drug into a joint, tendon sheath, bursa or other suitable area can bring long-lasting relief to a large number of inflammatory soft-tissue conditions. The steroid is often premixed with local anaesthetic to:
- minimise the discomfort of the injection
- give some immediate relief of the underlying condition
- act as a marker of successful localisation of an injection.
Complications of depot steroid injection include the following:
- Local damage
- Introduction of infection
- Rupture of a tendon
- Fat necrosis and atrophy and disfigurement of overlying skin.
As such, it is a technique that requires the following knowledge:
- The local anatomy
- The best approaches to the target area
- The correct drug dosage for each site (→ Table 7.1).
Table 7.1 Dose of methylprednisolone for local injection
| Joint | Dose | |
| (mg) | (mL) | |
| Large joint (knee, ankle, shoulder) | 20–80 | 0.5–2 |
| Medium joint (elbow, wrist) | 10–40 | 0.25–1 |
| Small joint (MCPJ, IPJ, ACJ) | 4–10 | 0.1–0.25 |
| Bursa | 4–30 | 0.1–0.75 |
| Periarticular (for epicondylitis) | 4–30 | 0.1–0.75 |
| Tendon sheath (never into a tendon) | 4–30 | 0.1–0.75 |
ACJ, acromioclavicular joint; IPJ, interphalangeal joint; MCPJ, metacarpophalangeal joint.
Local injections of steroid should not be given by inexperienced staff or in circumstances where there are no facilities for review of the patient.
Sports Injuries
Soft-tissue and bony injuries, secondary to trauma sustained during sport, are common presentations. Many such injuries can also occur during non-sporting activities. There are three specific needs of the sportsperson:
Accurate diagnosis is essential. A good general recipe for treating sports injuries is:
- 3 days’ complete rest (crutches/sling if required)
- appropriate analgesia
- early physiotherapy.
Ice, compression and elevation are useful in the early stages to reduce discomfort and swelling. There should be a return to about 50% training levels as soon as possible and then a gradual build-up to full activity.
THE HIP AND THIGH
Dislocation of the Hip
This is caused by axial violence such as a force applied to the knee. The dislocation is usually posterior with a fracture of the acetabular rim. Sometimes the sciatic nerve is injured – most frequently that part destined to be the common peroneal nerve. Pain is usually severe and the hip is held partially flexed and adducted. Central dislocation into the pelvis is associated with major (concealed) blood loss. Dislocation of an arthroplasty of the hip is often seen after relatively minor trauma.
XR
When resuscitation has been established and analgesia given, radiographs are obtained. Later a CT scan will aid identification of complex acetabular rim fractures.
TX
Resuscitate and provide analgesia; support the limb but do not attempt reduction in the ED. The distal neurovascular function must be assessed and the secondary survey completed, looking for other injuries. The patient needs an urgent referral to the orthopaedic department.
Both types of traumatic dislocation can be difficult to reduce by closed manipulation. Posterior dislocation may be treated more appropriately by open reduction and internal fixation of the bone fragments.
Fracture of the Hip (Fracture of the Proximal Femur)
There are three circumstances in which this may occur:
A detailed history must be taken and other injuries excluded. Consider the reason for an unexplained fall (medication, domestic disorganisation) and assess general health. The following notes assume that systemic examination has been undertaken and relate to the care of the typical elderly patient with an isolated injury.
The patient (usually female) presents as unable to weight-bear after a relatively minor fall. Some patients may be able to walk, albeit with a painful limp. There is pain in the hip, thigh or knee but usually no visible swelling, bruising or deformity. The affected leg may be shortened and externally rotated but this classic appearance is dependent on the grade of the fracture. A more valuable sign is pain on gentle passive rotation of the extended leg. If the fracture has impacted, other movements may be good with minimal pain including even straight-leg raising. Tenderness is most marked posteriorly. Significant blood loss is unusual and associated vascular and tendon damage is rare.
 Box 7.1 How to examine the hip joint
Box 7.1 How to examine the hip joint- Assess gait and continue inspection of mobility and pain as clothes are removed and the patient gets on to the couch
- Look for shortening or rotation of the leg. True shortening is caused by collapse or angulation of bone (distance between anterosuperior iliac spine and medial joint line of knee – both legs in the same position). Apparent shortening is the difference between the two sides when the patient is lying supine (distance from umbilicus to medial malleoli). It is usually caused by pelvic tilt or fixed deformity at the hip joint
- Look at the groin, perineum, buttock and lateral bony prominences, and feel for tenderness in these areas. A sinus or old scar may point to established disease but there are usually no surface signs of acute inflammation or of joint effusion
- Assess flexion, abduction, adduction and rotation in each leg (active before passive). Keep one hand under the lumbar spine when testing flexion and one hand on the opposite iliac crest when testing abduction and adduction. Rotation is most accurately measured with the knee at right angles (lower leg over the end of the couch or patient prone). With the patient lying on his or her side attempt to extend the hip joint backwards; 5–10° is often possible
- Examine the relationship between hip movement and lumbar spine and pelvic movement. Fixed flexion of the hip can be camouflaged by excessive lumbar lordosis. Fixed adduction is usually compensated for by pelvic tilt. The easiest way to abolish the lordosis is to fully flex the leg that is not being measured. Any passive movement off the bed of the leg under assessment is fixed flexion. Similarly, setting the pelvis square may cause fixed adduction of one leg
- Finally, ask the patient to stand on one leg. The pelvis should rise on the non-weight-bearing side. Failure to do this is a positive Trendelenburg sign and indicates disease in the weight-bearing hip or its associated abductor muscles
XR
Radiological examination must include an anteroposterior (AP) view of the hips and pelvis, and a lateral radiograph of the affected hip. In the AP view, look for a break in the normal apparent continuity of trabeculae across the joint.
Osteoarthrosis is associated with intertrochanteric rather than subcapital fractures, so it is very unlikely that an undisplaced subcapital fracture will be hidden in the disorganised radiological pattern around an arthritic joint.
Up to 5% of fractures in osteoporotic bone are not immediately visible on plain radiographs. An MR scan should be performed if a hip fracture is suspected but initial radiographs are normal. A CT scan is an alternative if MRI is not available within 24 h of admission. For different types of proximal femoral fractures → Box 7.2.
 Box 7.2 Hip fractures (or proximal femoral fractures)
Box 7.2 Hip fractures (or proximal femoral fractures)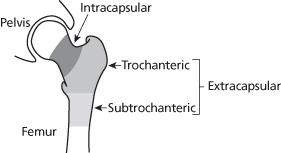
TX
A box splint may be used to control leg movements and analgesia should be given immediately (and the effect of these measures assessed after 30 min). Long waits on hard trolleys must be avoided because these patients acquire pressure sores very quickly. (For risk factors for pressure sores → p. 222.) Internal fixation, hemiarthroplasty or total arthroplasty is usually performed on the day of admission or at least within 24 h of injury.
Fracture of the Pubic Rami
The anterior pelvis should be carefully examined in all cases. Fracture of the pubic rami occurs in the same group of patients as those with fracture of the hip and gives a very similar clinical picture. The pain may be felt in the buttock or groin but otherwise symptoms are localised to one leg and may divert attention away from the pelvis. Patients with this injury need initial bed rest and analgesia and then gradual mobilisation (also → p. 84).
The Elderly Patient with Failure to Weight-Bear After a Fall
All such patients must be admitted for reassessment and mobilisation. A considerable number prove to have a fracture that was not evident on the initial radiograph. An MR scan should be performed if a hip fracture is thought to be a possibility (i.e. in most elderly patients) but initial radiographs are normal. A CT scan is an alternative if MRI is not available within 24 h of admission. Patients with soft-tissue injuries may require prolonged rehabilitation before they are ready for discharge. Local policy dictates whether care for these patients is provided by the geriatric or orthopaedic department.
Degenerative Disease of the Hip
The patient presents with pain and stiffness and may relate this to a recent injury. The hip joint has a restricted range of movement. Fixed flexion may be obscured by compensatory lumbar lordosis. Fixed adduction causes pelvic tilt and an apparently short leg. Pain is usually most marked at the extremes of the range and there is little muscle spasm. A general examination is always indicated to exclude systemic disease and injury.
XR
Radiographs show reduced joint space, irregular articular surface, osteophytes, sclerosis and bone cysts. Such changes, however, are common and may not be related to the patient’s symptoms.
TX
In the absence of other pathology, symptomatic treatment with analgesia and a walking aid should be offered. The patient should be advised to consult his or her GP. Physiotherapy may help with initial mobilisation.
Irritable Hip
This is a common condition in children. The child, usually under the age of 5 years, presents with a limp that is unrelated to trauma. Occasionally, the sore hip gives way and creates the illusion of a traumatic injury. Pain in the hip region may not be immediately evident and passive movements are usually normal. Sometimes mild protective spasm may limit abduction. There may be a history of a prodromal upper respiratory infection.
The condition is thought to be caused by a transient synovitis, possibly of viral origin, and is invariably unilateral. It is important to exclude a septic arthritis
 Box 7.3 The management of a young child who is limping or not weight-bearing
Box 7.3 The management of a young child who is limping or not weight-bearing- Ask about duration and severity of limp
- Ask about a history of trauma, viral infection or previous episodes
- Take the temperature
- Observe the gait
- Ask the child to stand on alternate legs
- Examine the whole limb, feeling carefully, especially for tibial tenderness and hip spasm in abduction
- Consider the need to obtain radiographs of the whole limb
- If there are no specific clinical or radiological findings, reassure the parents and recommend rest and paracetamol elixir for the child. Arrange for review within 72 h
XR
Radiographs of the affected limb from hip to ankle are usually required. The foot may need to be included if there is any tenderness in this area. The main differential diagnosis is a toddler’s fracture or other tibial injury (→ p. 100).
Ultrasound examination can demonstrate an effusion in the hip joint but cannot differentiate synovial fluid, blood and pus. A difference of >3 mm of effusion between the normal and the affected hip is considered to be pathological. A positive ultrasound scan obviates the need for radiographs.
TX
If there is an unexplained pyrexia and/or hip muscle spasm refer the child to the orthopaedic department for admission. A child who is apyrexial with no hip spasm and no evidence of bony injury can be discharged with analgesia and instructions to rest but must be reviewed in the ED review clinic within 72 h.
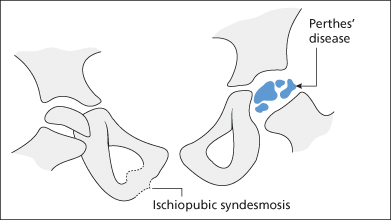
Perthes’ Disease
Perthes’ disease is an idiopathic avascular necrosis of the proximal femoral epiphysis. It is often called an ‘osteochondritis’ and belongs to a group of similar diseases of epiphyseal growth (→ p. 350). In the UK, it affects 1 in 10 000 children and is four times more common in boys than in girls. In 10% of cases it is bilateral. Children aged between 3 and 15 years may be affected, although it is most common in children between 5 and 8 years of age. It presents with a painful or painless limp or sometimes with hip or knee pain after exercise. Pain may be mild and is often of several months’ duration. There is restriction of hip movements with muscle spasm, especially internal rotation and abduction. Flexion is usually unaffected.
XR
Radiographs may be normal in very early disease. However, they often show remarkably advanced changes in contrast to the short clinical history. The femoral neck may be widened, bone density reduced, joint space increased and the femoral head fragmented (→ Figure 7.1). An ultrasound scan reveals an effusion and bone scanning shows reduced uptake in the affected epiphysis. Blood tests are all normal.
TX
The child should be referred to the orthopaedic department for admission. Bed rest until the muscle spasm has resolved is now the mainstay of treatment for this condition.
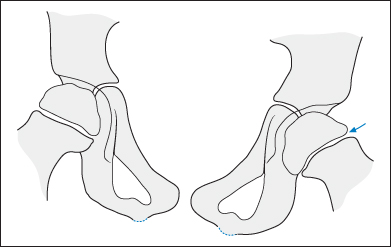
Slipped Upper Femoral Epiphysis
The capital (or proximal femoral) epiphysis may slip suddenly or gradually, usually in a teenager who is having a pubertal growth spurt. The onset may be linked to minor trauma. There is limping and pain, which may be localised to the distal thigh or knee. Hip abduction is restricted but adduction is often increased. Flexion and internal rotation may increase the pain because these movements stretch the joint capsule. An acute slip is more likely to lead to ischaemia and avascular necrosis of the epiphysis than the more common chronic slip.
XR
Radiographs may be difficult to interpret and should include AP and lateral views of both hips. Posterior movement of the epiphysis is sometimes the first radiographic sign and is best seen on the lateral view. Slight medial displacement of the epiphysis is usually the initial change and is sometimes likened to ‘an ice-cream sliding off its cone’ (→ Figure 7.2). More specifically, a line drawn parallel to the femoral neck (Klein’s line) will normally intersect with the lateral portion of the femoral epiphysis (Trethowan’s sign).
TX
Immediate referral to the orthopaedic department is essential. Surgical reduction of an acute slip followed by prophylactic pinning is usually recommended.
Extra-Articular Problems Around the Hip
Spinal and abdominal lesions may present with hip symptoms:
- Infection of the lumbar spine may produce a psoas abscess, which points just below the inguinal ligament. This may be tuberculous or as a result of a variety of agents in drug addicts.
- A femoral hernia may be overlooked, especially in an obese, elderly woman.
- A high lumbar disc lesion may present with anterior thigh pain and limitation of hip extension (the femoral stretch test).
- Constriction of the lateral cutaneous nerve of the thigh as it passes through the inguinal ligament may cause persistent pain over the thigh (meralgia paraesthetica).
- A child with haemophilia may present with hip joint spasm caused by haemorrhage into the psoas muscle.
Fracture of the Femoral Shaft
This is associated with extensive soft-tissue injury and internal bleeding but is not usually compound. The level of trauma required to fracture the femur should suggest the possibility of serious injuries elsewhere.
XR
The diagnosis should be clinically evident without immediate resort to radiographs, which are mainly used to exclude other injuries and to check the position of the bone after the application of a splint.
TX
Priorities are as follows:
- Complete ABCs
- Give effective analgesia, initially nitrous oxide mixture and then IV opiates and/or a femoral nerve block (→ Box 7.4)
- Apply Thomas’ or other traction splint (→ Box 7.5)
- Check distal pulses; vascular damage can occur with supracondylar fractures
- Withdraw blood for baseline values and cross-match
- Complete the secondary survey
- Take radiographs as appropriate
- Involve the orthopaedic team early in management.
 Box 7.4 Femoral nerve block
Box 7.4 Femoral nerve block Box 7.5 Splinting a femoral shaft fracture
Box 7.5 Splinting a femoral shaft fracture- If Thomas’ splint is to be used, obtain the appropriate size and cover it with tubular bandage or webbing slings. If a traction splint is to be used much of the following can be omitted, but ensure that you know how it works before trying to apply it
- Apply the strapping from the skin traction kit to the leg. Adhesive strapping must not be used on elderly or fragile skin because its removal later may damage the skin. Instead, use a non-adhesive traction kit
- Protect the malleoli by padding
- Secure the strapping with crepe bandages
- Ensure adequate analgesia. Intravenous analgesia can be supplemented with nitrous oxide while applying the splint
- Grip the heel and forefoot of the injured leg and apply firm continuous traction. Muscle spasm will gradually disappear and angulation of the thigh will decrease. Transient increase in pain is usually reduced by continuous traction
- Instruct an assistant to manoeuvre the splint over the foot and ankle
- Maintain constant traction while the assistant pushes the splint towards the pelvis
- Protect the genitalia
- Fasten the strapping by its ropes to the end of the splint
- Tighten the traction by inserting a wooden spatula between the two ropes and twisting it until the required tension is achieved (Chinese windlass method)
- Check the foot pulses and toe movements
- Request a radiograph to check the position of the splint
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


