60 Pericarditis, Pericardial Tamponade, and Myocarditis
 Key Points
Key Points• The classic symptom of acute pericarditis is sharp, pleuritic retrosternal chest pain that radiates to one or both trapezius ridges and changes with body position.
• The hallmark electrocardiographic findings in patients with pericarditis include diffuse ST-segment elevation with PR-segment depression in the same leads.
• High-dose aspirin or a nonsteroidal antiinflammatory drug with the addition of colchicine is effective treatment of most cases of acute pericarditis.
• Steroids should be avoided in the early treatment of first-time pericarditis because their use may actually increase the chance of recurrence.
• Large pericardial effusions often cause severe tachypnea and dyspnea; however, oxygen saturation levels are usually normal.
• Jugular venous distention is typical in patients with pericardial tamponade, but it may be absent in those with hypovolemia or if the tamponade developed rapidly.
• The hallmark echocardiographic finding in patients with pericardial tamponade is the presence of a large effusion with diastolic collapse of the right heart chambers.
• The classic manifestation of acute myocarditis includes low-grade fever, tachypnea, and tachycardia out of proportion to the fever.
Epidemiology
Acute pericarditis is often subclinical, so its incidence is uncertain. However, rough estimates range from 2% to 6%,1 and this disorder may be responsible for as many as 1 in every 1000 hospital admissions.2 Although acute pericarditis is not usually deadly, it can be painfully disabling if not treated appropriately.
Pericarditis
Pathophysiology
Pericarditis refers to inflammation of the layers of the pericardium. It has many possible causes (Box 60.1), but in most cases the cause is unknown. In the majority of these idiopathic cases the presumed cause is viral, although most attempts to prove a viral cause have low yield. The most common viral cause is coxsackievirus B. The most common cause of pericarditis worldwide is tuberculosis.3
Presenting Signs and Symptoms
Classic
Chest pain is the typical complaint of patients with acute pericarditis. Classically, the chest pain is sharp, retrosternal, and pleuritic, and it radiates to one or both trapezius ridges because the phrenic nerve, which traverses the pericardium, innervates these muscles.4 Typically, the pain also changes with body position: it improves when the patient sits up and leans forward and worsens when the patient lies supine.
The physical examination of patients with acute pericarditis is usually nondiagnostic. Although some researchers report the presence of a friction rub in up to 85% of patients at some point in the course of the disease,5 the presence of a friction rub at the time of initial evaluation is unreliable. When a friction rub is present, it is best heard at the left sternal border at end-expiration with the patient leaning forward. The rub is usually described as consisting of three components that correspond to atrial systole, ventricular systole, and rapid diastolic filling. A friction rub is thought to be caused by rubbing of the inflamed layers of the pericardium against each other.
Differential Diagnosis and Medical Decision Making
A thorough differential diagnosis of a patient with chest pain is described in Chapter 54. However, the most important initial consideration should always be the deadly causes of chest pain: pericarditis, acute coronary ischemia or infarction, thoracic aortic dissection, and pulmonary embolism. Table 60.1 lists some historical and physical examination features that are helpful in distinguishing among these conditions. Distinction among these causes of chest pain is critical in terms of treatment; patients with pulmonary embolism or myocardial infarction often require treatment with anticoagulants and thrombolytics, medications that can be deadly in patients with acute pericarditis or aortic dissection.
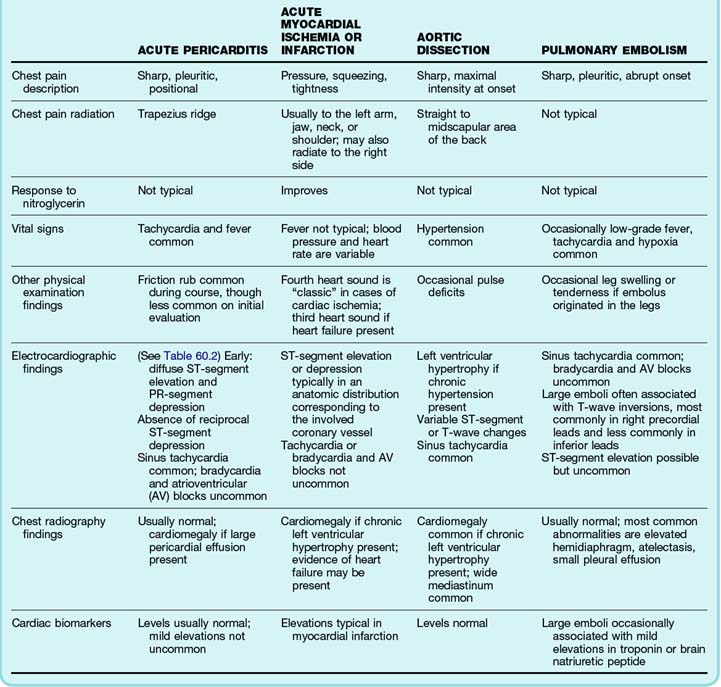
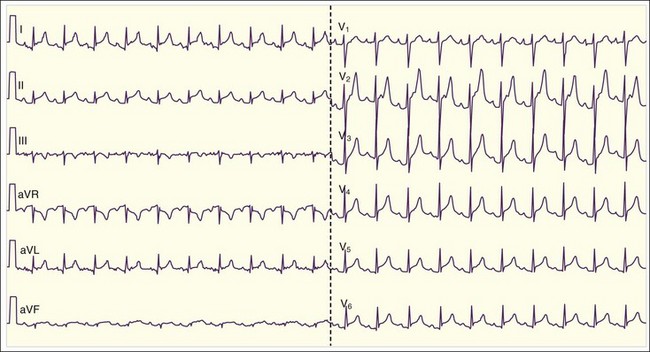
The diagnosis of acute pericarditis is based primarily on the clinical findings. In many cases an electrocardiogram (ECG) is helpful in confirming the diagnosis. Sound knowledge of the ECG findings in patients with acute pericarditis is critical, as well as some findings that help in diagnosing pericarditis versus myocardial infarction (see Table 60.1). Classically, pericarditis evolves through four ECG stages as described in Table 60.2. The first stage of acute pericarditis, characterized by diffuse ST-segment elevation and PR-segment depression or downsloping (Fig. 60.1), is the most common stage encountered in the emergency department (ED). The ST segments should be concave upward; a convex upward (“tombstone”) morphology virtually excludes the diagnosis of pericarditis and rules in acute myocardial infarction. ST-segment depression may be present in leads aVR and V1 in a patient with pericarditis but is unlikely to be present in any of the other 10 leads. In fact, the presence of ST-segment depression in any of the other 10 leads should be considered the “reciprocal” changes of acute myocardial infarction.
Table 60.2 Electrocardiographic Stages of Acute Pericarditis
| Stage I | Diffuse ST-segment elevation and PR-segment depression (except in leads V1 and aVR) |
| Stage II | Resolution of the ST-segment and PR-segment changes T-wave flattening in the same leads |
| Stage III | T-wave inversions in the same leads |
| Stage IV | Normalization of electrographic abnormalities |
Treatment
Treatment of patients with acute pericarditis should be targeted at the underlying cause. The majority of patients with viral, rheumatologic, posttraumatic, or idiopathic pericarditis are effectively treated with high-dose aspirin (2 to 4 g daily) or nonsteroidal antiinflammatory drugs (NSAIDs). Ibuprofen is effective in most cases and has fewer side effects than other NSAIDs; the pain usually improves significantly within days with ibuprofen therapy. If the patient’s symptoms persist, an alternative NSAID is indicated. Indomethacin is often used for severe cases because of its stronger antiinflammatory effect, although it should be avoided in patients with a history of ischemic heart disease because it may decrease coronary blood flow.4,7 Evidence now suggests that addition of colchicine (1.0 to 2.0 mg for the first day and then 0.5 to 1.0 mg/day for 3 months) to the standard regimen is effective in hastening the resolution of acute symptoms and also preventing recurrence rates, regardless of the cause of the pericarditis.8 Colchicine is also effective in cases of recurrent pericarditis.9,10 The use of corticosteroids is generally reserved for recurrent cases of pericarditis that are unresponsive to aspirin or NSAIDs plus colchicine. Initiation of steroids early in the course of first-time pericarditis may actually be an independent risk factor for recurrence.8







