Chapter 4 The analysis of movement
Movement analysis can be as daunting as it is complex, three-dimensional, always changing, and numerous aspects contribute towards functional control. Some basic underlying concepts are examined.
Basic concepts in posturomovement analysis
Kinematics
Kinematics describes motion in the body,1 without regard for the forces or torques that may produce the motion.2 Kinematic patterns of movement involve the alignment and relative contribution of various segments of the body in an action.
Kinetics
Kinetics describes the effect of forces upon the body.2 Movement concerns the way we organize ourselves in relation to numerous forces, the most dominant and consistent of which is gravity. This deserves some consideration.
Centre of gravity
The COG of the body in the anatomical upright position is considered to be at the level of the 2(nd) sacral vertebra, inside the pelvis.1,3,4 However, the anatomical position does not necessarily equate to movement function because as soon as the configuration of the body segments changes so does the COG. Each segment of the body has its own COG. If two or more adjacent segments are going to move together as a single solid segment they can be represented by a single COG.1 The COG can be raised for example when reaching up, or lowered if the legs or body bend, etc. Depending on the arrangement of the body segments it can be located at the edge of or outside the body. The LOG passes through the COG (Fig. 4.1).
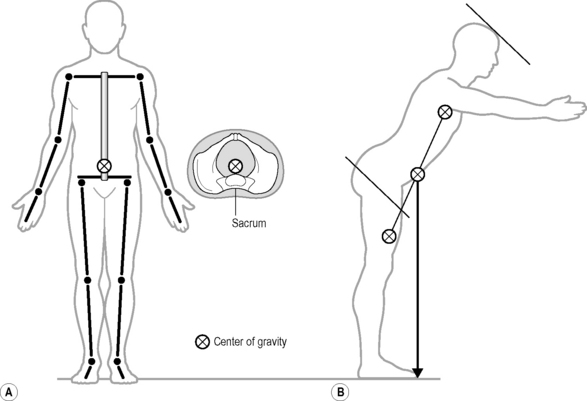
Fig 4.1 • The centre of gravity is mainly located within the body (A) but can deviate outside the body (B).
The interaction between the LOG and the COG is in a constantly changing relationship in movement. In fact movement can be simply seen as shifting ones COG around with respect to the LOG. The body is most stable when segmental or global alignment is closer to the LOG and the COG is low and most vulnerable to instability when the body configuration moves outside the LOG and/or the COG is high. The neuromyofascial articular system anticipates and responds to the continual gravity induced sensory cues in order that we do not collapse or fall over.
Centre of pressure
This is the point of application of the ground reaction force through the base of support. This force reflects Newton’s third law of action/reaction in that the force exerted by the body onto the ground is reflected back at the centre of pressure.4 Pressure down into the ground stimulates a neuromuscular response of ‘push up and lift’. This force is utilized a lot as we develop and maintain movement control against gravity. It may be exerted through any part of the body – the hands, feet, knees, ischia or even the head, as is the case when standing on the head! (See Ch.13).
Planes of motion
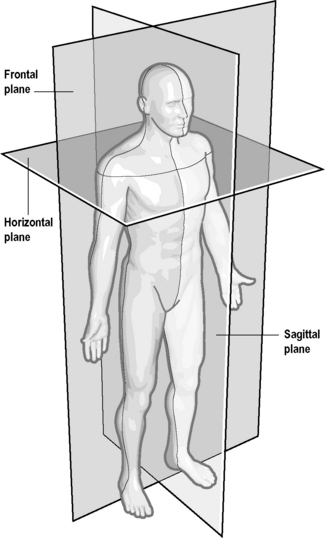
Posture and movement are generally analyzed and described in relation to the three cardinal planes. These planes of reference are derived from dimensions in space and are at right angles to each other. They are depicted in the context of the person standing in the anatomic position as illustrated and are carried over into other postures as the person moves (Fig. 4.2).
Posture
The term ‘posture’ is used to describe both biomechanical alignment of the segments of the body, as well as the orientation of the body to the environment.5
Commonly posture is thought of as alignment of the body in the upright sitting and standing positions. However, each and any position adopted is ‘a posture’. The posture adopted in any position is a reflection of the neuromuscular status of the person, and this is evident from birth through to adulthood (see Ch. 3).
‘Static’ posture
Gracovetsky6 describes posture as ‘an average’– the steady erect stance is maintained by cycling through a sequence of different but closely related postures. This oscillation is necessary from a sensory perspective and to prevent continuous loading of the viscoelastic tissues.
Sagittal view
Optimum alignment of the segments and easy equilibrium is said to occur when the LOG passes through:
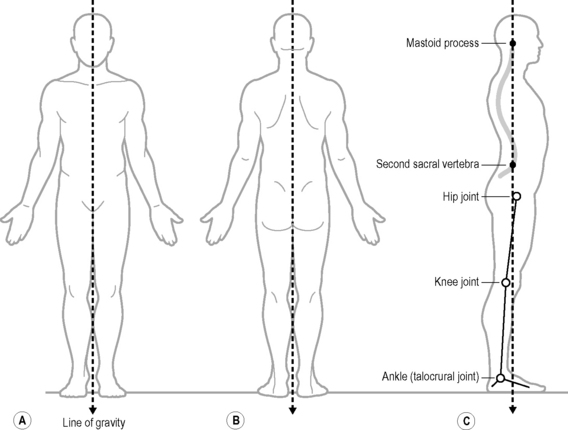
Optimal alignment of the vertebral column is also said to occur when the LOG passes through the transitional or junctional regions of the spine.7 Many consider that the T12/L1 articulation is quite central8,9 being the point of inflection between the thoracic kyphosis and lumbar lordosis.7 Ideal alignment is said to produce a torque that helps maintain the optimum shape of each spinal curve with the maximum torque at the convexity of each curve. When the line of gravity falls posterior there is an increased axial extensor torque; when it falls anterior there is an increased flexor torque.2
In the pelvis, ‘ideally’ the LOG passes through the greater trochanter yet posterior to the axis of the hip joint1 but anterior to the sacroiliac joints.9 This tends to nutate the sacrum while also creating an extensor moment at the hip and a tendency to passive posterior rotation of the pelvis.
Coronal view
The LOG passes directly through the centre of the head, trunk and pelvis and falls midway between the two feet. This conceptually divides the body into two symmetrical, equal halves (Fig. 4.3).
This view is useful for discerning lateral deviations and asymmetries in the body.
There is a constant though subtle postural sway in response to breathing10 which provides continual sensory cues which keep refuelling the alignment of the segments and the antigravity response. Flexible and adaptable segmental control throughout the spine allows appropriate postural shifts and sets to balance and support movement.
Farhi11 points to the observable close relationship between how we stand and breathe. Three patterns are generally apparent:
Dynamic posture
In functional terms posture is always dynamic as it is constantly changing and adapting to support movement. However, when walking, running, jumping, throwing and lifting1 there is the increased challenge of adapting to further changed alignment of the segments, momentum and larger perturbations.
Quantitative and qualitative aspects of movement
Effective clinical practice relies upon the ability of the practitioner to analyze movement in the clinic in a relatively easy, practically relevant, and useful way. Trew4 states ‘it is relatively straight forward to measure some of the physical aspects of movement such as joint range or muscle strength in a non functional context but difficulty arises when the quality of the movement must also be considered’.
The skilled practitioner is one who has the ability to see the qualitative ‘soft signs’ as well as the ‘hard signs’ of objectively measurable movement. Janda considered that the quality of the motor performance was of greater importance than testing strength.15
The qualitative aspects of movement are observable
While the quantitative aspects of movement function are more derived from testing, the qualitative aspects are derived more through observation of the patterns of motor response in different situations. We are interested in the quality of a person’s sensory–motor integration. Without any interference we note how he habitually chooses to stand, sit, bend over and perform some of the repetitive actions involved in daily living such as getting undressed or standing on one leg. Feldenkrais apparently coined the term ‘acture’ – posture in action, to describe the observation of the person moving.12 This can reveal a wealth of information such as the presence of organic or pathological movement patterns, discomfort during motion, the emotion behind the motion, the amount of sensory amnesia present, the range of motion, the quality of the breathing pattern and the quality of specific tasks as in the transitions between lying, sitting standing and walking. We may decide to ‘test’ by observing the manner in which the patient spontaneously chooses to perform a requested task
Doing it – but ‘how’ the movement happens: aspects of quality control in posturomovement
The following aspects are functionally interrelated in varying respects.
Observing the size, shape and symmetry of the superficial muscles tells a story
Janda13 maintained that ‘changes in muscle function play an important role in the pathogenesis of many painful conditions of the motor system and constitute an integral part of postural defects in general’. The muscles both cause and reflect altered function.14
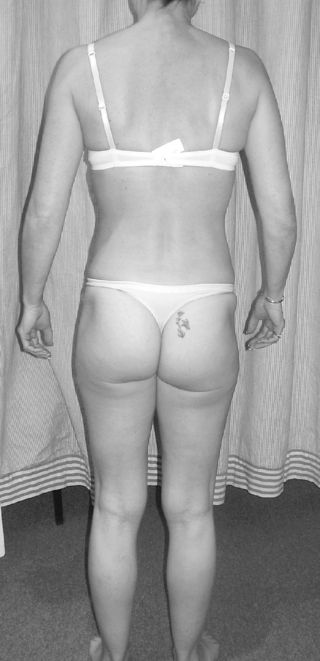
Simply observing the appearance of the standing person’s superficial muscles can provide insights about the patient’s neuromuscular function.15 The size shape and symmetry of a muscle provides clues to the level of its activity. Those muscles which are used a lot become bulkier and more prominent (Fig. 4.4) and those that aren’t lose their definition or shape. The role of the deeper muscles in postural deviations may need to be confirmed or negated in later tests (Ch.13).
The ability to align the body segments in different functional acts
As infants we spent a deal of time down on the ground as we learned how to move along and get ourselves up against the force of gravity. As adults, we tend to spend most of our time upright in one way or another and our patterns of motor use represent a fairly constrained repertoire by comparison. Commonly, most of us use four basic spinopelvic posturomotor patterns and derivatives of them in the course of our daily living – standing, walking, sitting and bending/lifting/squatting.
The importance of this ‘functional control’ in everyday activities has also been recognized by McGill who has examined motion patterns of lifting16 and O’Sullivan who has examined postural patterns of sitting in non back pain and back pain groups.17,18
The ability to generate appropriate patterns of axial stabilisation
All muscles contributing to the ‘central stabilisation system’ are interdependent in function. If one muscle is weak or overactive, this never remains isolated, but affects the static and dynamic function of the entire spine. Individual spinal segments will no longer be controlled in a balanced way. In particular, the diaphragm needs to become integrated into the patterns of central control.19 Observing the quality of the breathing pattern and axial alignment at rest and during trunk and limb movements tells us a lot about the quality of axial control. Poor patterns of axial make balanced alignment difficult (Fig. 4.5).

Limb load tests e.g. the active straight leg raise test
The supine active straight leg raise test (ASLR) is a functional test which assesses the quality of the patterns of axial stabilization when the extended leg is lifted off the surface. First described by Mens et al.,20 the extended leg should be able to effortlessly lift 5 cm. When control is optimal, three dimensional alignment of the pelvis21 should be maintained as well as the alignment of the whole torso while breathing patterns are maintained.22,23 The test as originally described, is positive if accompanied by a primary sensation of profound heaviness in the leg and /or pain23 which is relieved by the application of bilateral compression through the ilia either just below the anterior superior iliac spines or at the level of the symphysis pubis20 (above or below the hip joint). This compression is considered to enhance ‘force closure’ through the sacroiliac joint21 by simulating muscle forces which would otherwise control the movement. The prone ASLR test similarly tests axial patterns of control including the breathing mechanism with hip extension in knee extension.
Because of the long lever arm of the leg, it represents a fairly high level challenge to the ability and quality of axial stability. While a positive test result has been shown to strongly correlate in people with pelvic ring instability,20 a positive test does not necessarily confer sacroiliac joint instability. However, a positive test is indicative of suboptimal neuromuscular control in the torso and pelvic–hip complex. Subjective complaints should not be the only decider of dysfunction as probably more important is the observed quality of the axial control patterns. Dysfunctional responses include loss of alignment, breath holding, central ‘fixing’ strategies and a functional ‘disconnect’ between the upper and lower torso. There are numerous other tests using either a short or long limb lever which can be applied in a similar manner in order to test and facilitate axial control strategies.
Sequence and degree of muscle activation in a movement
Movement stems from a starting point – a ‘posture’ developed on a base of support which is actively controlled before the actual movement happens. The work of Hodges24,25 has shown that normally transversus abdominis is active before arm movement begins. Transversus is a member of the ‘central stabilization system’ – a coordinated trunk muscle synergy creating anticipatory postural adjustment to support limb movement.
Janda15 maintained that examination of movement patterns provides a good indication of the quality of a person’s motor control. In the presence of muscle imbalance or poor central nervous system regulation some typical abnormal patterns of muscle activation can be clinically observed. He described six basic movement patterns15,26–28 which essentially test the quality of axial patterns of control.
These are fully described elsewhere.28 When changed, these usually show certain typical patterns of response. Appreciating the common features of dysfunction (Ch. 8) and clinical sub-classification helps predict the response (Chs 9 & 10).









