4 Shock
 Key Points
Key Points• Circulatory dysfunction can occur at three levels—the central circulation, the peripheral circulation, and the microcirculation—sometimes with subtle clinical findings.
• The initial history and physical examination should focus on identifying signs of hypoperfusion and detecting any immediately life-threatening circulatory disorders.
• Bedside ultrasonography can be helpful in assessing intravascular volume status and cardiac function and in detecting vascular catastrophes.
• Circulatory support is aimed at restoring adequate oxygen delivery.
• End points of circulatory resuscitation include clinical signs, mean arterial blood pressure, serum lactate level, and central venous oxygenation.
Pathophysiology of Circulatory Dysfunction
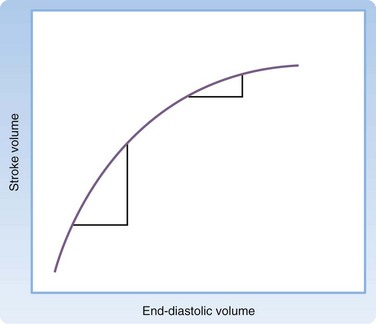
Cardiac output can be affected by the heart rate, arrhythmias, and alterations in ventricular loading. Preload, afterload, and contractility each affect ventricular loading. The Frank-Starling law (Fig. 4.2) states that the principal force governing the strength of ventricular contraction is the length of muscle fibers.1 In a normal heart, muscle fiber length is determined by intravascular volume, often termed preload. As preload increases, myocardial fibers increase in length, which results in increased force of contraction. Increased force of ventricular contraction increases stroke volume and cardiac output. In contrast, depletion of intravascular volume results in muscle fiber shortening, less forceful cardiac contractions, lower stroke volume, and decreased cardiac output.
Circulatory dysfunction exists as a spectrum ranging from mild impairment to shock with overt circulatory collapse. Shock is defined as the inability of the circulatory system to provide adequate tissue perfusion, which potentially leads to cellular dysfunction.1 Four categories of shock have been differentiated and defined by the underlying patho-physiology of the circulatory dysfunction: hypovolemic, cardiogenic, distributive, and obstructive (Box 4.1).2 Because each category requires specialized management, every attempt must be made to determine the exact cause of the shock.
Initial Assessment
Vital Signs
For nearly all ED patients, circulatory assessment begins with the noninvasive measurement of vital signs. Although blood pressure and heart rate are central to the initial assessment, it is important to note the respiratory rate and oxygen saturation. Any abnormality in the respiratory rate or oxygen saturation may affect arterial oxygen content and impair oxygen delivery. Noninvasive measurement of vital signs correlates poorly with organ perfusion in critically ill patients but serves as an important component of the initial ED assessment of the circulatory system.3
Blood Pressure
Blood pressure, the driving force for organ perfusion, is determined by cardiac output and arterial tone.1 It is important to understand that no blood pressure value is considered normal for every patient. Normal blood pressure values do not always indicate sufficient oxygen delivery. Blood pressure values should be interpreted in the context of the patient’s clinical findings, medical history, and treatment received.
Blood pressure is one of the most common measurements in all of clinical medicine, yet it is often measured incorrectly.4 In the ED, blood pressure is initially obtained during triage with automated blood pressure devices that apply the oscillometric method. These devices can be adversely affected by ambient noise and cuff position. In addition, automated devices typically overestimate true arterial blood pressure in patients with low-flow states. These limitations, combined with activity in the triage environment and patient anxiety, often result in inaccurate measurements of blood pressure. Understandably, triage values can be an unreliable indicator of true blood pressure. Blood pressure measurements should be repeated serially at the bedside in patients demonstrating any evidence of circulatory insufficiency.
1. Remove all clothing from the arm and place the blood pressure cuff so that the middle of the cuff is approximately at the level of the right atrium. The lower edge of the cuff should be 2 to 3 cm above the antecubital fossa to allow easy palpation and auscultation of the brachial artery.
2. Locate the radial artery and inflate the blood pressure cuff to approximately 30 mm Hg above the point at which the radial arterial pulse disappears.
3. Place the bell of the stethoscope over the brachial artery and deflate the cuff at a rate of 2 to 3 mm Hg per second. The appearance of faint, repetitive sounds for at least two consecutive beats is phase I of the Korotkoff sounds. Phase I is systolic blood pressure. The point at which all sounds disappear is phase V, or diastolic blood pressure.
Measure blood pressure bilaterally during the initial circulatory examination. A difference of more than 10 mm Hg is significant and may indicate an aortic emergency. Unfortunately, up to 20% of individuals have significant blood pressure differences between their arms.5 Nevertheless, an aortic emergency must be ruled out in any patient with evidence of circulatory insufficiency and blood pressure discrepancies.
Though considered the gold standard, the auscultatory method has several pitfalls. Box 4.2 lists errors commonly made during measurement of blood pressure with the auscultatory method.
Heart Rate
The heart rate is an integral component of cardiac output. Tachycardia or bradycardia can impair circulatory function. As with blood pressure, triage measurements of the heart rate can be inaccurate and unreliable. Therefore, heart rate measurement should be repeated in every patient on initial examination. In addition to the rate, irregularities in rhythm should be noted. Arrhythmias can severely compromise circulatory function and organ perfusion. Furthermore, heart rate variability may be an early indication of circulatory dysfunction.6 Methods to determine heart rate variability remain investi-gational and require additional research before clinical application.
Orthostatic Blood Pressure
A positive orthostatic blood pressure response is defined as a reduction in systolic blood pressure of at least 20 mm Hg or a reduction in diastolic blood pressure of at least 10 mm Hg within 3 minutes after standing in a patient with symptoms of volume depletion.7 Orthostatic blood pressure should be measured with the patient in the supine and standing positions. For patients who are unable to stand or who are markedly unsteady, a sitting position may be used. Wait at least 2 minutes before obtaining a standing blood pressure measurement because nearly all patients have a brief orthostatic response immediately on standing. Always measure the heart rate with orthostatic blood pressure. In normal patients, the heart rate increases from 5 to 12 beats/min with standing. Increases greater than 30 beats/min are abnormal and indicate significant volume depletion.
Orthostatic blood pressure measurements have several limitations. Numerous conditions in addition to volume depletion impair the postural hemodynamic response and result in orthostatic hypotension. Most notable are the effects of aging and medications. Up to 30% of elderly patients demonstrate an orthostatic response in the absence of volume depletion.8 Many elderly patients take medications that alter the postural response to changes in position; such medications include antiadrenergics, antidepressants, antihypertensives, neuroleptics, anticholinergics, and antiparkinsonian drugs. In addition, any disorder causing primary or secondary autonomic dysfunction can lead to orthostatic hypotension.
Physical Examination
Physical examination of the circulatory system begins with the general appearance of the patient. Observe the patient’s positioning, mental status, skin color, and respiratory pattern. Suspect circulatory abnormalities in restless, diaphoretic, delirious, pale, mottled, or tachypneic patients. In addition, note any distinct clinical features implying an underlying medical condition. Table 4.1 lists the characteristic features of disorders that can affect the circulatory system.
Table 4.1 Characteristics of Conditions That Affect the Circulatory System
| CONDITION | CLINICAL APPEARANCE | POTENTIAL CIRCULATORY IMPLICATIONS |
|---|---|---|
| Marfan syndrome | Arachnodactyly Arm span greater than height Longer pubis-to-foot length than pubis-to-head length | Aortic dissection |
| Osteogenesis imperfecta | Blue sclera | Aortic dissection Aortic aneurysm Aortic valve insufficiency Mitral valve prolapse |
| Hyperthyroidism | Exophthalmos | Congestive heart failure |
| Hypothyroidism | Expressionless face Periorbital edema Loss of lateral third of the eyebrows Dry, sparse hair | Congestive heart failure Pericardial effusion |
| Hemochromatosis | Bronze pigmentation of skin Loss of axillary and pubic hair | Cardiomyopathy |
| Turner syndrome | Short stature Webbed neck “Shield” chest Medial deviation of the extended forearm | Aortic coarctation |
| Aortic insufficiency | Bobbing of the head with heartbeat Systolic flushing of the nail beds | — |
Examine the head and neck for abnormalities suggesting circulatory disease. Facial edema implies impaired venous return resulting from conditions such as superior vena cava thrombosis and constrictive pericarditis. Examination of the jugular venous pulse provides important information about central venous pressure (CVP) and the dynamics of the right side of the heart.9 Place the patient in a 45-degree recumbent position and shine a light tangentially across the neck. The right side is preferred because of its anatomic alignment with the superior vena cava and right atrium. Beginning at the sternal notch, measure the height (in centimeters) of the internal jugular vein pulsations. Pulsations more than 4 cm above the sternal notch are abnormal and a sign of elevated CVP.9 Figure 4.3 illustrates jugular venous distention in a young woman with pericardial effusion.








