164 Sodium and Water Balance
 Key Points
Key Points• Most signs and symptoms of clinically significant hyponatremia are related to an increase in cellular volume in the central nervous system and subsequent cerebral edema.
• Hyposmolar hypovolemic hyponatremia, the most common type of hyponatremia encountered in the emergency department, is seen in patients with severe total body water depletion in excess of sodium loss.
• Diagnostic criteria for the syndrome of inappropriate secretion of antidiuretic hormone (ADH) include hyposmolar hyponatremia, inappropriately concentrated urine, and exclusion of other causes of hyposmolar euvolemic hyponatremia such as hypothyroidism and adrenal insufficiency.
• Hypovolemic hypernatremia, the most common cause seen in the emergency department, results from severe total body water depletion.
• Patients with central diabetes insipidus produce dilute urine because of a decrease in ADH secretion from the hypothalamus; those with nephrogenic DI exhibit a decreased response to ADH at the renal tubule.
• Osmotic demyelination syndrome, the most serious complication of the treatment of hyponatremia, occurs when the administration of relatively hyperosmolar intravenous fluid causes intracellular water to rapidly diffuse out of central nervous system cells.
• The most serious complication of therapy for hypernatremia is the development of cerebral edema secondary to excessively rapid rehydration.
Scope
Hyponatremia is diagnosed when the serum sodium level is lower than 135 mEq/L, but clinical signs and symptoms most often occur when sodium falls below 130. Hyponatremia most commonly occurs in the very young and the very old, with prevalence increasing with advancing age. Hyponatremia is observed in infants given tap water as a home remedy for gastroenteritis and in elderly patients with a poorly regulated thirst mechanism or an inability to procure fluids because of immobility (or both).1,2
Hypernatremia, a plasma sodium level higher than 145 mEq/L, most commonly results from inadequate water intake. In the very young, this situation usually occurs secondary to water loss exceeding intake, such as with diarrheal illness; in the geriatric population, hypernatremia may result from a poor sense of thirst or an inability to obtain adequate fluids because of physical or mental impairment. Hypernatremia is less common than hyponatremia, but it is associated with a far greater mortality rate of approximately 50%, primarily from the causative disease states in elderly patients and from the direct neurologic effects of the high sodium concentration in the very young.3
Pathophysiology
Hyponatremia
The low osmolality of the intravascular space and the relatively high osmolality of the intracellular space results in an osmotic gradient and diffusion of water into the cell. The resulting cellular edema is generally well tolerated by most tissues, except when it occurs in a confined space such as the central nervous system (CNS). The initial, rapid response to the increase in CNS cellular volume is diffusion of electrolytes and water out of the cell, which leads to a partial reduction in glial cell volume. Continuing hyponatremia over the next 48 to 72 hours generates slow diffusion of organic osmolytes, primarily large amino acids, out of the cell, thereby further reducing cell volume.4 Treatment of hyponatremia with intravenous fluid (IVF) may then lead to a state of relative hyperosmolality in the extracellular space with resultant diffusion of water out of the cell and continued reduction in cellular volume. This cycle creates the most serious treatment complication of hyponatremia: osmotic demyelination syndrome (otherwise known as central pontine myelinolysis).5
Hypernatremia
In hypernatremia, water diffuses out of the cell along the osmotic gradient, which results in loss of cellular volume. In the acute phase, electrolytes and water rapidly diffuse into the cell to partially restore cellular volume. With ongoing hypernatremia, slow redistribution of osmolytes occurs and water diffuses into the cell. With treatment, the relatively hyposmolar IVF leads to an osmotic gradient that promotes further diffusion of water into the cell. The size of the larger organic osmolytes prevents rapid diffusion out of the cell and results in the most serious treatment complication of hypernatremia: cerebral edema.6,7
Clinical Presentation
Hyponatremia
Symptoms of hyponatremia include nausea, headache, and general malaise with sodium levels of 125 to 130 and lethargy, confusion, agitation, psychosis, and seizures as the sodium level falls to the range of 115 to 120; severe symptoms develop at 110 regardless of the rate of change. Severe CNS signs observed with hyponatremia include a decreased level of alertness, focal or generalized seizure activity, and signs of brainstem herniation such as unilateral dilated pupil, posturing, and respiratory arrest.8
Hypernatremia
The signs and symptoms of hypernatremia depend on age. Infants exhibit restlessness, tachypnea, characteristic high-pitched crying, alternating irritability and lethargy, and hypotonia. Elderly patients have nausea, weakness, altered mental status, agitation, irritability, lethargy, stupor, coma, and seizures. The severity of the CNS symptoms correlates with serum sodium levels.9
Differential Diagnosis and Classifications
Hyponatremia
The differential diagnosis of hyponatremia begins with determination of serum osmolality (Fig. 164.1).4 Osmolality is measured by osmometry in the laboratory or is calculated according to the following formula:
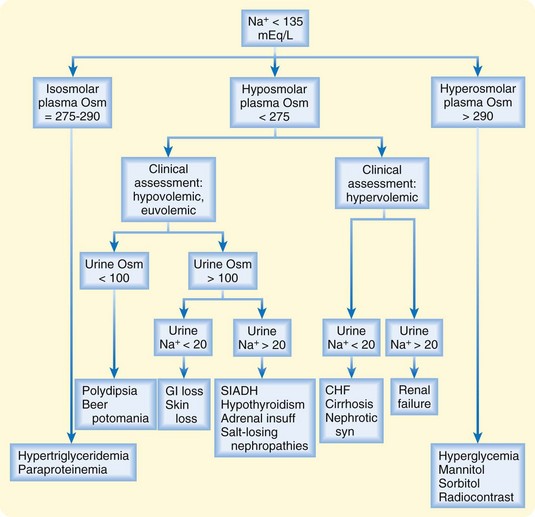
Fig. 164.1 Diagnostic algorithm for hyponatremia.
(Adapted from Kumar S, Berl T. Sodium. Lancet 1998;352:220-8.)




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


