Chapter 36 Structure of the Respiratory System
Lower Respiratory Tract
Lower Respiratory System
Lungs
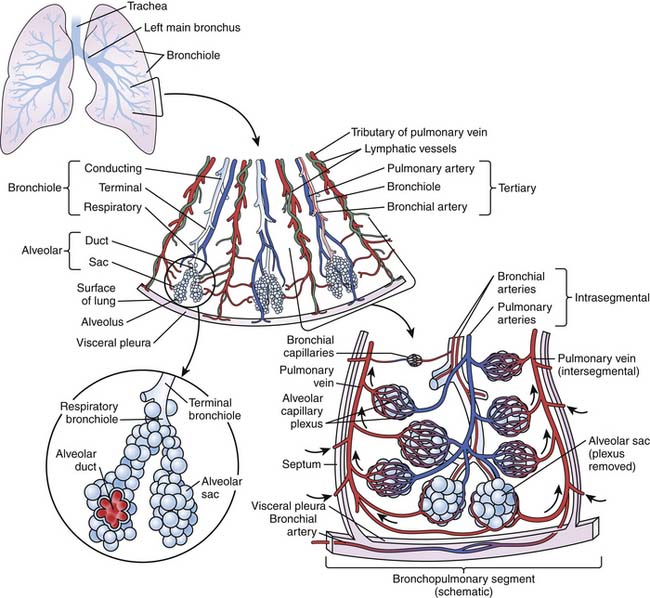
Lung weights of children from birth to age 12 years have been published.1–13 At birth, the lungs weigh about 40 g and double in weight by 6 months. Mature respiratory alveoli appear at approximately 36 weeks of gestation and continue to develop until about 2 years of age. By age 2 years, when most of the alveolarization process is completed, total lung weight is approximately 170 g. In the normal adult, the lungs weigh approximately 1000 g.9 Lung volume increases from about 250 mL at birth to 6000 mL in the adult. The height of a normal adult lung is 27 cm at total lung capacity, but in the range of normal breathing it is approximately 24 cm in height. Externally, the lungs are paired structures that, with the mediastinum, fill the thoracic cavity. Normally the right lung is comprised of three lobes and the left lung consists of two lobes and the lingula, which arises from the left upper lobe. The lobes are separated by fissures and have hili that receive a primary lobar bronchus, pulmonary artery and veins, bronchial arteries and veins, lymphatics, and nerves (Figure 36-1).14 The lobes are further subdivided into 19 bronchopulmonary segments that receive a primary segmental bronchi and a tertiary pulmonary artery branch and are drained by pulmonary veins. The pulmonary veins do not course with the airway and pulmonary artery dyad; instead, they course midway between the dyads and can be readily identified in the septa that run within the intersegmental septa. The connective tissue septa that demarcate each bronchopulmonary segment define the smallest surgically resectable portions of the lung.
Airways and Bronchus-Associated Lymphoid Tissue
The airway branching pattern in the lung undergoes multiple generations, yielding a total of 27 or 28 divisions when counting begins from the primary bronchus. The bronchi are the larger intrinsic cartilaginous airways and comprise nine to 12 generations starting with the primary bronchus and terminating in bronchi having a diameter of approximately 1 mm. Bronchioles, sometimes called membranous bronchioles or distal noncartilaginous airways, are the last of the conducting system. They comprise an additional 12 generations before ending as terminal bronchioles, the last purely conducting structure in the lung. Horsfield4 showed that the course from the trachea to the alveolar level may be as few as eight or as many as 24 airway branch points. This finding points out that a particular airway diameter may occur at various points along the distribution of the bronchial wall. Determination of the total cross section of airways is important in understanding the distribution of airway resistance. Weibel12 showed that as the peripheral generations of the airways are approached, the total cross-sectional area of the lung is markedly increased, suggesting that peripheral airways account for only a small proportion of total airway resistance. In the adult, the asymmetrical dichotomous branching pattern results with each daughter branch decreasing an average of 0.75% of its parent branch, but an increase results from the combined cross-sectional area of the two daughter branches. It is well known, however, that peripheral airway resistance in children’s lungs is disproportionately high. The size of the conducting airways is related to stature, so the airways’ cross-sectional area in children increases at a slow rate with growth and aging. Because the peripheral airways make up a significant portion of the total respiratory resistance in children, disease in the bronchioles can be serious.
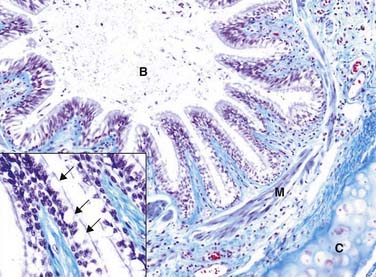
The bronchi maintain the histologic appearance of the trachea in that a mucosa, submucosa, muscularis, adventitia, and cartilaginous support are present. As the bronchi branch deeper into the lung parenchyma, the cartilage rings become plates and less regular, and the muscularis becomes continuous, being located between the submucosa and the cartilage plates. Also contained within the bronchial submucosa are mucus-secreting submucosal glands, nerves, ganglia, and bronchial arterial branches (Figure 36-2). As the bronchi decrease in diameter, the pseudostratified columnar epithelium becomes lower and the mucoserous glands become fewer in number. Although the glands wane in number in the more distal parts of the lung, mucous cells persist and can be found in very small bronchi and in some of the membranous bronchioles.
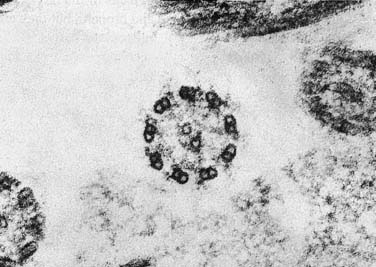
The bronchial mucosa contains several epithelial cell types: ciliated, mucus producing (goblet cells), basal, brush, and neuroendocrine. The ciliated cell constitutes more than 90% of the epithelial cell population in the conducting airways, but the proportion and number of cilia per cell decrease from the proximal to distal airways. The 9+2 microtubular structure within the cilia has been shown to be altered in the primary ciliary syndromes (Figure 36-3). In addition to its ciliary beating movement, the ciliated columnar cells regulate the depth of the composition of the periciliary fluid and transport ions across the epithelium. The basal cell has a progenitor cell role and also functions to maintain adherence of columnar cells to the basement membrane. The brush cell, thought to have a role in fluid absorption and/or chemoreceptor function, is found rarely in the tracheobronchial and alveolar epithelia.
Bronchus-associated lymphoid tissue (BALT) appears as isolated nodules in the connective tissue of the lamina propria of the bronchial tree and produces primarily IgG and secretory IgA. Collections of BALT cells tend to occur at airway bifurcations and are covered by a special epithelium that can undergo pinocytosis and transport solutes and particulate antigens. BALT is sparse at birth but starts accumulating thereafter. It is prominent in lungs of children and in diseased lungs of smokers and patients with bronchiectasis. Although more than 50% of the cells are B lymphocytes, T lymphocytes also are found (18%), along with follicular dendritic cells.15 Sometimes these nodules bulge into the bronchial lumen. Additional lymphoid tissue in the lung is a rich supply of lymph nodes within the lung, at the carina, and along the trachea.
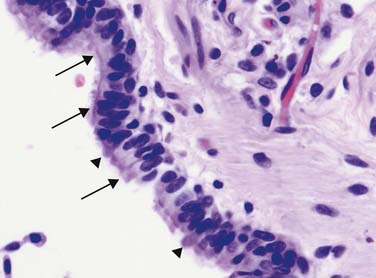
Although originally defined as having a lumen diameter less than 2 mm, the term “small airway” usually refers to a bronchiole. Histologically, the bronchiole is characterized by a transition from pseudostratified tall columnar epithelium to a more cuboidal ciliated form. In addition, the mucous goblet cell is replaced by the nonciliated Clara cell (Figures 36-4 and 36-5). In the bronchiolar epithelium, a ratio of about three ciliated cells to two nonciliated cells lines the lower airways. The Clara cell is identified as a dome- or tongue-shaped cell that protrudes into the bronchiolar lumen among the shorter ciliated cells. The Clara cell has varying features according to species but possesses an abundance of agranular reticulum and secretory granules. Clara cells synthesize and secrete Clara cell secretory protein (CC10, CC16), a unique 10-kDa protein similar to rabbit uteroglobin that has antiinflammatory and immunoregulatory functions.16 In addition, Clara cells secrete surfactant-associated proteins A, B, and D. Importantly, the Clara cell also functions as a progenitor cell that differentiates into ciliated cells following injury, and some investigators have shown that the Clara cell can differentiate into a type II epithelial cell.17
< div class='tao-gold-member'>






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


