Percutaneous Lumbar Disc Decompression
A vertebral disc is built like a jelly doughnut. The inner jelly part is the nucleus pulposus and the outer layer is the anulus fibrosus (Fig. 31-1). The anulus fibrosus can become weak, which causes the nucleus pulposus to herniate into it and sometimes through it. This herniation of disc material out of its normal position causes compression and irritation of the adjacent nerve root (Fig. 31-2). This irritation is termed radicular pain. When a nerve root is irritated, it sends an aberrant signal up to the brain, which is interpreted as pain along the entire nerve. For example, when the L5 nerve root is irritated, it sends an aberrant signal up to the brain, which tricks the brain into thinking pain is not just at the nerve root but along the course of the entire L5 nerve. People often describe this sensation as a burning, electric, sharp pain that can be constant or intermittent. It starts in the lower back/buttocks and radiates down one leg or both.
Most disc herniations (90%) occur in the disc that lies between the fourth and fifth lumbar vertebral bodies (L4–L5) and the disc that lies between the fifth lumbar vertebral body and the sacrum (L5–S1). This is a matter of physics, because the greatest range of motion in the spine is at the L4–L5 and L5–S1 levels.
Practitioners use several measures for treatment for radiculopathy caused by a herniated disc. Earlier chapters discuss these techniques.
Fluoroscopically guided epidural steroid injections. The steroids decrease inflammation at the site of injury.
Medication. First-line agents include antiseizure and/or antidepressant medications used for neuropathic pain.
Physical therapy. This can alleviate pressure on the spine by strengthening core muscles and increasing flexibility.
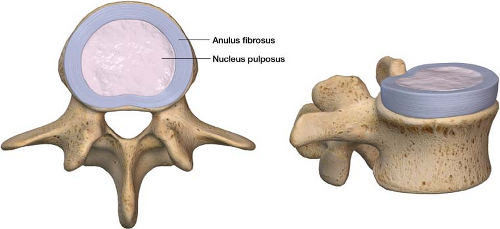
Figure 31-1 Anatomy of a vertebral disc. Inner nucleus pulposus and outer anulus fibrosus.
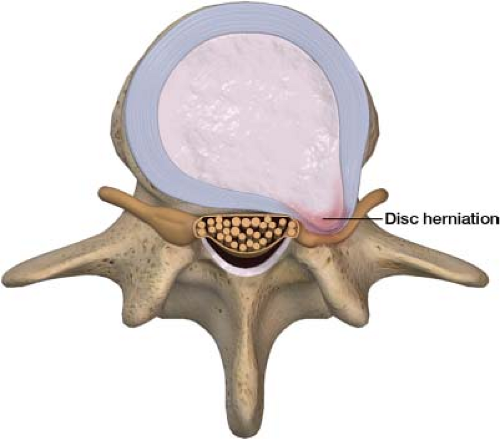
Figure 31-2 Irritation of a nerve root caused by a herniated disc.
Spinal cord stimulation. Electrical current is used to alter pain perception.
The development of interventional pain management, however, has led to an explosion of techniques that attempt disc decompression with minimally invasive approaches.
One interventional technique used to treat radicular pain focuses on decreasing the amount of nucleus pulposus tissue. The goal is to decrease the amount of internal disc pressure by removing some of the nucleus pulposus, which allows the disc to implode back to its original form (Fig. 31-3). The objective of the procedure is to relieve pressure on the affected nerve root without damaging surrounding tissue and to minimize postoperative complications. Pressure transducers placed in the disc have recorded a significant drop in intradiscal pressure after nucleus pulposus extraction.1 A list follows of historical interventional procedures aimed at reducing intranuclear disc pressure.
Nucleoplasty: A needle with a radiofrequency tip is placed into the center of the nucleus pulposus. Using radiofrequency energy (heat), nucleus pulposus tissue is ablated in a controlled manner. The temperature at the tip of the radiofrequency needle decreases significantly in the tissue not immediately adjacent to the tip during the ablation.
Chemonucleolysis: A needle tip is placed into the center of the nucleus pulposus, and chymopapain – a proteolytic enzyme – is injected into the nucleus pulposus. The enzyme degrades nucleus pulposus tissue. The downside of this procedure is that it is difficult to predict how much material the enzyme will digest. If the enzyme is released outside the nucleus pulposus, it could possibly cause neurologic damage.
Percutaneous Laser Discectomy: This is similar to nucleoplasty, but rather than using heat from a radiofrequency tip a laser is used to vaporize a portion of the nucleus pulposus. Heat transfer from the procedure remains a significant concern.
Reimbursement for these historical lumbar disc decompression procedures, in which there is no physical removal of disc material, is no longer covered. In these procedures it is also unclear how much disc material is removed, if any. Mechanical percutaneous lumbar disc decompression with nuclear extraction has become a mainstay of minimally invasive disc
decompression. This procedure involves insertion of an introducer needle into the nucleus pulposus. A smaller needle with an augerlike device that rotates at high speeds passes through this introducer needle (Fig. 31-4). The auger is turned on and disc material is physically extracted.
decompression. This procedure involves insertion of an introducer needle into the nucleus pulposus. A smaller needle with an augerlike device that rotates at high speeds passes through this introducer needle (Fig. 31-4). The auger is turned on and disc material is physically extracted.
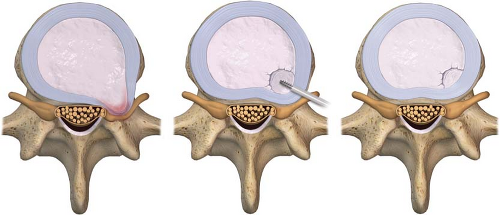 Figure 31-3 A herniated disc imploding back to its original form after part of the nucleus pulposus is removed reducing the amount of internal disc pressure.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





