Pathophysiology and Initial Triage of Acute Coronary Syndromes
John M. Field
In patients with symptoms of possible ACS, some of the traditional risk factors for CAD (e.g., hypertension, hypercholesterolemia, cigarette smoking, family history) are only weakly predictive of acute ischemia. Therefore, the presence or absence of these traditional risk factors ordinarily should not be used to determine whether an individual should be admitted or treated for ACS. Patients who present with ischemic symptoms should undergo early risk stratification using a risk-stratification model.1,2
A Disrupted Plaque as the Proximate Cause of ACS
Usually a Nonocclusive Plaque in the Infarct-Related Artery
Triage Priorities for ACS—Not Only the Traditional Risk Factors
A Systematic Approach—Key to Selecting a Strategy
Introduction to Acute Coronary Syndromes
An acute coronary syndrome (ACS) due to a disrupted plaque is present in the majority of patients with adult cardiac arrest.3,4 Alarmingly, the first prolonged episode of ischemic discomfort has a 34% fatality rate. More than half the patients with sudden cardiac death (SCD) have no prior symptoms; in 17%, SCD is the first, last, and only symptom.5,6,7 Additionally, the consequences of coronary atherosclerosis and ACS are responsible for the epidemiologic pool of patients at risk for SCD and those with significant cardiovascular morbidity. A conservative estimate for the number of discharges from patients with ACS from hospitals from 2005 is 772,000.7
It is, therefore, appropriate for a textbook on emergency cardiovascular care to begin with a section on acute coronary syndromes. The following chapters by Drs. Nichol and
Mitchell, Hollander, Ornato, Pollock and Summers, Peacock, Dean, and Stahmer set the stage for the broad spectrum of patients who present with cardiovascular emergencies. Currently, there are approximately 15.8 million individuals in the United States with coronary artery disease (CAD). There will be at least 1.4 million new, recurrent, or silent episodes of ACS. About 325,000 of these patients will experience out-of-hospital or emergency department SCD.7
This introductory chapter provides a broad general overview of ACS, focusing on an understanding of the pathophysiology necessary to apply triage and risk-stratification principles. In the following chapters, the authors mentioned above review these principles in current detail for health care providers who are charged with managing patients with ACS during the first several hours after presentation.
Overview of the Acute Coronary Syndrome
Definition and Spectrum of Acute Coronary Syndromes
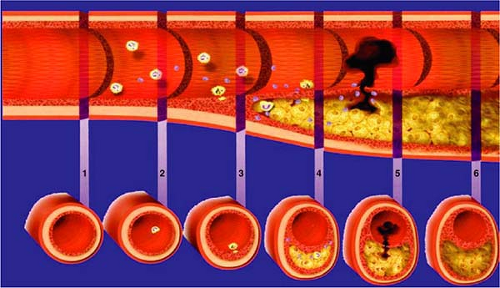
The formation and accumulation of lipid and oxidative byproducts in an arterial wall is called atherosclerosis. When this deposit involves the coronary arteries, it is called coronary atherosclerosis. This process is gradual (Fig. 1-1) and gives rise to no symptoms for the many years of pathologic progression.8