the formation of clot in the calf veins, which propagates proximally to larger veins in the leg (popliteal, femoral, or iliac). Thrombus in these large proximal leg veins are more likely to cause physiologically significant PE than emboli from the smaller calf veins.
incidence of VTE (within 91 days) in patients undergoing specific types of surgery.16 This study did not analyze thromboprophylactic practice and excluded patients with a previous diagnosis of VTE. Different thromboprophylactic practices in the groups studied may alter the rate of VTE and change the interpretation of the risk of VTE from a surgery16 (see Table 13.2).
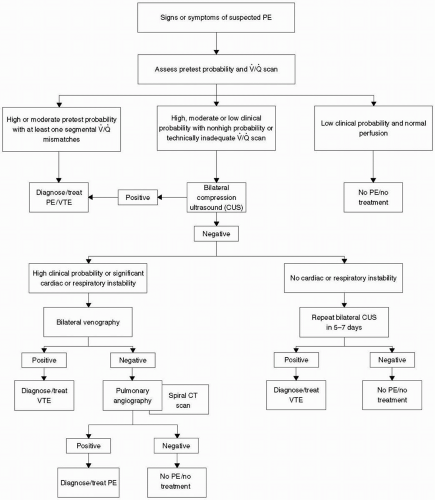 FIGURE 13.1 Diagnostic algorithm for patients with suspected pulmonary embolism. PE, pulmonary embolism; VTE, venous thromboembolism; CUS, compression ultrasound; CT, computed tomography. |
preventative therapy for postoperative VTE should be based on the patient’s risk for developing VTE17 as shown in Table 13.3.
TABLE 13.1 Risk Factors for Deep Venous Thrombosis | ||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
TABLE 13.2 Surgical Procedure Related to Risk of Venous Thromboembolism | ||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||
TABLE 13.3 Preventive Therapy Related to Risk of Developing Postoperative Venous Thromboembolism | |||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


