97 Peripheral Nerve Disorders
 Key Points
Key Points• Nerve compression is the most common cause of radiculopathy and mononeuropathy.
• Radiculopathy and radicular pain are typically associated with symptoms within a dermatome or myotome.
• Patients with mononeuropathy have symptoms limited to a single peripheral nerve.
• Guillain-Barré syndrome is an autoimmune demyelinating disease that results in primarily motor symptoms, with severe disease leading to respiratory compromise.
• Myasthenia gravis and Lambert-Eaton myasthenic syndrome are both autoimmune disorders of the neuromuscular junction; myasthenia gravis affects the postsynaptic membrane, whereas Lambert-Eaton syndrome affects the presynaptic membrane.
• Botulism is a toxin-mediated disorder of the neuromuscular junction.
• Systemic diseases such as diabetes mellitus and human immunodeficiency virus infection can result in several peripheral nerve disorders.
Perspective
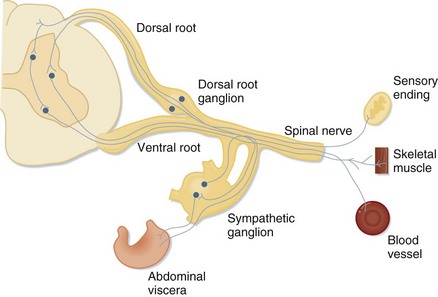
Evaluation of peripheral nerve disorders requires an understanding of the anatomy of the spinal cord and the peripheral nervous system (Fig. 97.1). The peripheral nervous system is composed of 12 cranial nerves and 31 spinal nerves. Spinal nerves are formed from motor fibers whose cell bodies reside in the ventral horn of the spinal cord and from sensory fibers whose cell bodies are found in the dorsal root ganglion. The motor and sensory fibers join to form one nerve as it exits the spinal canal. Spinal nerves from several spinal levels merge at the cervical, brachial, lumbar, and sacral plexuses. Peripheral nerves originate either at these plexuses or, if they are formed from nerves of only one spinal level, as they exit the vertebral foramina.
Systemic diseases affect the peripheral nervous system as well, and multiple peripheral nerves may be involved. Examples include disorders of the neuromuscular junction (NMJ), demyelinating disorders, diabetes, and toxic effects of drugs or chemicals (Box 97.1).
Radiculopathies
Presenting Signs and Symptoms
As noted, sensory loss and weakness follow a dermatomal or myotomal distribution. Diminished reflexes may also assist in determining the nerve root that is involved (Table 97.1).
Table 97.1 Nerve Root and Associated Reflex
| NERVE ROOT | REFLEX |
|---|---|
| C5-6 | Brachioradialis |
| C7-8 | Triceps |
| L3-4 | Patellar |
| S1 | Achilles |
Treatment
In the acute phase of injury, painful symptoms are typically treated conservatively with nonsteroidal antiinflammatory drugs (NSAIDs) and physical therapy. Low-quality evidence suggests that there is no difference between bed rest and activity for patients with sciatica.1 However, a randomized controlled trial showed that the addition of physical therapy is more effective than counseling and pain medications alone, although it may not be as cost-effective.2 Persistent or severe symptoms may require more invasive measures, from local corticosteroid injections to neurosurgical intervention.3 For the cervical spinal nerves, some evidence has shown that conservative therapy consisting of pain control has favorable short-term outcomes when compared with surgical intervention, although long-term outcomes appear to be similar.4 Surgical outcomes can be dependent on the mechanism of injury; for example, with spinal stenosis, 70% of patients will still have persistent loss of function. Chronic pain symptoms may be treated with medications used for neuropathic pain, such as antidepressants or anticonvulsants.
Mononeuropathies
Epidemiology
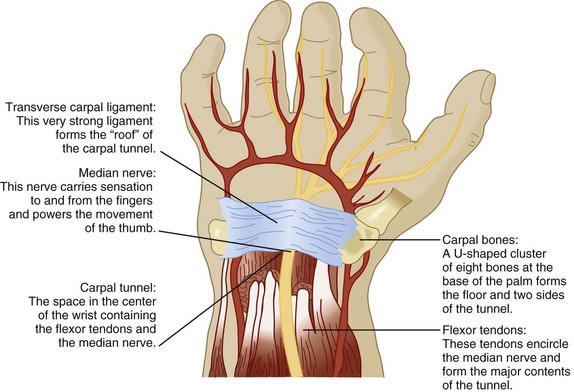
As with radiculopathy, compression of peripheral nerves is the most common cause of peripheral mononeuropathy, the most frequent being median mononeuropathy (Fig. 97.2). Women older than 55 years are most commonly affected, with a 4.6% prevalence in women and 2.8% in men.5 The second most frequent cause is ulnar mononeuropathy; specifically, cubital tunnel syndrome. Other common peripheral mononeuropathies include involvement of the radial nerve in the upper extremity and the peroneal and lateral cutaneous femoral nerves in the lower extremity.
Pathophysiology, Presenting Signs and Symptoms, and Diagnostic Testing
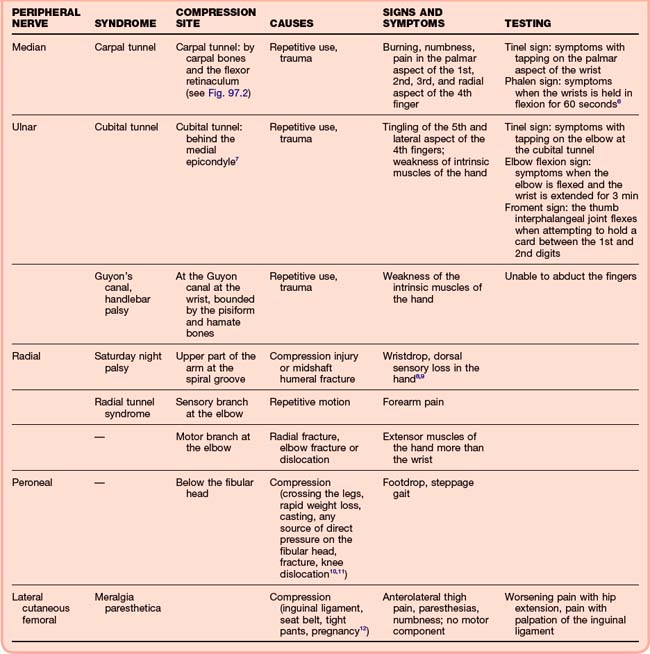
For mononeuropathies, the history and physical examination largely lead to the appropriate diagnosis. Findings in patients with common mononeuropathies and diagnostic maneuvers are presented in Table 97.2.6–12 In patients with a history of trauma or acute symptoms, plain films may be necessary to rule out fracture or dislocation. Patients with subacute or chronic symptoms should be asked about chronic conditions. Mononeuropathies can occur with several systemic diseases, including diabetes mellitus, amyloidosis, HIV, and states that cause edema, such as pregnancy.13 Outpatient testing may be more appropriate for individuals with chronic symptoms. MRI or electrodiagnostic testing such as electromyography or nerve conduction studies may be necessary, and the patient should be referred to a neurologist. MRI may demonstrate chronic nerve injury, whereas electrodiagnostic testing may show slowing of nerve conduction. These studies may aid in deciding whether surgical repair or decompression is necessary for certain syndromes.
Treatment
Initial treatment of chronic mononeuropathy is typically conservative and supportive. Modification of behavior is a key component of treatment and prevention of further injury. For carpal tunnel syndrome, behavior modification includes weight loss and avoidance of caffeine, nicotine, and alcohol. Patients should be instructed to decrease any possible trauma related to repetitive use by making changes in workplace ergonomics, reducing repetitive use, and changing posture. Some neuropathies may require supportive devices; for example, the carpal tunnel may benefit from wearing a wrist splint, the ulnar nerve from wearing a sling or a long arm posterior splint, the radial nerve from wearing a volar splint, and the peroneal nerve from wearing a posterior splint.8,9 NSAIDs are typically prescribed for relief of symptoms, although they may be ineffective without appropriate behavioral modification. In patients with a systemic disease, the primary process should be treated. Diuretics may be given if edema is believed to be contributing significantly to the patient’s symptoms. More invasive procedures, such as local nerve block for meralgia paresthetica or surgical decompression for carpal tunnel syndrome, are reserved for severe cases.
Autoimmune Disorders
Guillain-Barré Syndrome
Epidemiology
Guillain-Barré syndrome (GBS) is also known as acute inflammatory demyelinating polyradiculopathy or Landry-Guillain-Barré syndrome. Its worldwide incidence is 0.6 to 4 per 100,000 individuals annually.14
Presenting Signs and Symptoms
Classic Guillain-Barré Syndrome
Classic GBS is preceded by a viral prodrome and followed by acute or subacute ascending symmetric weakness or paralysis and loss of the deep tendon reflexes. Paralysis may ascend to the diaphragm and compromise respiratory function to the extent that mechanical ventilation is required. One third of patients will require intubation and 15% will experience dysautonomia. Specific findings are strongly suggestive of this diagnosis (Box 97.2).







