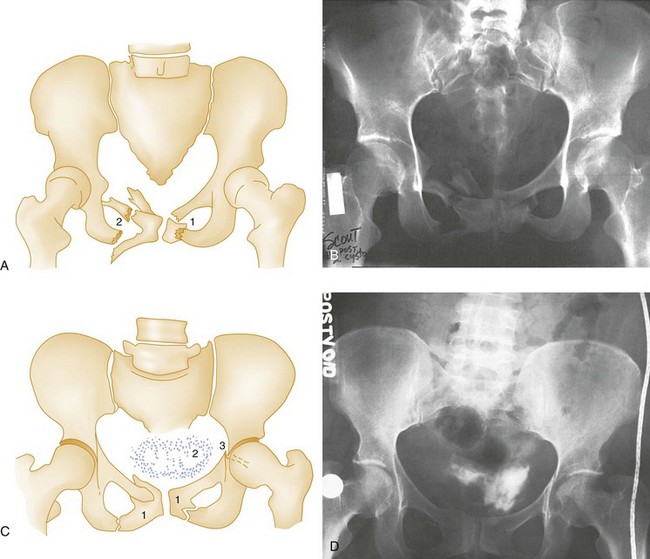
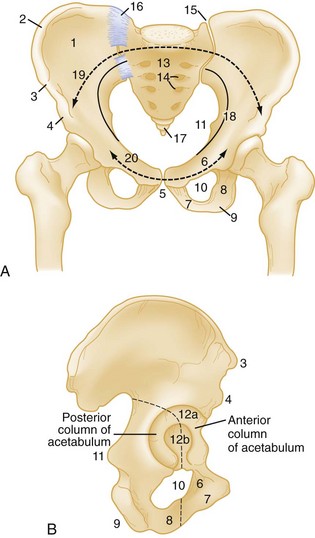
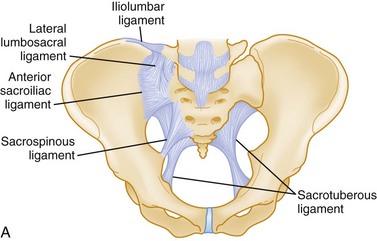
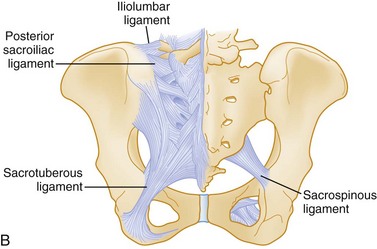
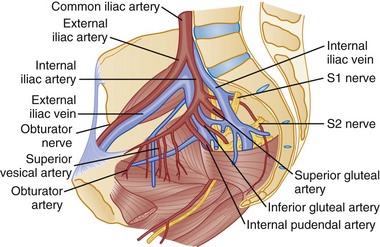
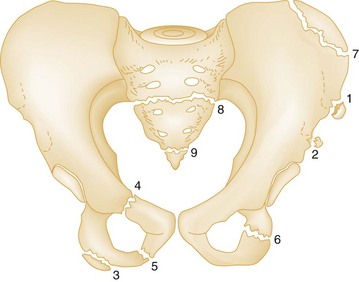
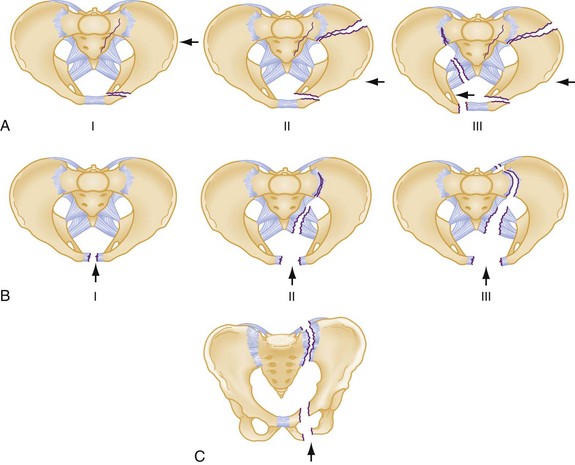
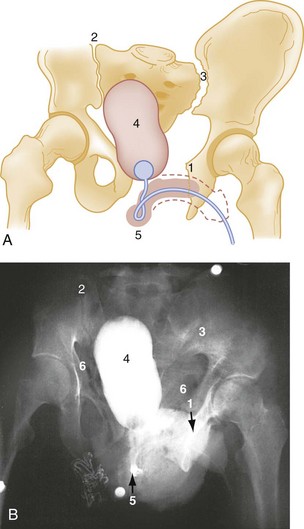
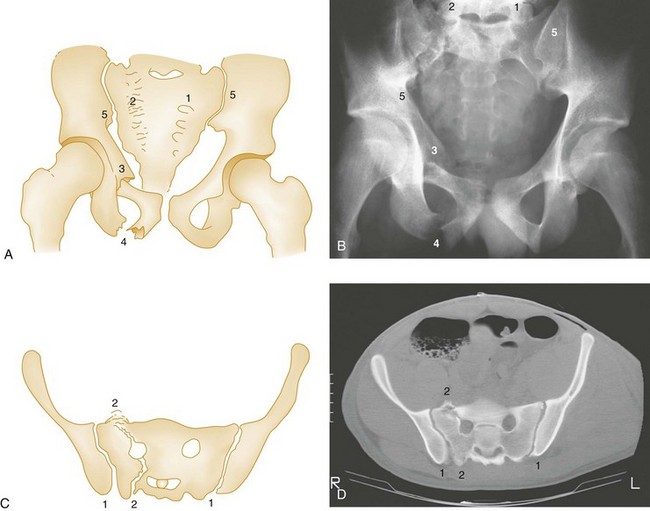
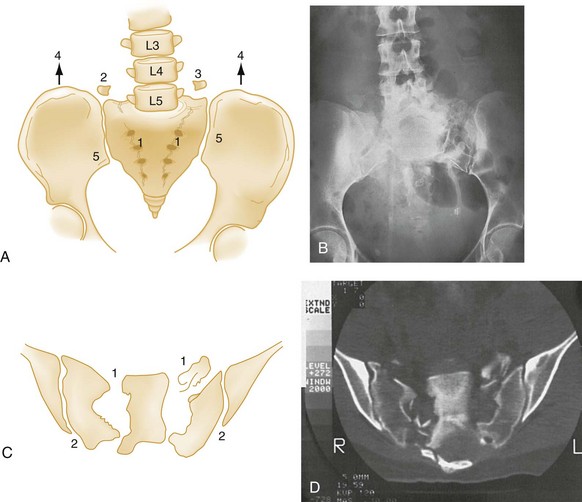
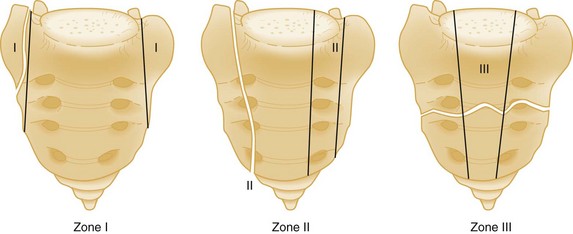
Chapter 55 Based on data from trauma registries, the majority of high-energy pelvic ring injuries are caused by motor vehicle collisions (MVCs), motorcycle crashes, and pedestrians being struck by motor vehicles, together accounting for 80 to 84% of pelvic fractures; and falls from height, which account for 5 to 12%1–5 of pelvic fractures. The mortality rates reported in the literature associated with pelvic fracture range from 9 to 22%1–5; in studies of large cohorts of trauma patients, the presence of pelvic fracture has been consistently shown to be an independent risk factor for death compared with trauma patients without pelvic fracture.6–8 Patients with pelvic fractures and with shock on arrival to the hospital have mortality rates of 33 to 57%.3,4 Increased age, shock on arrival at the hospital, high injury severity and revised trauma scores (which generally reflect the presence of multisystem injuries), and the need for transfusion have all been shown to increase the risk of death.3–5,9,10 The mortality rate among pedestrians struck by motor vehicles who sustain pelvic injury has been shown to be 23%.11 Despite advances in motor vehicle safety design, MVCs continue to be a major cause of pelvic fracture. Rates of pelvic fracture secondary to MVC range from 10 to 28%.9,12,13 Lateral impact remains the most prevalent mechanism for pelvic trauma in collisions, for which the widespread advent of front airbags has little effect. Some have speculated that the increased popularity of sport-utility vehicles in past decades is contributing to the severity of side-impact injuries, specifically as a result of the higher bumper in these vehicles striking the side of lower cars.9,12,14 The pelvic ring is made up of right and left innominate bones and the sacrum. The innominate bones consist of the pubis, ischium, and ilium (Fig. 55-1). The bony pelvis provides protection for its visceral contents, serves as attachment points for muscles, and transmits weight from the trunk to the lower limbs. The main weight-bearing forces are transmitted through the posterior wall of the pelvis, called the posterior arch, which is composed of thick bone and ligaments. The rich network of major arteries, veins, and nerves that course in front of the posterior arch may be injured concomitantly with forces causing bony injuries of this arch. Knowledge of the ligamentous attachments of the pelvic ring is crucial to understanding how stability is maintained or disrupted in pelvic injury. The stability of the pelvis is maintained by ligaments, as well as the muscles and fascia that make up the pelvic floor. Anteriorly, the symphysis pubis provides the major mechanical stability. Posteriorly, a complex of strong ligaments—the sacrospinous, sacrotuberous, iliolumbar, and anterior and posterior sacroiliac (SI) ligaments—maintains the integrity of the posterior arch (Fig. 55-2). It is important to appreciate that mechanically unstable pelvic fractures are unstable primarily because of the disruption of these posterior ligaments. Most of the blood supply to the pelvis comes from the left and right internal iliac arteries. The internal iliac arteries course at the level of the SI joints. The various arteries that derive from the internal iliac arteries initially run in close proximity to the posterior pelvic arch and eventually anastomose extensively with one another, forming a rich collateral network (Fig. 55-3). The superior gluteal artery is the largest branch and is commonly injured in fractures of the posterior pelvic arch. The obturator and internal pudendal branches are often injured in fractures involving the pubic rami. Numerous classification schemes exist for pelvic fractures. Two widely used schemes for pelvic injury are presented here. The classification by Tile stresses the biomechanical stability of the pelvic ring15 (Box 55-1). The Young-Burgess classification emphasizes the mechanisms of injury16 (Box 55-2). From a practical viewpoint, it is highly useful to consider both of these elements in the assessment of a pelvic ring fracture. Within both classification systems exist numerous subtypes of injuries, the interobserver reliability of which has been questioned.17,18 For the emergency physician, a good understanding of both the underlying principles of pelvic stability and mechanisms of injury is far more important than a detailed knowledge of the numerous subtypes of injury that exist within the classification schemes. The broad distinction of mechanically stable from unstable fractures of the pelvic ring is clinically useful to bear in mind in assessing patients, as it has been demonstrated consistently over time that those with unstable injuries have higher mortality and greater transfusion requirements.16,19,20 Fractures of individual bones without involvement of the pelvic ring represent one third of all pelvic fractures. In general, most stable pelvic fractures heal well with rest and analgesic drugs for pain control (Fig. 55-4).15 Undisplaced or Minimally Displaced Fractures of the Pelvic Ring.: The normal pelvis is not totally rigid because of the slight mobility at the SI joints and symphysis pubis and the inherent elasticity of bone. A single break in the ring is possible. Nevertheless, the pelvis is not totally forgiving, and identification of a single break in the ring should prompt a search for a second disruption. If the patient with a ramus fracture reports posterior pelvic pain and plain radiographs do not reveal posterior injury, further investigations may reveal occult posterior fractures. A study performed more than 35 years ago found that patients who sustained apparently isolated pubic ramus fractures showed increased uptake of radionuclides on bone scans in the acetabulum and SI joint, suggesting that occult bony or ligamentous injury accounted for the pain.21 More recently, a study that prospectively evaluated elderly patients who were diagnosed with isolated ramus fractures on plain films found that 95% had sacral fracture detected by magnetic resonance imaging (MRI).22 This study does not imply a need to perform MRI on all elderly patients with ramus fractures in the ED; rather, it enhances our understanding of the pathophysiology of ramus fractures and underscores the importance of adequate analgesia in these patients. The lateral compression type I fracture described by Young and Burgess (Fig. 55-5)—characterized by pubic ramus fracture with ipsilateral sacral compression—bears special consideration among the mechanically stable pelvic fractures, as it has been shown to be associated with a mortality rate of 8% with a high incidence of associated injuries.20,23,24 Also termed a straddle fracture, four-pillar injuries involve fractures of both pubic rami on both sides of the symphysis pubis, causing the so-called “butterfly segment” (Fig. 55-6). The injury is produced by a direct blow with a straddle mechanism. Although these fractures may occur without posterior arch disruption, four-pillar injuries are also commonly associated with lateral compression or vertical shear forces that may cause concomitant injuries to the posterior pelvic arch. CT of the pelvis is required in cases of four-pillar injuries to detect and classify precisely the posterior arch injury and plan orthopedic treatment.15 The genitourinary tract frequently is injured concomitantly with this type of pelvic fracture and should be evaluated carefully (see Fig. 55-6). Figure 55-6 Four-pillar (straddle) fracture. A and B, Partial inlet view of pelvis shows straddle fracture. (1) and (2) Marked comminution of left pubic bone and comminuted right superior and inferior rami. This partial inlet projection shows displacement of fragments into the pelvis, which is not evident on the anteroposterior view of the same patient in C and D. A true inlet projection and computed tomography scan (not available) would provide further information about the posterior arch, which is injured frequently in straddle fractures and should be imaged (see text). C and D, Postvoid cystogram of the same patient with anteroposterior pelvis. (1) Fractures of pubic rami are seen again but do not appear to be as displaced compared with A and B because this projection is an anteroposterior view. Even minor degrees of angulation of the x-ray beam can change the appearance of pelvic fracture displacement. (2) Extravascular contrast indicates bladder rupture; (3) left acetabular fracture is seen in this projection but not in B because of the difference in projection. The acetabular fracture disrupts the ilioischial line (see also Fig. 55-13) and is a posterior column fracture. Isolated fracture of the iliac wing was described by Duverney in 1751 and now bears his name. It is caused by direct trauma to the iliac crest, usually by lateral compression forces. Although displacement is usually minimal because of the arrangement of the muscle attachments of the abdominal wall, orthopedic consultation is recommended. The fracture may extend into the acetabulum, altering the treatment and prognosis. Severely displaced fractures of the iliac wing require open reduction and internal fixation.15 It is worth noting that a high incidence of major associated nonpelvic injuries among patients with isolated iliac wing fracture has been reported.23 Transverse Fractures of the Sacrum.: Transverse fractures of the sacrum do not compromise the pelvic ring. Transverse fractures at or below S4 are unlikely to be accompanied by neurologic injury.25 An upper sacral transverse fracture is the result of a flexion injury, such as being struck on the lower back by a heavy load while bending over, or by direct forces to the sacrum, as in a fall from a great height.25 The patient reports pain in the buttocks, perirectal area, and posterior thighs. There may be local pain, swelling, and bruising overlying the sacrum, and on gentle bimanual rectal examination, severe pain, abnormal motion, and palpable hematoma may be elicited. Radiographically, the fracture may be difficult to visualize on anteroposterior (AP) and lateral projections, in which case a pelvic outlet view may be helpful. Simple transverse fractures at or below S4 are treated conservatively. Above S4, neurologic injuries are common, necessitating careful clinical evaluation and surgery when neurologic compromise is present. Avulsion Fractures.: These usually occur during athletic activities and are the result of a sudden, forceful muscular contraction or excessive muscle stretch. They are seen more commonly in older children and teenagers before closure of the corresponding physis occurs; adults may have the same symptoms from ligamentous injury at these sites without radiographic abnormality. A portion of the iliac crest epiphysis may be avulsed by contraction of the abdominal muscles. Similarly, the anterior superior iliac spine may be avulsed by forcible contraction of the sartorius muscle. Forceful contraction of the rectus femoris (as in kicking a ball) can result in the less common injury of anterior inferior iliac spine avulsion; however, this radiographic finding should be distinguished from a normal variant, the os acetabuli, which is a secondary center of ossification at the superolateral margin of the acetabulum.26 Clinical examination is similar in these injuries and reveals local pain, swelling, and limitation of motion. Stress Fractures.: Stress fractures occur with vigorous athletic or military training and in the last trimester of pregnancy.27 The diagnosis of stress fractures is based on the clinical evaluation and can be confirmed, if required, by radionuclide bone scan, although MRI has been shown to be a superior method for detecting these injuries.28 Anteroposterior Compression.: Severe AP compression forces result in disruption at or near the symphysis pubis. Symphysis widening of less than 2.5 cm is considered a stable injury (the symphysis should normally be ≤0.5 cm in an adult but can increase 2-3 mm during or after pregnancy); however, with continued force in the AP direction, the hemipelvis externally rotates, tearing the sacrospinous, sacrotuberous, and anterior SI ligaments. The SI joint opens and hinges on the intact posterior SI ligaments. The resulting injury is aptly described as an “open-book” fracture. The pelvis is rotationally unstable in the horizontal plane, but the intact posterior SI ligaments maintain vertical stability.15,16 When diastasis of the pubic symphysis is greater than 2.5 cm on the AP radiograph, the posterior injury is usually seen as widening of the SI joint and occasionally as a sacral or iliac fracture (see Fig. 55-5).15 If the injurious forces continue, they may separate the hemipelvis, and the SI joint is seen as widely separated on the plain AP radiograph (Fig. 55-7) and the CT scan.15 The AP radiograph may be misleading in suggesting a pure open-book fracture in cases with symphysis disruptions greater than 2.5 cm. These cases commonly are associated with vertical shear fractures, and careful clinical and computed tomography (CT) assessment for vertical instability is essential to classify the fracture properly and plan treatment.15 These same forces also may injure the neurologic and vascular structures at the posterior arch; the overall volume of the pelvis is increased in the open-book injury, facilitating the expansion of a retroperitoneal hematoma. Several studies have demonstrated that patients with severe grades of AP compression injuries have the highest crystalloid and blood requirements.16,19 Lateral Compression.: Lateral compression of the pelvic ring results in varying degrees of internal rotation of the affected hemipelvis. Initially, this causes buckling of the sacrum and horizontal pubic rami fractures. Rami fractures may occur on the ipsilateral or contralateral side, the latter being referred to as the “bucket-handle” fracture (Fig. 55-8). Similar to the AP injury, with increasing disruption of the posterior ligaments comes increasing rotational instability. In the most severe lateral compression trauma, the ipsilateral pelvis internally rotates to such a degree that the contralateral pelvis may externally rotate. This is referred to as the “windswept” pelvis. Lateral compressive injuries result in varying degrees of horizontal rotational instability; however, the vertical stability of the pelvis is maintained (see Fig. 55-8). Vertical Shear.: Vertical shear injuries represent the most unstable injuries to the pelvic ring and are associated with violent axial loading of the hemipelvis (e.g., fall from height, “submarining” underneath a dashboard). Fractures occur in vertical planes. Anteriorly, the symphysis and rami may be disrupted. Posteriorly, gross displacement and instability in the rotational and vertical planes may be present through the sacrum, the SI joint, or the ilium such that the hemipelvis may displace posteriorly and cephalad15,16 (see Fig. 55-9). Avulsion of the ischial spine, the lower lateral lip of the sacrum, and the transverse process of the fifth lumbar vertebra (sites of insertion of ligaments) (Fig. 55-9 and Box 55-3) are important clues to the presence of vertical shear fractures.15 The vertical shearing forces transmitted through the bony pelvis are also transmitted through the rich vascular network and nerve plexus that are directly adjacent to the bone. This activity accounts for the major hemorrhage and neurologic injuries associated with vertical shear fractures. Vertical Sacral Fractures.: A crucial distinction in considering sacral fractures is that transverse fractures do not involve the pelvic ring, but vertical fractures do. Vertical sacral fractures are caused by high-energy injuries and were classified by Denis into three groups according to whether the fracture line extends (1) laterally to the sacral foramina, (2) through the foramina, or (3) medially to the foramina, involving the central spinal canal29 (Fig. 55-10). The radiographic diagnosis of this fracture hinges on careful examination of the symmetrical cortical lines that are normally present at the superior margins of the sacral foramina on the AP view. Disruption, distortion, or asymmetry of these lines is an important marker of sacral fractures.26 There is a high risk of neurologic complications associated with these injuries: 6% when lateral to the foramina, 28% when through the foramina, and 58% when medial to the foramina.29 Neurologic dysfunction correlates to the nerve roots involved but may include any bowel, bladder, or sexual dysfunction. Surgery is commonly performed for fractures associated with neurologic dysfunction, with the goals of bony fixation of the sacrum and decompression of affected nerve roots. An open pelvic fracture is present when there is direct communication between the fracture site and a skin, rectal, or vaginal wound. These are potentially lethal injuries, especially if the open nature is not recognized: hemorrhage accounts for early mortality, but infection, sepsis, acute respiratory distress syndrome, and multisystem organ failure are all causes of delayed death.24,30 The majority of case series before 1991 reported mortality rates greater than 50%; rates reported from 1991 to 1999 ranged from 5 to 30%,30 although a recent series reported a 45% mortality rate.31 The skin over the posterior pelvis and gluteal area and perineum is inspected carefully for wounds. Some fractures are open only by virtue of a bone spicule penetrating the vagina or rectum and are identified by careful digital rectal examination (DRE) and vaginal examination. Hemorrhage from a large open laceration should be treated by direct manual pressure or pressure dressing. Pelvic fractures communicating with the rectum have traditionally mandated a diverting colostomy; however, a systematic review of the literature on this topic found no difference in infection rates between patients treated with colostomy and those treated without.32
Pelvic Trauma
Perspective
Epidemiology
Principles of Disease
Bony and Ligamentous Anatomy
Vascular Anatomy
Pathophysiology and Key Patterns of Pelvic Fracture
Stable Injuries (Tile Type A)
Partially Stable and Unstable Injuries (Tile Types B and C)
Open Pelvic Fractures
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Pelvic Trauma
Only gold members can continue reading. Log In or Register to continue




