Team Activation and Organization
William S. Hoff
I. The Trauma Response
The response to an injured patient arriving at a health care institution is determined by (1) the manner in which the patient is triaged in the prehospital phase and (2) the type of facility to which the patient is being transported.
Institutional capability. The resources available to manage trauma patients are institution-specific. The American College of Surgeons Committee on Trauma has designated trauma centers as follows:
Level I. Provides a 24-hour, in-house trauma team with the ability to fully resuscitate injured patients and provide definitive surgical care for the most complex injuries. The trauma team is usually led by an attending trauma surgeon, emergency physician or senior-level surgical resident. Level I centers are typically located in population-dense areas. Level I trauma centers also distinguish themselves through research, training, and prevention and outreach programs.
Level II. Clinical capabilities are similar to Level I centers. However, more specialized resources (e.g., cardiac surgery, microvascular surgery) are not required. An in-house trauma surgeon is not required, but must be available to meet the patient on arrival. Level II centers are frequently located in suburban areas.
Level III. These centers typically serve rural areas not easily accessible to Level I or II trauma centers. A surgeon must be available in a timely fashion, but certain subspecialties (e.g., neurosurgery) are not required. Complex patients are routinely transferred to level I or II trauma centers.
Level IV. Provide initial evaluation and assessment of injured patients; typically located in small hospitals or clinics serving the more remote areas. Surgical coverage is not mandatory and most patients will require transfer to higher levels of care.
Non-designated. The majority of hospitals in the United States carry no specific trauma center designation. Each hospital should be aware of the resources available for management of trauma patients with clearly delineated plans for transfer of patients that exceed the “resource threshold.”
Levels of response. All hospitals should have some established response to injured patients. In non-designated hospitals, where a full trauma team is not available, an organized procedure (e.g., personnel, tasks, etc.) will facilitate resuscitation and optimize patient outcome. Trauma centers use pre-determined tiered levels of response based on regionally established triage criteria. The composition of the trauma team varies based on the level of trauma response:
Full response (e.g., “trauma code,” “code red”). Highest level of response designed for patients with physiologic instability, severe traumatic brain injury or who present with obvious life-threatening injuries (e.g., abdominal gunshot wound).
Modified response (e.g., “level II trauma,” “trauma alert”). Response typically intended for physiologically stable and neurologically normal patients with the potential for serious injury based on injury mechanism or anatomic findings. Composition of the trauma team will vary with the trauma center; emergency medicine physicians frequently assume the leadership role.
Trauma consultation. In most trauma centers, this response is reserved for low-energy or single system injuries in stable patients. Patients are fully evaluated by an emergency medicine physician prior to consultation with a trauma surgeon.
II. Trauma Resuscitation Area
Physical plant
A dedicated trauma resuscitation area (TRA) is required for any Level I or II trauma center and should be considered in any hospital emergency department that receives a significant volume of injured patients or where an injured patient may arrive without prior notification.
The TRA should be secure, with limited access to non-medical personnel.
Convenient access to the operating room, radiology suite, intensive care unit, and staff call rooms are other important considerations in TRA design.
The TRA must be sufficiently large to accommodate all members of the trauma team (i.e., 5 to 10 people). Ample space must be provided to allow free movement of prehospital providers into and out of the area, complete resuscitation, basic radiographic evaluation, orthopedic stabilization, and required emergency surgical procedures:
Airway intubation
Cricothyroidotomy
Insertion of central venous catheters
Tube thoracostomy
Placement of urinary catheters and naso/orogastric tubes
Emergency department thoracotomy
Focused abdominal sonography for trauma (FAST)
Diagnostic peritoneal lavage (DPL)
Splinting of fractures
Wound irrigation and suturing
Other TRA considerations include:
Lighting should be sufficient and must allow free access to the patient and easy movement of personnel and equipment through the workspace.
Hypothermia must be actively prevented during trauma resuscitation. Specific measures to prevent hypothermia include individual TRA thermostats and overhead heat lamps.
A mechanism should exist to supply the TRA with uncrossmatched packed red blood cells (O-neg), especially for hospitals in which the blood bank is located a significant distance from the emergency department. Ideally, the laboratory or blood bank, as part of the trauma response, can deliver O-neg blood in a cooler to the TRA. Level I and II trauma centers should have a massive transfusion plan designed to supply large volumes of packed red blood cells, thawed plasma and platelets.
Each institution must have guidelines for resuscitation of multiple trauma patients within the confines of the defined TRA or emergency department. A pre-determined plan for temporary expansion into alternate patient care areas is essential to optimal mass casualty triage and disaster management. A plan for mobilization of additional personnel should also be established.
Protective garments
Any bodily fluid should be considered a potential source of transmissible disease and, thus, barrier precautions should be mandated for all members of the trauma team. Specifically, non-sterile gloves, an impervious gown, surgical mask, protective eyewear, and shoe covers are required for all team members likely to come in contact with a patient.
It is not uncommon for radiographic studies to be performed concomitant with the trauma resuscitation. Appropriate protective gear (e.g., lead vests, lead aprons) should be worn by trauma team members who may be working close to the patient while radiographs are being performed. Having these garments available obviates the need to interrupt the resuscitation during x-rays.
Protective garments should be available in a designated area adjacent to the TRA in full view of those who may enter the area. The trauma team leader or recorder should monitor and enforce compliance with barrier precautions and radiographic protective gear.
Inevitably, patients will arrive without notification. In these cases, guidelines should be developed for relieving personnel who, by necessity, have entered the TRA without barrier precautions. Protected team members should provide rapid relief for those who have not had the opportunity to don protective equipment. The ultimate goal is to minimize the total number of unprotected individuals during a given resuscitation.
Appropriate and visible receptacles available for disposal of used protective gear must be available within the confines of the TRA. Personnel should be discouraged from leaving the TRA with soiled gown, gloves, etc.
Equipment. The minimal amount of equipment and supplies necessary to effectively resuscitate should be stored in the TRA. While frequent restocking may be necessary, eliminating superfluous inventory optimizes resuscitation space and facilitates standardization of care.
Carts or trays may be utilized to store the most frequently used equipment (e.g., airway cart, thoracotomy tray). Equipment trays should contain only those instruments and materials absolutely necessary to perform a given procedure. Trays should be easily accessible, openly displayed, and clearly labeled for easy identification. One logical approach is to stock supplies in a head-to-toe configuration, with airway equipment and cervical collars stored near the head of the stretcher, thoracostomy trays near the midportion of the stretcher, and splinting materials near the foot of the stretcher.
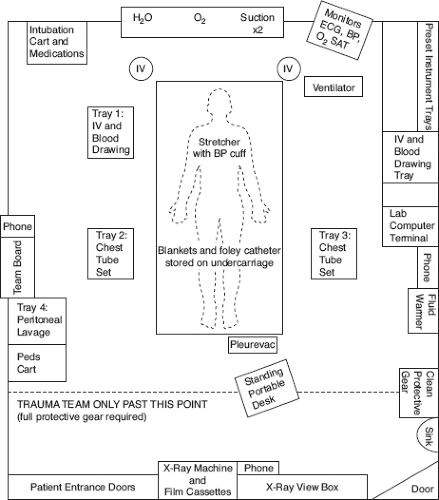
Figure 10-1. Layout of the TRA.
Table 10-1 Immediately Accessible Equipment and Supplies
Head of stretcher Equipment for airway management, including multiple endotracheal tubes, oxygen, suction devices, oral/nasal airways, Ambu bags, and laryngoscopes
Tray #1 Equipment for intravenous access, intravenous tubing, phlebotomy, arterial blood gases
Trays #2 and #3 Thoracostomy trays, chest tubes (36 F, 40 F), appropriate suture material
Tray #4a Diagnostic peritoneal lavage equipment
Foot of stretcher Chest drainage system (e.g., Pleurovac)
Left side Manual blood pressure cuff, electrocardiogram wires, pulse oximetry monitor
aUltrasound machine.
Equipment necessary to manage immediately life-threatening conditions should be stocked close to the stretcher, in proximity to the trauma member most likely to use it (Table 10-1; Fig. 10-1).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree






