Fig. 29.1
Carl-Ludwig Schleich, father of infiltration anaesthesia, insisted that local anaesthesia could decrease or eliminate the need for general anaesthesia. He advocated training in anaesthesia. (The picture, taken around 1905, is from the collection of the author.)
Nevertheless, many German surgeons, chemists and other physicians, produced anaesthetic innovations. These included the introduction of regional anaesthesia, development of the barbiturates, and invention of anaesthesia apparatus.
Local and Regional Anaesthesia
The 1884 discovery of cocaine’s anaesthetic properties by the ophthalmologist Carl Koller (1857–1944) of Vienna, introduced local and regional anaesthesia [2]. The same concentrations of cocaine used for topical anaesthesia were then used for injection, and such high concentrations sometimes caused fatal complications, leading other investigators, including Schleich, to dilute the solutions to produce “infiltration anaesthesia”.
Schleich described his techniques in a lecture to the 21st annual Congress of the German Surgical Society in 1891 in Berlin. After reviewing infiltration anaesthesia including indications, and the pros and cons, using humanistic, legal and ethical arguments, Schleich denounced chloroform anaesthesia as dangerous, and denied the need for general anaesthesia for most surgical procedures. A tumult arose. Although the audience knew little about the new technique, nobody agreed with Schleich’s arguments, and he left the congress without further discussion. Schleich continued to perform major surgical procedures including hernia repair, laparotomy, and limb amputation under infiltration anaesthesia, stating that general anaesthesia was not needed. The initial negative response eventually subsided, and his method was later considered a “great feat in the discipline of surgery in Germany” [3].
In 1894, Schleich again inflamed his fellow surgeons by arguing, in his textbook “Schmerzlose Operationen” (Painless Surgery), that only specially trained physicians should perform anaesthesia, and moreover that the specialist should teach younger colleagues. This was then a revolutionary concept in Germany [4].
Regional Anaesthesia: Further Developments
At the end of the nineteenth century, the side effects of cocaine inspired the German chemist Alfred Einhorn (1856–1917), to search for a better local anaesthetic. In 1904, Einhorn and his colleagues produced procaine (Novocaine), which until the 1940s discovery of lidocaine by Swedes Nils Löfgren (1913–1967) and Bengt Lundquist (1878–1922), was the prototypic local anaesthetic.
In 1903, Heinrich Braun (1862–1934) of Leipzig recommended adding adrenaline to cocaine to decrease the speed of absorption. This allowed the safe administration of larger amounts of cocaine and more extensive surgery. Braun also realized that the simultaneous use of adrenaline would minimize procaine’s vasodilating properties, decrease the toxic side effects of procaine and prolong its anaesthetic properties. Not surprisingly, procaine became the most important local anaesthetic for decades, world-wide. In the 1920s, variants of procaine, such as isocaine and nirvanine were introduced, but failed to challenge procaine [5].
Specialized regional anaesthesia techniques including splanchnic, paravertebral, sacral-caudal and brachial plexus blocks, were developed subsequently and local anaesthesia increasingly displaced general anaesthesia. Braun described these new options in his famous textbook “Local Anaesthesia’Scientific Basis and Practical Use”, first published in 1905, with several editions following until 1951 [6]. A 1914 translation popularized local anaesthetic techniques in the English-speaking world [7].
Arthur Läwen (1876–1958) trained with Braun, and in 1933 succeeded him as editor of the textbook. Läwen enthusiastically supported local and regional anaesthesia. He provided a clinical evaluation of a bicarbonated procaine solution, which he developed in collaboration with his pharmacological colleague Oskar Gross (1877–1947) from Leipzig. This preparation had a faster onset, longer duration of action, and less potential for toxicity [8].
New Conduction Anaesthesia Techniques are Established
In 1911, Georg Hirschel (1875–1963) invented the axillary approach to the brachial plexus while Diedrich Kulenkampff (1880–1963) described the supraclavicular approach. Hirschel also published a textbook of local anaesthesia which gained world-wide recognition due to its excellent illustrations and detailed descriptions. Several editions were published in Germany. Translations into English, French, Spanish and Russian popularized local anaesthetic techniques outside Germany [1].
Spinal Anaesthesia
In 1899, August Bier (1861–1949; Fig. 29.2), a colleague of the Kiel surgeon, Friedrich von Esmarch (1823–1908), administered the first spinal or regional “block” to adult patients. Bier sought to “render a large part of the body insensitive to pain for surgical purposes.” Using a fine hollow needle, as described by Heinrich Quincke (1842–1922), Bier performed a lumbar puncture with the patient in the lateral recumbent position. The puncture itself was made painless by local anaesthetic infiltration using Schleich’s method. Bier then injected 0.10–0.15 mg of cocaine into the lumbar subarachnoid space. Following an initial enthusiasm, German surgeons rejected the new method because of reports of severe side effects [9].

Fig. 29.2
August Bier gave the first spinal block and invented intravenous regional anaesthesia. (The picture, taken around 1910, is from the collection of the author.)
Bier himself called for caution in applying the method. The problem of an excessively high spinal block with its attendant side effects represented a major challenge, and the means to prevent these adverse reactions were often inadequate. Side effects such as the unsolved problem of postoperative nausea and vomiting, post spinal headache, and hypotension caused Bier to call for restricted use of the brand-new technique. Moreover, the analgesic cocaine was far from the ideal anaesthetic [10]. Thus, most physicians contented themselves with local infiltration and inhalation anaesthesia and only a few enthusiasts persisted in administration of spinal anaesthesia [11]. In the mid 1920s, new atraumatic spinal needles and hypo- or hyperbaric anaesthetic solutions renewed interest in spinal anaesthesia [12]. A better knowledge of physiology and newly developed vasoconstrictive drugs like ephedrine, further augmented enthusiasm [13].
In the 1930s, the Hamburg surgeon Helmut Schmidt (1895–1979) popularized Pitkin’s 20–22 gauge short bevel needle in Germany. This special needle, originally described by Georg Pitkin (1885–1943) of New Jersey in 1924, decreased the incidence of post-dural puncture headache (PDPH) to less than 5% [14].
With wider use of spinal anaesthesia in German speaking countries in the mid 1970s, the call for less traumatic spinal needles increased. This prompted the Würzburg anaesthetist, Günther Sprotte (1947), to develop a spinal needle, with a “pencil point” tip and aperture positioned slightly back from the tip. The design minimized trauma during perforation of the dura, further decreasing the incidence of PDPH to less than 2%. Since then the “Sprotte needle” has found world-wide acceptance among anaesthesiologists [15].
Unlike surgeons, obstetricians and gynaecologists persisted in advocating the use of spinal anaesthesia. After the London surgeon, Arthur Barker (1850–1916), described hyperbaric and hypobaric solutions in 1907, Freiburg obstetrician Carl Gauss (1875–1957; Fig. 29.3), assessed the use of gravity as revealed by experiments in Great Britain with a glass model of the spinal canal, evaluating the potential of hyperbaric/hypobaric solutions to control intrathecal spread [16]. Gauss recommended hyper- or hypobaric solutions in spinal anaesthesia for patients undergoing operative gynaecology. However, his technique did not become popular until the mid 1930s [17]. In 1900, Oskar Kreis (1872–1958) of Basle used spinal anaesthesia to ameliorate labour pain, describing the parturients as remarkably alert compared with women receiving other forms of labour analgesia [18]. Later, spinal anaesthesia was often combined with a low dose of subcutaneously administered scopolamine for sedation, as recommended by the Austrian obstetrician Richard von Steinbüchel (1865–1952) in 1903 [19]. It was hoped that the scopolamine would also decrease the incidence of vomiting.

Fig. 29.3
Carl Gauss gives a lecture at the University of Würzburg. Gauss used baricity to control the level of spinal anaesthesia. He contributed to the invention of twilight sleep. (The picture, taken around 1938, is from the collection of the author.)
Paravertebral and Epidural Conduction Anaesthesia
Most regional anaesthetic procedures designed to avoid the adverse effects of spinal anaesthesia were developed during the early 1900s. Tübingen obstetrician Hugo Sellheim (1871–1936), described paravertebral anaesthesia in 1908 [20], but surgeons did not become interested until Max Kappis (1881–1938), of Hanover, published articles on it [21]. Kappis suggested applying it to differentiate indistinct types of abdominal pain, a method approved by Läwen [22]. Läwen also advanced the use of epidural anaesthesia, particularly “sacral anaesthesia”, in urology and obstetrics [23,24]. The initially inferior quality of epidural anaesthesia stimulated Läwen’s efforts to improve the technique to one that allowed safe cholecystectomy, gastrectomy or nephrectomy [25]. To shorten the time of onset and to prolong the duration of anaesthesia, he used a new bicarbonated preparation of the local anaesthetic procaine [26]. He combined epidural and general anaesthesia in 1912 [27].
Safety First: Localization of Peripheral Nerves by Electricity
The increasing popularity of conduction anaesthesia in the twentieth century prompted development of techniques that located peripheral nerves using electrical stimulation. Georg Perthes (1869–1927) from Tübingen, described this method in 1912. Unfortunately his technique lay fallow until the 1960s, when it was rediscovered and became the “gold standard” until the twenty-first century when ultrasound became available for localization of peripheral nerves [28].
Quality Management in Regional Anaesthesia: Realized in 1910
In 1908, Bier described regional intravenous anaesthesia [29]. He injected up to 40 ml of 1% procaine intravenously into a limb previouly made bloodless by an Esmarch bandage. Complete anaesthesia and motor paralysis could be achieved. Known as “Venenanästhesie” in German speaking countries, and “Intravenous Regional Anaesthesia” (IVRA) or “Bier’s Block” in Anglo-American countries, the method achieved limited popularity. Fear of local anaesthetic overdose, or the cumbersomeness and limited duration of the block may have hindered its use [30]. IVRA also may not have competed with new conduction techniques for blocking peripheral nerves and plexuses percutaneously. Fear of intravenous overdose inspired Bier’s colleague Fritz Momburg (1870–1939) to invent a double tourniquet, still applied today when IVRA is used [31]. Concerns regarding the side effects of IVRA prompted the development of a remarkable risk/benefit questionnaire [32] marking the beginning of quality control measurements in German anaesthesia.
Pain Therapy
The pioneers of local anaesthesia appreciated the adverse effect of acute and chronic pain upon daily life, and evaluated the possible role of local anaesthetics in pain management. Surgeons Schleich, Braun, Läwen, Kappis and Kirschner explored various regional anaesthesia techniques in the management of chronic pain. A lesser known pioneer was the Berlin surgeon Walter Capelle (1881–1950), who in the early 1930s suggested continuous subcutaneous injection of local anaesthetic. Specially designed needles (Fig. 29.4) were inserted into the subcutaneous tissue of the abdominal wall surrounding the surgical incision. He hypothesized that pain relief would facilitate deep breathing and decrease the incidence of postoperative pneumonia [33]. His contemporaries did not appreciate the importance of this concept and it seems that only his surgical colleague Ewald Fulde (1899–1971) in 1933 praised Capelle’s innovative concept [34].
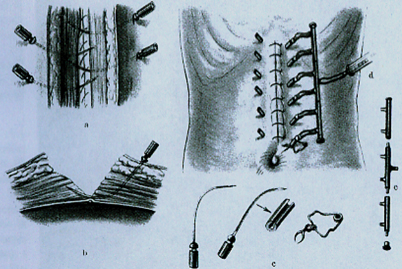
Fig. 29.4
This set of specially designed needles allowed the continuous application of local anaesthetics into the abdominal muscles for post-operative pain relief. (From Capelle W: Die Bedeutung des Wundschmerzes und seiner Ausschaltung bei Laparotomierten. Dtsch Zschr f Chir 1936; 246: 466–85.)
Tübingen surgeon Martin Kirschner (1881–1942), introduced the modern treatment of trigeminal neuralgia [35]. In 1932, he used an electrocoagulating current to produce discrete lesions and to limit the spread of substances injected into the trigeminal nerve and Gasserian ganglion. Kirschner inserted the electrode through the foramen ovale into the ganglion. Decades previously, Georg Perthes had used a similar apparatus to localize peripheral nerves, and perhaps this stimulated Kirschner to invent a comparable device [36].
The Long Way to Painless Childbirth: The Medicated Birth
In the early twentieth century, childbirth moved from the home to hospital. Progress in anaesthesia, and the introduction of new anaesthetics, led women and their obstetricians to expect a painless birth through medication. Unlike surgeons, obstetricians and gynaecologists applied spinal anaesthesia widely from its beginning. By 1900, Gauss had suggested the use of combinations of scopolamine and morphine to alleviate pain during childbirth. Although anaesthetic drugs affected the baby, physicians believed that the benefits of the combination outweighed the risks to mother and baby. Morphine relieved or dulled the pain, and scopolamine produced mental sedation and amnesia. There was the unproven perception that the drug combination enhanced the effectiveness of each single drug, thereby enabling a reduced dose of medication and a minimization of side effects. Labour might progress uninterruptedly without the pregnant woman being aware, or at least remembering, that she had suffered any discomfort. Gauss’ concept, known as “twilight sleep” attained transient popularity world-wide but its dangers to the baby and mother [37] rapidly led to its abandonment.
Later, caudal anaesthesia was recommended as a substitute for spinal anaesthesia. By the 1950s, epidural blocks, often performed via a catheter, became popular. This allowed more precise control over the extent of sensory loss and enabled the mother to assist in pushing during labour [38].
Early Intravenous Anaesthesia’Beginning with Intravenous Ether
Rectal and intravenous alternatives to the inhalation route were tried soon after the 1846 discovery of the anaesthetic properties of ether. In 1847, the Russian surgeon Nicolai Pirogoff (1810–1881) described such experiments in his monograph [39]. Decades later, French physiologist Cyprien Oré (1828–1899) attempted to popularize the intravenous injection of chloral hydrate, but failed due to inadequate analgesia and side-effects. Intravenous anaesthesia was forgotten for another thirty years, and rediscovered by the Würzburg surgeon Ludwig Burkhardt (1872–1922).
In 1909, Burkhardt reported that intravenous infusion of 4% chloroform or ether in a warmed saline solution could produce unresponsiveness and could sustain anaesthesia. He thought that intravenous infusion should minimize pulmonary complications because evidence of respiratory irritation such as coughing, laryngeal spasm, and cyanosis was markedly decreased. There were the added benefits of little or no excitement during induction, and intra- and postoperative cardiovascular stability, probably a consequence of the infusion of several litres of fluid. Burkhardt suggested that IV-ether was indicated for patients undergoing surgery of the head, face and neck, and especially for cachectic and hypovolemic patients [40]. Hamburg surgeon Hermann Kümmell (1852–1937) praised IV-anaesthesia as an “ideal narcosis” and recommended it for oesophageal surgery, gastric resection, craniotomy, and hypophysectomy. Intravenous ether was used during World War I, especially in hypovolemic patients [41].
But IV-ether never became popular. In the writer’s view, the technique died for two reasons: There was the problem of easily establishing reliable intravenous access; and few experienced persons knew how to use IV needles (i.e., to avoid the need for cut-down access). Nevertheless, until the late 1920s, notable German surgical journals and textbooks of surgery discussed the use of IV-ether, recommending it in selected cases and calling for further research. The introduction of the short acting barbiturates, cyclopropane, and intubation techniques, made IV ether superfluous by the early 1930s [42].
From Intravenous Ether Anaesthesia to Balanced Anaesthesia
In the early 1930s, oral barbiturates became widely used for premedication. Berlin chemist Emil Fischer (1852–1919) winner of the 1902 Nobel prize in chemistry in collaboration with Josef von Mering (1849–1908) synthesized barbitone (Veronal)®, the first effective sedative barbiturate, in 1903. In the mid 1920s, others reported on water soluble preparations of limited value due to unwanted pharmacological properties [43]. Their pharmacological properties caused a deep sleep lasting for up to 24 hours. Moreover, respiratory and circulatory side effects were noted and often the patient’s airway was compromised by the drug’s action, producing life-threatening situations [44]. In 1932, Bayer pharmacist Hellmuth Weese (1897–1954; Fig. 29.5) reported his experiences with a new, water-soluble and ultra-short acting barbiturate that changed anaesthetic practice, Evipan® (hexobarbital) [45].
Fig. 29.5
Hellmuth Weese invented hexobarbital in 1932, and the plasma substitute, 4% polyvinyl pyrrolidone in 1943. (The picture, taken around 1950, is from the collection of the author.)
The pharmacological properties of hexobarbital created a breakthrough despite untoward effects, including life-threatening cardiovascular depression, induced respiratory depression with airway obstruction, local phlebitis and allergic reactions. IV hexobarbital anaesthesia offered considerable advantages, particularly a smooth induction which was then followed with an inhalational anaesthetic. Unlike ether, hexobarbital did not burn or explode with the use of cautery. Its portability recommended its application in war zones, if administered with caution, and as often suggested, “with an individual dosage” [46]. Cumbersome anaesthesia apparatus could be eliminated. These advantages plus changing surgical requirements led to the broad acceptance of hexobarbital.
Weese, Professor of Pharmacology at Dusseldorf and Director of Pharmacology at Bayer Wuppertal-Elberfeldt, was a major contributor to modern intravenous anaesthesia, illustrating a beneficial partnership between academia and industry [47]. In 1938, he was elected as an honorary member of the International Anesthesia Research Society, and became one of the first honorary members of the German Anaesthesia Society (DGA) on its founding in 1953 [48]. In the later 1930s, thiopental displaced hexobarbital. The Munich scientist, Alfred Doenicke (born in 1928), reported on a new hypnotic, etomidate, [marketed as Hypnomidate®] synthesized in 1971 and introduced in 1973. Its minimal depression of the circulation facilitated anaesthesia in hemodynamically compromised patients [49].
On the Way to Target-Controlled-Infusion (TCI)
In the 1960s and 1970s, pharmacokinetics and pharmacodynamics with new available hypnotics and analgesics became a topic of scientific interest in Germany [50].
The onset and elimination characteristics of drugs administered via precision infusions pumps were analysed. These tests identified dosages of the drugs for used for “target controlled infusion” (TCI). The invention of microprocessor controlled infusion pumps facilitated development of TCI. A group of anaesthetists guided by Horst Stoeckel (1930) in Bonn published the first paper on “closed–loop total intravenous anaesthesia”, using the EEG as the feedback variable in estimating pharmacokinetic and pharmacodynamic values [51]. Of note, closed loop delivery of inhaled ether anesthesia had already been realized by the US physiologist Reginald Bickford (1913–1998) with his so-called Servo-Anesthesizer for the EEG-controlled dosing of ether in the early 1950s [52].
Rectal Anaesthesia
Pioneering anaesthesiologists found that rectal administration of pure ether produced excellent narcosis but adversely affected local tissues. The method was abandoned, but was revived early in the twentieth century by the American anaesthetist James Gwathmey (1862–1944) whose mixture of ether with olive oil produced satisfactory narcosis without injuring tissues [53]. It enjoyed some popularity in the US, especially for obstetric analgesia. In Germany it never became popular. Similarly, rectally administered paraldehyde was used as a basal narcotic in Great Britain, but was rarely given in German speaking countries.
Paraldehyde’s unpleasant odour, and the occasional violent restlessness associated with its use, caused German anaesthetists to prefer Avertin® (tri-bromoethanol), which became available in the mid 1920s. The surgeon Otto Butzengeiger (1885–1968) observed that convenience, a smooth induction, and ready acceptance by patients recommended the use of Avertin® [54], particularly where calmness during preparation for anaesthesia was desirable (e.g., in children and patients suffering from thyrotoxicosis). However, adverse local tissue reactions were described shortly after Avertin’s® introduction, leading to cautionary headlines in the lay-press and medical journals. With a revised dosage regimen, and administration restricted to selected patients, Avertin® remained in use until the middle of the 1960s.
Some Early Developments in Infusion Therapy
Experiences with IV anaesthetics stimulated the design of devices that administered precise volumes. In 1911, the pharmacologist Walter Straub (1874–1944; Fig. 29.6) produced the first electrically driven roller pump [55]. Straub suggested the use of his device to accurately infuse intravenous fluids, and drugs during anaesthesia, but only after the beginning of the 1950s were these pumps introduced into clinical practice. In German speaking countries, various models then became available, the most popular being the “Perfusor”®, designed by the Braun Company, Melsungen, in the early 1950s. (Fig. 29.7). Even today, the term “Perfusor”® is colloquial for an anaesthesia IV pump in German speaking regions, even if it is a microprocessor-controlled computerized model [56].

Fig. 29.6
Walter Straub (center and with cigar) produced the electrical roller pump for accurate infusion of liquids. Weese is third from left. (The picture, taken around 1930, is from the collection of the author.)
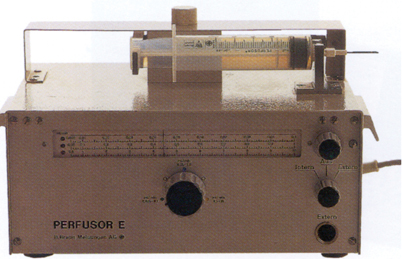
Fig. 29.7
An early model of Braun’s infusion pump, named “Perfusor”, used in clinical practice around 1955. (From the collection of the author.)
Synonymous with the use of an intravenous infusion needle is the term “Strauss-Kanüle”, a needle made of steel and invented in the first decade of the twentieth century by the Berlin internist Strauss (1868–1944) [57]. A comparable model, made of polypropylene, became available in the mid 1950s. It was produced by the Braun Company, Melsungen, hence it is usually named “Braunüle”® [58].
The first appearance (in 1911) of today’s ubiquitous drip-chamber may be credited to the Cologne surgeon Emil Martin (1865-?) [59].
From Short-Acting Salt-Solutions to Volume Expanding Fluids
Early in the twentieth century, the importance of a sufficient intravascular fluid volume during anaesthesia became increasingly appreciated. Attempts were made to retain infused solutions within the intravascular space longer than normal saline by using a solution of gum acacia [60]. The research of the English physiologist Ernest Starling (1866–1927), suggested that a 3% solution might be best. His concept was correct, as shown by tests during World War I in wounded soldiers. But serious adverse effects such as allergic reactions, fever and even shock, led to tests of new approaches, such as the administration of hypertonic solutions [61]. Surgeon Friedrich Hercher (1881–1958) may have been the first to use such hypertonic solutions, giving them during World War I. He administered a “maximum of 50 ml of a 9% hypertonic solution” and praised its immediate cardiovascular stabilizing effects in several publications. Berlin surgeons Franz Schück (1888–1958) and Erich Simenauer (1901–1988) revived this concept in the 1930s. Schück noted the positive circulatory effects that appeared in 3–5 minutes. Why this revolutionary concept did not change clinical practice is unclear. One explanation is that both scientists were Jewish and emigrated to escape persecution. Their idea was temporarily forgotten, and rediscovered in the early 1980s. Today their concept is known world-wide as “small-volume resuscitation” [62].
A world-wide search for a solution with volume expanding properties proceeded in parallel to the studies of a concentrated saline or sugar solution. The lack of safe and effective blood-volume expanders became apparent during World War II. In Germany, Weese devised a non toxic, biocompatible solution with the desired blood-volume expanding properties, but without side-effects in 1943. This was Periston® (Polyvidone) [63], containing 4% polyvinyl pyrrolidone (PVP) with an average molecular weight of 30,000. It was successfully tested as a plasma substitute in wounded soldiers, primarily during the campaign in France in 1940. Later it was not uncommon to administer Periston® into the sternal marrow of hypovolemic soldiers to manage hemodynamic instability. However it was generally infused intravenously during surgical procedures in anaesthetized patients. It was noticed that the pyrrolidone could bind with toxic substances like botulism and diphtheria toxins that were then renally excreted, thus being detoxified. Bayer subsequently developed a 6% preparation for this use, and this preparation was used to treat intoxication-hazards, such as barbiturate poisoning in suicide or in septic patients [64]. In the mid 1960s, pyrrolidone was withdrawn from the market, as better new synthetic colloids became available, especially modified fluid gelatins, dextrans and new preparations of starch solutions [65].
Around 1920, Straub developed an infusion of a “serum saline solution”. Its use became widespread, since it could be prepared from hot water and a powder. A “Normosal-solution”, manufactured at the “Sächsische Serum Werke” was available in ampoules by the middle of the 1920s. Some years later, other saline solutions, such as Tutofusin became available
Professional Developments in Surgical Pain Relief in Germany
Schleich’s call to raise the quality of anaesthesia practice in the early part of the twentieth century fell on deaf ears. However the introduction of acetylene as an anaesthetic, the greater use of nitrous oxide, and the increased administration of intravenous or rectal anaesthetics in German speaking countries in the early 1920s, revived the idea of a specialty of anaesthesia. The development of complex apparatus for anaesthetic delivery, and more intricate operations increased the pressure for specialization. Physicians and state institutions favoured specialization, and the founding of a German Anaesthesia Society was discussed during the ninetieth Meeting of the German Natural Scientists and Physicians in Hamburg in 1928. But influential surgeons rejected the idea of anaesthesiologists. Most surgeons feared losing their place as the “captain of the ship” in the operating theatre. There was also an economic reason. Accepting the anaesthesiologist’s important role in the treatment of patients during surgery would result in monetary requests to the patient, and this was not acceptable! In a popular textbook, Greifswald surgeon Friedrich Pels-Leusden (1866–1944) argued: “Fortunately, we do not have specialists in anaesthesiology like in the United States and hopefully they will never annoy us”. Thus for decades, nurses experienced in the administration of anaesthetics were responsible for anaesthesia [66].
The enormous progress in anaesthesia in the US and UK during the 1930s and 1940s, rekindled discussion after World War II. But major surgical circles continued to deny the need for specialization in anaesthesiology. Karl-Heinrich Bauer (1890–1978) argued: “For the training of anaesthesia physicians there is no urgent need; on the contrary, a better training of the anaesthesia nurses is more urgent” [67]. But the development of anaesthesiology as an independent branch of medicine could no longer be stopped. In 1953, the German Society of Anaesthesia (Deutsche Gesellschaft für Anaesthesie) was founded [68].
Because in Germany there was no educational program for nurses to specialize in anaesthesia, their role diminished as the medical specialty developed [69]. For decades, nurses have not been allowed to perform anaesthesia unless controlled (directed) by a physician [70]. In contrast to this situation in Germany and Austria, trained nurses in Switzerland are permitted to perform anaesthesia when an anaesthesiologist is nearby.
Journals and Textbooks Reflect the Increasing Importance of Anaesthesia
Publication of the first German anaesthesia-related journals “Der Schmerz” and “Narkose und Anaesthesie” in 1928, considerably preceded the founding of a professional specialty of anaesthesia. These journals merged to “Schmerz, Narkose und Anaesthesie” for economic reasons in 1929 and continued publication until 1944, interrupted then by the devastation of World War II. In the early 1950s, discussion by those working to form the German Anaesthesia Society led to publication of the journal “Der Anesthesist”. Indeed, the first issue of “Der Anesthesist” appeared in 1952 when the Austrian and Swiss Societies were founded. It is noteworthy, that this happened before the founding of the German Society of Anaesthesia! Der Anesthesist subsequently became the official organ of the German, Swiss and Austrian Anaesthesia Societies. In the mid 1960s, additional anaesthesia related journals appeared: Anästhesiologie und Intensivmedizin (Anaesthesiology and Intensive Medicine), Anästhesiologie-Intensivmedizin-Notfallmedizin-Schmerztherapie (AINS; Anaesthesiology, Intensive Care Medicine, Emergency Medicine, Pain Therapy) and these are still published [71]. The official journal of the German Society and Intensive Therapy of the former German Democratic Republic (DDR) merged with AINS after West and East Germany reunified in the late 1990s. Presently, all publications are official organs of the German Anaesthesia Society [72].
An increasing demand for information concerning anaesthesia encouraged publication of new textbooks for both the novice and the experienced anaesthetist. In the first decade of the twentieth century, German speaking authors Fritz Dumont (1854–1932) from Bern, Switzerland, Benno-Wilhelm Müller (1873–1947) from Berlin, and Max von Brunn (1875–1924) from Tübingen published anaesthesia related monographs. Dumont’s textbook, “Handbuch der der allgemeinen und lokalen Anästhesie” [Textbook of general and local anaesthesia] appeared in 1903, Müller’s monograph “Narkologie’Narkosen und Methoden der lokalen Anaesthesie” [General anaesthesia and methods of local anaesthesia] followed in 1908. Max von Brunn’s monograph “Allgemeinnarkose” [General Anaesthesia] became available in 1913. In 1934, two monographs were published: Hans Killian’s “Narkose für operative Zwecke” (General Anaesthesia for Operative Surgery) [73] and Ludwig Lendle’s, Fritz Hesse’s and Rudolf Schoen’s “Allgemeinnarkose und örtliche Betäubung” (General Anaesthesia and Local Anaesthesia) [74].
Related posts:
 History Reflected in the Evolving Approaches to Anesthesia for a Patient Undergoing Cholecystectomy
A History of Intravenous Anesthesia
History Reflected in the Evolving Approaches to Anesthesia for a Patient Undergoing Cholecystectomy
A History of Intravenous Anesthesia
 Major Anesthesia-Related Events in the 2000s and Beyond
Major Anesthesia-Related Events in the 2000s and Beyond
 1846–1860: Following the Discovery of Anesthesia
1846–1860: Following the Discovery of Anesthesia
 Major Anesthetic Themes in the 1960s
Major Anesthetic Themes in the 1960s
 A History of Intensive Care Medicine
A History of Intensive Care Medicine
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


