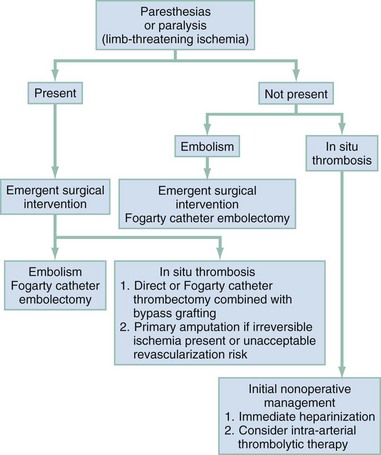
Chapter 87 Atherosclerosis: Atherosclerosis is a disease of large- and medium-sized muscular arteries. The basic lesion, the atheroma, or fibrofatty plaque, is a raised focal plaque within the intima; it has a lipid core (mainly cholesterol, usually complexed to proteins and cholesterol esters) covered by a fibrous cap. As the plaques increase in size and number, they progressively encroach on the lumen of the artery and the adjacent media. Atheromas compromise arterial blood flow and weaken the walls of the affected arteries. Aneurysms: A true aneurysm is an abnormal localized dilation of the intact vessel wall. With a pseudoaneurysm the entire wall perforates or ruptures, and the extravasated blood is contained by the surrounding tissues, eventually forming a fibrous sac that communicates with the artery. Mural and mechanical factors contribute to true aneurysm formation.1 The major cause of aneurysms is a weakness or defect in the integrity of the arterial wall. The only aneurysms that develop in a normal arterial segment are poststenotic aneurysms, such as with coarctation. Acceleration of flow past a narrow point creates slower flow beyond the stenosis lateral to the jet stream, producing increased lateral pressure. Aneurysmal dilation accelerates, increasing the risk of rupture as diameter increases, as predicted by Laplace’s law: tension (lateral pressure) in the wall of a hollow viscus varies directly with its radius (tension = pressure × radius). Arterial Embolism: An embolus is a blood clot or other foreign body that is carried by the blood to a site distant from its point of origin. Most emboli are the result of detached thrombus formation (thromboembolism). Less common sources include debris from ruptured atherosclerotic plaques, tumor debris, or foreign bodies. Unless otherwise specified, the term embolus in this chapter is defined as thromboembolus. Thromboembolism.: Most arterial emboli (85%) originate in thrombus formation in the heart. Left ventricular thrombus formation resulting from myocardial infarction accounts for 60 to 70% of arterial emboli. Atrial thrombi associated with mitral stenosis and rheumatic heart disease account for only 5 to 10% of arterial emboli.2 Coexisting atrial fibrillation, often without mitral stenosis, is present in 60 to 75% of patients with peripheral arterial embolic events, because atrial fibrillation itself can predispose patients to intracardiac clotting.3 Because vessel diameters change most abruptly at branch points, embolic occlusion most often occurs at major arterial bifurcations. The bifurcation of the common femoral artery is the most frequent site of arterial embolism, accounting for 35 to 50% of all cases.2 The smaller femoral and popliteal arteries are involved twice as often as the larger aortic and iliac vessels, reflecting the small size of most emboli. Cell death from arterial ischemia can produce high concentrations of potassium, lactic acid, and myoglobin in the extremity distal to an arterial occlusion. Their sudden release after revascularization can produce life-threatening hyperkalemia, metabolic acidosis, and myoglobinuria. This myonephropathic-metabolic syndrome accounts for approximately one third of the deaths from arterial embolism after revascularization.4 Atheroembolism.: Atheroembolism refers to microemboli consisting of cholesterol, calcium, and platelet aggregates dislodged from proximal complicated atherosclerotic plaques that lodge in distal end arteries. In the central nervous system, atheroemboli cause transient ischemic attacks and strokes. In the peripheral vascular system, atheroemboli characteristically cause cool, painful, and cyanotic toes, or the blue toe syndrome.5 Atheroemboli are caused by a proximally located arterial lesion, usually atherosclerotic plaques or aneurysms. Bilateral distal extremity involvement usually implies an aortic source, whereas unilateral atheroemboli usually arise from sites distal to the aorta. Distal lesions are most common in the femoropopliteal arteries (60%) and the aortoiliac arteries (40%). Aortic lesions (e.g., aneurysms, polytetrafluoroethylene grafts) are a less common source of microemboli.5 Atheroemboli are small and tend to lodge in distal arteries, such as the digital arteries, which are 100 to 200 µm in size. Single atheroembolic events seldom result in tissue loss, but atheroemboli tend to cluster. If unrecognized, repeated events ultimately result in loss of collateral circulation, progressive symptoms, and extensive tissue infarction.5 Arterial Thrombosis: Thrombosis is the in situ formation of a blood clot within the uninterrupted arterial vascular system. Complicated atherosclerotic plaques are usually responsible for the two major factors that cause in situ thrombosis: endothelial injury and alterations in normal blood flow. Less common causes include acute vasculitis and trauma. Thrombosis is rare in normal arteries.6 Inflammation: Inflammatory arterial injury can be caused by drugs, irradiation, mechanical trauma, or bacterial invasion. The major cause of arteritis is noninfectious systemic necrotizing vasculitis. Most cases of infectious arteritis are caused by direct invasion of the arterial wall. Septicemia, intravenous drug abuse, or infective endocarditis is most often responsible. Certain fungal infections, particularly aspergillosis and mucormycosis, are frequently associated with vasculitis and thrombosis. Trauma: Different types of vascular injury result in characteristic pathologic syndromes. Partial arterial lacerations continue to bleed because the intact portion of the vessel wall prevents retraction and closure of the arterial wound. This may form an expanding hematoma, causing progressive deformity, pain, and nerve compression. Complete arterial transection usually has only moderate or insignificant bleeding because of arterial spasm of the transected ends of the artery and the formation of a temporary thrombus. Delayed hemorrhage in completely transected arteries may result from relaxation of arterial spasm, eventual liquefaction of the thrombus, or displacement of the thrombus by arterial pressure. Blunt injury may produce partial or complete intimal disruption. Dissection of the distal intima can lead to progressive obstruction and thrombosis. Complete occlusion may not occur for hours or days after injury. Vasospasm can accompany injuries that are adjacent to blood vessels; spontaneous resolution always occurs in the absence of arterial disruption or intimal injury. Vasospasm: Vasospastic disorders (Raynaud’s disease, Raynaud’s phenomenon, livedo reticularis, acrocyanosis, erythromelalgia) produce an abnormal vasomotor response in distal small arteries. The cause of these disorders is unknown but may be related to the autonomic innervation of the peripheral arterioles. The vasospastic disorders are characterized by the presence of ischemic symptoms and the absence of tissue loss. True organic changes within the arterial wall are absent. In contrast, patients with digital ulceration and gangrene always have fixed arterial occlusions in the distal extremity arteries. Arteriovenous Fistulae: Abnormal communication between arteries and veins may result from congenital defects, rupture of an arterial aneurysm into an adjacent vein, penetrating injuries, and inflammatory necrosis associated with neoplasms or infection. Arteriovenous fistulae can occur in any region of the body. The artery proximal to the fistula becomes distended, tortuous, and aneurysmal. Similar changes occur in the venous side of the fistula. Proximal and distal veins respond to alterations in hemodynamics with intimal proliferation and fibrosis, followed by a decrease in the internal elastic lamina, resulting in distention, tortuosity, and aneurysm formation. The resultant chronic venous hypertension may cause dermatitis and ulceration of overlying skin. The size of the fistula generally increases with time. Approximately 60% of arteriovenous fistulae are associated with a false aneurysm.7 False aneurysm formation can occur as part of the fistulous tract or as the result of arterial or venous dilation.7 Acute Arterial Occlusion: The patient with acute arterial occlusion usually exhibits some variant of the five Ps: pain, pallor, pulselessness, paresthesias, and paralysis. Paresthesias and paralysis indicate limb-threatening ischemia that requires emergency surgical intervention regardless of the cause. In patients with non–limb-threatening ischemia, accurate differentiation between embolism and in situ thrombosis as the cause of acute arterial occlusion determines management. Arterial embolism is best managed by emergency Fogarty catheter embolectomy. Non–limb-threatening ischemia from in situ thrombosis is often aggravated by emergency surgical intervention and is therefore initially best managed nonoperatively, if possible (Fig. 87-1). Because acute arterial embolism usually occurs in patients without significant peripheral atherosclerosis and without well-developed collateral circulation, it usually manifests as sudden limb-threatening ischemia. Patients describe a sensation of the leg’s being “struck” by a severe shocking pain. Often the patient has to sit or fall to the ground during the sudden event. Chronic Arterial Insufficiency: Chronic arterial insufficiency causes two characteristic types of pain: intermittent claudication and ischemic pain at rest. The location of arterial occlusion determines the location of claudication. Calf claudication is associated with femoral and popliteal disease, typically a cramping pain, reliably reproduced by the same degree of exercise and completely relieved by rest (usually 1-5 minutes). Aortoiliac occlusive disease causes claudication in the buttocks and hips, as well as the calves. The calf pain in aortoiliac disease is generally more severe than the buttock and thigh pain, which is more often described as an aching, discomfort, or weakness. Some patients deny pain, complaining only that the thigh or hip “gives out” with exercise. Aortoiliac occlusive disease severe enough to produce bilateral claudication is almost always associated with impotence in men (Leriche’s syndrome). Even in the absence of impotency, bilateral hip or thigh pain in a man should indicate the possibility of aortoiliac occlusive disease. A systematic assessment of the peripheral vascular system includes palpation of the pulse volume in the pairs of brachial, radial, femoral, posterior tibial, and dorsalis pedis arteries documented on a scale of 0 to 4+. Approximately 10% of the population does not have one of the dorsalis pedis pulses.8 Carotid arteries should be gently palpated one at a time. Arterial Embolism: The physical examination can differentiate arterial embolism from in situ thrombosis. The sudden loss of a pulse is the hallmark of arterial embolism but may be difficult to recognize if the prior pulse status is unknown or is abnormal as the result of associated atherosclerosis. A bounding pulse may be felt initially at the location of an embolus from transmitted pulsations through the fresh clot. In general, patients with arterial embolism have few physical findings suggestive of long-standing peripheral vascular disease with normal proximal and contralateral limb pulses. Tenderness to palpation may occur at the site of an embolic occlusion. Arterial Thrombosis: Physical findings of in situ thrombosis are often accompanied by evidence of atherosclerotic occlusive disease. Proximal or contralateral limb pulses are usually diminished or absent. An embolic source, such as mitral valve disease or atrial fibrillation, is usually absent. Because of collateral circulation, demarcation of limb ischemia is less well defined in these patients (Table 87-1). Table 87-1 Differentiation of Embolus from Thrombosis From Brewster DC, Chin AK, Fogarty TJ: Vascular Surgery. Philadelphia, WB Saunders, 1990. Inflammation: Inflammatory vascular disease manifests primarily as skin involvement. Skin lesions typically appear as palpable purpura; other cutaneous manifestations of vasculitis include macules, papules, vesicles, bullae, subcutaneous nodules, ulcers, and recurrent or chronic urticaria. The skin lesions may be pruritic or even painful, with a burning or stinging sensation. Lesions are more common in dependent areas: in the lower extremities in ambulatory patients or in the sacral area in bedridden patients. Edema accompanies some lesions, and hyperpigmentation occurs in areas of recurrent or chronic lesions. Vasospasm: Vasospastic disorders cause a sharp border between ischemic and normal tissue. Raynaud’s disease is characterized by intermittent attacks of triphasic color changes: pallor, cyanosis, and then rubor.9 The most important element is pallor, during which the digits turn chalk white. Attacks last 15 to 60 minutes, and rewarming the hands restores normal color and sensation. Color changes do not occur above the metacarpophalangeal joints and rarely involve the thumb. Arteriovenous Fistulae: Arteriovenous malformations and fistulae, although rare, must be distinguished from vascular bruits or aneurysms. True aneurysms and arterial stenoses are associated with a systolic murmur. Pseudoaneurysms generally have a loud systolic and sometimes a separate faint diastolic murmur. Arteriovenous fistulae have a constant systolic and diastolic (to-and-fro) murmur heard best directly over the lesion and often associated with a palpable thrill, precisely analogous to the findings of a therapeutic dialysis arteriovenous fistula. Unless congenital, arteriovenous fistulae occur at prior operative or trauma sites. The skin overlying the lesion may be warm, but distally the temperature is often decreased. Veins peripheral to the fistula are usually distended and varicose. Large and long-standing arteriovenous fistulae produce high cardiac output and widened pulse pressure. Digital pressure on the artery leading to the fistula or the fistula itself may decrease the tachycardia (Branham’s sign). Ultrasound is useful in detecting and evaluating atherosclerotic plaques and mural thrombi and in sizing aneurysms of the abdominal aorta and iliac, femoral, and popliteal arteries.10 B-mode ultrasonography is noninvasive, painless, less expensive than other modalities, and universally available and is the diagnostic procedure of choice for the initial evaluation and determination of the size of peripheral artery aneurysms. Bedside ultrasound can lead to rapid diagnosis of life-threatening conditions and reduce the number of delayed or invasive diagnostic procedures.11 B-mode duplex ultrasonography combines the image of B-mode ultrasonography and sophisticated online computer analysis of accurately sampled Doppler waveforms to allow simultaneous acquisition of both the image of a vascular structure and the characteristics of blood flow velocity within it. Duplex scanning permits noninvasive and accurate diagnosis of peripheral vascular, cerebrovascular, and venous disease. Angiography is the definitive test of abnormal peripheral artery anatomy but is often inconclusive about the physiologic condition of the tissues. Adverse effects of contrast media and catheter-related complications must be weighed against the benefits of this procedure. Contrast media have a direct toxic effect on vascular endothelium; can produce renal failure, especially in diabetic patients; may cause peripheral vasodilation with hypotension; may result in seizures and stroke in patients with neurologic conditions; and can cause severe idiosyncratic and allergic reactions. Catheter-related complications, including embolization, catheter breakage, and vascular disruption, vary with operator skill and anatomic location but average 0.5%. The overall mortality rate from angiography is 0.03%.11 Emergency angiography is usually necessary in the following circumstances: (1) acute arterial embolus or thrombosis if the clinical diagnosis is uncertain, (2) consideration of emergency vascular bypass grafting, and (3) characterization of vascular abnormality before emergency surgical correction. Computed tomography angiography is the most useful test for evaluation of the abdominal aorta.12 In the peripheral arteriovascular system, CT angiography is useful primarily for atherosclerotic, infected, and false aneurysms and for imaging the cerebral circulation. Magnetic resonance imaging (MRI) has the capability for angiography (magnetic resonance angiography) and has been particularly useful in delineating cerebrovascular problems (see Chapter 101); it is seeing expanded use in the evaluation of peripheral vascular disease. The ability to make axial, coronal, and sagittal sections provides accurate visualization of anatomy. MRI detects changes in the relaxation variables of tissues before obvious structural changes, uniquely differentiating blood, thrombus, fat, and fibrosis. The management of acute arterial occlusion depends on the degree and cause of ischemia. Patients with limb-threatening ischemia from embolism should undergo emergency Fogarty catheter embolectomy.13 Patients with limb-threatening ischemia caused by in situ thrombosis require direct or Fogarty catheter thrombectomy combined with vascular bypass grafting. Thrombectomy alone often fails because of recurrent thrombosis. Patients who have a lesion that cannot be bypassed, who have evidence of irreversible ischemia, or who are too ill to tolerate revascularization are treated with primary amputation. A patient with non–limb-threatening ischemia from embolism still is treated with Fogarty catheter embolectomy. Non–limb-threatening ischemia from in situ thrombosis is managed nonoperatively with immediate systemic heparinization and possibly with intra-arterial fibrinolytic therapy (see Fig. 87-1). Acute Anticoagulation with Heparin: For acute arterial embolism, acute arterial thrombosis, and subclavian vein thrombosis, heparin is indicated at standard intravenous doses (80 units/kg by intravenous bolus, followed by a maintenance infusion of 18 units/kg/hr). Heparin quickly reduces thrombin generation and fibrin formation, minimizing clot propagation, which can intensify limb ischemia and jeopardize tissues. Relative contraindications include recent neurosurgery (especially within 2 weeks), major surgery within 48 hours, childbirth within 24 hours, a known bleeding diathesis, thrombocytopenia, a potentially hemorrhagic lesion, and active bleeding. Fibrinolytic Therapy: Low-dose intra-arterial fibrinolytic therapy is increasingly used for acute arterial occlusion. Patients with limb-threatening ischemia are not candidates because clot lysis generally takes 6 to 72 hours. Patients with limb-threatening ischemia cannot tolerate several more hours of ischemia without tissue or limb loss. Fibrinolytic therapy is generally reserved for patients with in situ thrombosis and non–limb-threatening ischemia. Fogarty Catheter Thrombectomy: The Fogarty catheter is most frequently used for iliac, femoral, and popliteal embolectomy, often with only local anesthesia.13 Aortic saddle embolus is removed by sequentially passing the Fogarty catheter through bilateral common femoral arteriotomies. Peripheral Percutaneous Transluminal Angioplasty: The initial success and long-term patency achieved with angioplasty depend on the location of the lesion and the extent of atheromatous disease. Proximal larger arteries (e.g., iliac, femoropopliteal) have the best initial and long-term results. Discrete stenotic lesions (<5 cm) have better long-term patency rates than vessels that are diffusely involved or have multiple involved segments. Balloon angioplasty is the accepted treatment for isolated stenotic lesions in the renal, iliac, and superficial femoral vessels. Transluminal angioplasty with intravascular stent is used in more distal vessels, including the popliteal and tibial circulation, in cases of more diffuse lesions, and for patients who are prohibitive surgical risks, although its value remains to be determined.14 Grafting: Vascular grafting is associated with a variety of complications that can be diagnosed in the emergency department. Autogenous vein grafts (usually a reversed greater saphenous vein) provide excellent long-term patency for small arteries. Vein grafts respond to arterial pressure with gradual intimal proliferation and medial fibrosis. They may develop atherosclerosis, which can lead to graft stenosis and thrombosis. False aneurysms can form along the suture line. Vascular grafts can be used to bypass arterial occlusions and reconstruct a diseased arterial bifurcation, or can be interposed between sections of resected artery. The two most common complications of both prosthetic and vein grafts are thrombosis and development of a false aneurysm at one or more suture lines. Bypass grafting is most often used as palliative treatment for symptoms of atherosclerotic occlusive disease. Patients with localized unilateral stenosis (<3-5 cm in length) may have a comparable rate of success with percutaneous transluminal angioplasty with or without stent placement.15 Sympathectomy: Lumbar sympathectomy is no longer used for treatment of ischemia from arterial occlusion. The benefit of sympathectomy in patients with symptomatic Raynaud’s phenomenon is unclear, but it remains a potential intervention to assist healing of superficial ischemic ulcers and relieve rest pain in patients with Buerger’s disease.16 Scant objective evidence indicates that hyperbaric therapy alters the long-term course of chronic obliterative vascular disorders, presumably by accelerating formation of fine vessels. More success has been achieved with healing chronic diabetic ischemic ulcers and salvaging ischemic skin grafts and flaps.17 Referral to a hyperbaric unit for chronic therapy should be made by the patient’s primary physician or vascular surgeon and not in the emergency department. Diseases of Chronic Arterial Insufficiency Arteriosclerosis obliterans is responsible for 95% of cases of chronic occlusive arterial disease. It is most common in persons older than 50 years, but as many as 19% of cases occur in patients aged 30 to 49 years. Men are affected more often than women (5 : 1 to 10 : 1). Approximately one third of patients with arteriosclerosis obliterans have coexistent coronary artery disease. The incidence of diabetes mellitus is 20 to 30%.18 Risk factors for arteriosclerosis obliterans include cigarette smoking, hyperlipidemia, and hypertension. Of patients with arteriosclerosis obliterans, 70 to 90% are smokers when first examined, 75% have hyperlipidemia, and 30% have hypertension.18 Clinical Features and Differential Diagnosis: Acute arterial occlusion from embolism, thrombosis, or trauma is ruled out primarily by history. Atheromatous emboli from proximal ulcerated plaques or aneurysms can cause small scattered ischemic lesions in the toes, feet, or legs, causing blue toe syndrome (Fig. 87-2). The peripheral pulses are present in blue toe syndrome. Exercise-induced claudication must be distinguished from the nocturnal muscle cramps that frequently occur during rest in elderly patients. Aortoiliac occlusive disease must be differentiated from osteoarthritis of the hip, which tends to be more variable from day to day, is not relieved completely with rest, and is not reliably reproduced by the same amount of exercise. Pseudoclaudication from the cauda equina syndrome is caused by narrowing of the lumbar canal from spondylosis, disease of the intervertebral disks, or spinal cord tumor. The symptoms mimic intermittent claudication but are less closely related to exercise and rest than true claudication. Figure 87-2 Clinical presentation of atheromatous emboli, or blue toe syndrome. (Courtesy Gary R. Seabrook, MD.)
Peripheral Arteriovascular Disease
Principles of Disease
Pathophysiology
Clinical Features
Physical Examination
CLINICAL FINDINGS
EMBOLUS
THROMBOSIS
Identifiable source for embolus
Usual, particularly atrial fibrillation
Less common
History of claudication
Rare
Common
Physical findings suggestive of occlusive disease
Few; proximal and contralateral limb pulses normal
Often present; proximal or contralateral limb pulses diminished or absent
Demarcation of ischemia
Sharp
Diffuse
Arteriography
Minimal atherosclerosis; sharp cutoff; few collaterals
Diffuse atherosclerosis; tapered, irregular cutoff; well-developed collaterals
Diagnostic Strategies
Noninvasive Assessment
Contrast Arteriography
Computed Tomography and Magnetic Resonance Imaging
Management Options
Noninvasive Therapy
Invasive Therapy
Hyperbaric Therapy
Specific Arteriovascular Diseases
Arteriosclerosis Obliterans

![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Peripheral Arteriovascular Disease
Only gold members can continue reading. Log In or Register to continue




