Reactive Airways Disease
Bret P. Nelson
Andy S. Jagoda
THE CLINICAL CHALLENGE
There are a number of confounders that make airway management of the patient with asthma or chronic obstructive pulmonary disease (COPD) challenging. These patients are often hypoxic, desaturate quickly, and can be hemodynamically unstable. Unlike many other clinical conditions, intubation itself does not resolve the primary problem, which is obstruction of the small, distal airways. The actual intubation may be the easiest part of the resuscitative sequence because postintubation ventilation may be extremely difficult with persistent or worsening respiratory acidosis, barotrauma, or worsening hypotension caused by high-intrathoracic pressures with diminished venous return. Thus, the decision to intubate must be made carefully, and the appropriate technique must be chosen to facilitate the best possible outcome.
Severe asthma often presents one of the most difficult airway management cases encountered in the emergency department. Diaphoresis is a particularly ominous sign, and the diaphoretic asthmatic patient who cannot speak full sentences, appears anxious, or is sitting upright and leaning forward to augment the inspiratory effort must not be left unattended until stabilized.
Standard initial management of acute severe asthma exacerbation includes reversal of dynamic bronchospasm using continuous β2-agonist nebulization therapy (Albuterol 10-15 mg per hour) and anticholinergic nebulization therapy (ipratropium bromide 0.5 mg every 20 minutes for three doses). In addition, oral or intravenous (IV) steroids are indicated for the treatment of the inflammatory component. If the patient is severely bronchospastic and cannot comply with a nebulized treatment, subcutaneous epinephrine or terbutaline 0.3 to 0.5 mg may be of benefit. The use of IV terbutaline is controversial; and has no proven benefit in adults. However, if selected, it should be initiated in the child at 10 µg per kg over 30 minutes followed by a continuous infusion of 0.1-0.4 µg/kg/minute. For severe, refractory asthma, administration of IV magnesium sulfate 2 g in adults and 25-75 mg per kg (up to a maximum of 2 g) in children may be of benefit, although evidence supporting this is mixed. The addition of inhaled or IV anticholinergic agents (atropine or glycopyrrolate), titrated doses of IV ketamine, or inhalational helium/oxygen mixture is controversial but also may be considered in severe cases (Fig. 33-1).
In COPD, much of the obstruction is fixed, comorbidity (especially cardiovascular disease) plays a greater role, and the prognosis (even with short-term mechanical ventilation) is worse. In the patient with COPD, anticholinergic therapy may be as important as β2-agonist therapy. Steroids are again important to attenuate underlying inflammation. As is the case for many asthma patients, it is progression of fatigue, not worsening bronchospasm that leads to respiratory failure and arrest. The intubated COPD patient may have a prolonged, difficult course, and weaning from the ventilator is not assured. Therefore, unless the patient’s condition forces early or immediate intubation, a trial of noninvasive ventilation is recommended. Noninvasive ventilation (bi-level positive airway pressure [BL-PAP] or continuous positive airway pressure) is of proven value in certain COPD patients and may help avoid intubation (see Chapter 6). As for the asthmatic patient, mechanical ventilation after intubation in COPD is notoriously difficult to manage. Ventilation pressures often are high, and breath stacking (automatic positive end-expiratory pressure [auto-PEEP]) is common, even with excellent ventilator management. Increased intrathoracic pressures induced by mechanical ventilation, combined with volume depletion from the patient’s work of breathing before intubation, coexisting cardiovascular disease, and hemodynamic changes related to decreased sympathetic tone after intubation makes the peri-intubation period highly dynamic and unstable. Ventilator management is discussed below. There is no role for IV aminophylline in the management of either acute severe asthma or acute severe COPD exacerbation, before or after intubation.
APPROACH TO THE AIRWAY
Despite this vast array of noninvasive treatment modalities, 1% to 3% of acute severe asthma exacerbations will require intubation. These patients are usually fatigued and have reduced functional residual capacity, so it is difficult (if not impossible) to preoxygenate them optimally, and rapid desaturation
must be anticipated. Because most of these patients have been struggling to breathe against severe resistance, usually for hours, they have little if any residual physical reserve, and mechanical ventilation will be required. In fact, the need for mechanical ventilation is the indication for tracheal intubation; the airway itself is almost invariably patent and protected. This fact argues strongly for rapid sequence intubation (RSI), which often is the preferred method even if a difficult airway is identified on preintubation assessment (the “forced to act” scenario; see Chapters 2 and 3). If the patient has a difficult airway, the operator might plan intubation even earlier than for the nondifficult patient, in an attempt to have the best conditions and greatest amount of time possible for an awake technique.
must be anticipated. Because most of these patients have been struggling to breathe against severe resistance, usually for hours, they have little if any residual physical reserve, and mechanical ventilation will be required. In fact, the need for mechanical ventilation is the indication for tracheal intubation; the airway itself is almost invariably patent and protected. This fact argues strongly for rapid sequence intubation (RSI), which often is the preferred method even if a difficult airway is identified on preintubation assessment (the “forced to act” scenario; see Chapters 2 and 3). If the patient has a difficult airway, the operator might plan intubation even earlier than for the nondifficult patient, in an attempt to have the best conditions and greatest amount of time possible for an awake technique.
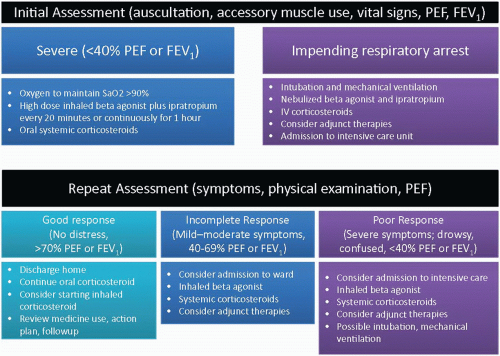 Figure 33-1 • Approach to the Patient with Severe Asthma Exacerbation. (Adapted from National Heart, Lung, and Blood Institute, National Institutes of Health, National Asthma Education and Prevention Program. Expert Panel Report 3 (EPR-3): Guidelines for the Diagnosis and Management of Asthma—Summary Report 2007. NIH publication 08-5846. http://www.nhlbi.nih.gov/guidelines/asthma/asthsumm.pdf. Accessed May 15, 2011.) |
Technique
The single most important tenet in managing the status asthmaticus patient who requires intubation is to take total control of the airway as expeditiously as possible. Patients typically adopt an upright posture as their respiratory status worsens; this position should be maintained as much as possible during the preintubation period. Preoxygenation should be achieved to the greatest extent possible (see Chapters 5 and 19). Noninvasive ventilation may be considered as a means of increasing FiO2 during this phase while decreasing work of breathing. The RSI drugs chosen should be administered with the patient in their position of comfort, often sitting upright. As the patient loses consciousness, place the patient supine, position the head and neck, and perform laryngoscopy and intubation, preferably with an 8.0- to 9.0-mm endotracheal tube to decrease resistance and facilitate pulmonary toilette. If bag-mask ventilation is required because of desaturation before intubation is achieved, Sellick maneuver may help prevent the passage of air down the esophagus, particularly in these patients, who have high pulmonary resistance to ventilation.
Drug Dosing and Administration
If time permits, patients with reactive airways disease or obstructive lung disease should be pretreated with 1.5 mg per kg of IV lidocaine 3 minutes before induction to attenuate the reflexive bronchospasm in response to airway manipulation. Ketamine is the induction agent of choice in the asthmatic patient because it stimulates the release of catecholamines and also has a direct bronchial smooth muscle relaxing effect that may be important in this clinical setting. Ketamine 1.5 mg per kg IV is given immediately before the administration of 1.5 mg per kg of succinylcholine or 1.0 mg per kg of rocuronium. If ketamine is not available, any of the other commonly used induction agents (propofol, etomidate, and midazolam) may be used, but the barbiturates should be avoided as they release histamine. For COPD patients, who often have concomitant cardiovascular disease, etomidate may be preferred to avoid the catecholamine stimulation of ketamine.
POSTINTUBATION MANAGEMENT
After the patient is successfully intubated and proper tube position has been confirmed, sedation and analgesia are titrated according to a sedation scale (see Chapter 19). Neuromuscular blockade may be required during the first few hours of mechanical ventilation to prevent asynchronous respirations, promote total relaxation of fatigued respiratory muscles, decrease the production of carbon dioxide, and allow optimal ventilator settings. Often, though, these same goals are achieved using a proper balance of sedation and analgesia. Prolonged neuromuscular blockade is not required and may worsen the patient’s overall course of management. Meticulous ventilator management is critical in achieving the best patient outcome. Additional ketamine, as well as continuous in-line albuterol and other pharmacologic adjuncts, may also be given.
Mechanical Ventilation
All asthmatic patients have obstructed small airways and dynamic alveolar hyperinflation with varying amounts of end-expiratory residual intra-alveolar gas and pressure (auto-PEEP or intrinsic PEEP). Elevations in auto-PEEP increase the risk for baro/volutrauma. Reversal of airflow obstruction and decompression of end-expiratory filled alveoli are the primary goals of early mechanical ventilation in the asthmatic patient. The former requires prompt administration of IV steroids and continuous in-line nebulization with β2-agonists until reversal is objectively measured (decrease in peak and plateau airway pressures) or unacceptable side effects are produced. Safe, uncomplicated alveolar decompression requires prolonged expiratory time (inspiration/expiration [I/E] ratio of 1:4 to 1:5), which is achieved by using smaller tidal volumes than usual, with a highinspiratory flow (IF) rate to shorten the inspiratory cycle time, permitting a longer expiratory phase. A general discussion of ventilation parameters can be found in Chapter 7.
The initial goal of ventilator therapy in the asthmatic patient is to improve arterial oxygen tension to adequate levels without inflicting barotrauma on the lungs or increasing auto-PEEP. Initial tidal volume should be reduced to 6 to 8 ml per kg to avoid barotrauma and air trapping. The speed at which a mechanical breath is delivered in liters per minute, typically 60 L per minute, is called the inspiratory flow rate (IFR). In asthma, the initial IFR should be increased to 80 to 100 L per minute with a decelerating flow pattern. Pressure control is preferred to volume control because of the lower risk of barotrauma. If volume control is used, the operator should select the flow waveform to use ramp (decelerating) instead of square (constant). The ventilation rate should be determined in conjunction with the tidal volume. An initial rate of 8 to 10 breaths per minute (bpm) with a high IFR promotes a prolonged expiratory phase that allows sufficient time for alveolar decompression. It is acceptable to permit the maintenance or gradual development of hypercapnia through reduced minute ventilation (the product of tidal volume and ventilatory rate) in the asthma or COPD patient because this approach reduces peak inspiratory pressure (PIP) and thus minimizes the potential for barotrauma. High intrathoracic pressure may compromise cardiac output and produce hypotension; therefore, it is to be avoided.
The highest measured pressure at peak inspiration is the PIP. The patient’s lungs, chest wall, endotracheal tube, ventilatory circuit, ventilator, and mucus plugs all contribute to the PIP. This reading has an inconsistent predictive value for baro/volutrauma, but ideally should be kept under 50 cm H2O. A sudden rise in PIP should be interpreted as indicating tube blockage, mucous plugging, or pneumothorax until proven otherwise. A sudden, dramatic fall in PIP may indicate extubation.
The measured intra-alveolar pressure during a 0.2- to 0.4-second end-inspiratory pause is referred to as the plateau pressure (Pplat). Values <30 cm H2O are best and are not usually associated with baro/volutrauma. Measurement and trending of Pplat is an excellent objective tool to confirm optimal ventilator settings and the patient’s response, as well as the reversal of airflow obstruction. If initial ventilator settings disclose a Pplat of more than 30 cm H2O, consider lowering minute ventilation and increasing IF, both of which will prolong expiratory time and attenuate hyperinflation. If Pplat is unavailable, PIP may be used as a surrogate.
Most status asthmaticus patients who require intubation are hypercapnic. The concept of controlled hypoventilation (permissive hypercapnia) promotes gradual development (over 3 to 4 hours) and maintenance of hypercapnia (PCO2 up to 90 mm Hg) and acidemia (pH as low as 7.2). This treatment is done primarily to decrease the risk of ventilator-related lung injury and prevent hemodynamic compromise as a result of increasing intrathoracic pressure from auto-PEEP or intrinsic PEEP. Permissive hypercapnia is usually accomplished by reducing minute ventilation, increasing IF rate to 80 to 120 L per minute. Optimal sedation and analgesia is required, with some patients also requiring neuromuscular blockade, to tolerate these settings. Permissive hypercapnia may be instrumental in promoting prolonged expiratory times and reducing auto-PEEP.
Summary for Initial Ventilator Settings
1. Determine the patient’s ideal body weight.
2. Set a tidal volume of 6 to 8 ml per kg with FiO2 of 1.0 (100% oxygen).
3. Set a respiratory rate of 8 to 10 bpm.
4. Set an I/E ratio of 1:4 to 1:5. Pressure control is preferred. If using pressure control, the I/E ratio is adjusted directly by the I/E ratio parameter or by adjusting the inspiratory time parameter. If using volume control, the I/E ratio can be adjusted by increasing the peak flow rate, and the ramp inspiratory waveform should be selected. Peak IF can be as high as 80 to 100 L per minute.









