Figure 20.1. Modified Atkinson approach to facial nerve block. The needle is inserted 2 cm lateral to the lateral border of the orbit, which is usually 2 to 3 cm further lateral than the van Lint approach. Infiltration is first performed with 2 or 3 mL as the needle is withdrawn up from its first contact with the bone (A). Local anesthetic is then injected superiorly (B) and inferiorly (C) from this point to catch the spreading fibers of the facial nerve as they surround the eye.
1. A modified Atkinson approach (Figure 20.1) is a simple technique to block the terminal branches of the facial nerve. A 38-mm (1.5-in.) needle is inserted through a skin wheal 2 cm (0.8 in.) lateral to the orbital rim. The needle is advanced first superior toward the upper orbital rim, and 3 to 4 mL of anesthetic injected as it is withdrawn to the insertion point. It is then redirected toward the inferior orbital rim, and a repeat injection is made. Sensory blockade of the lid is achieved by a subcutaneous injection of 1% lidocaine or mepivacaine through this single skin puncture. This approach has less chance of producing periorbital ecchymosis than the classic van Lint approach, and it is less likely to produce a total facial paralysis as would be obtained with a more proximal (such as O’Brien or Nadbath-Rehman) approach.
2. The approach described by Atkinson has the needle inserted over the zygomatic arch at the level of the lateral orbital rim and advanced subcutaneously upward toward the top of the ear. Three to 4 mL of local anesthetic is injected as the needle is withdrawn.
3. The classic van Lint approach (Figure 20.2) is slightly more medial, at a point 2 cm (0.8 in.) posterior to the lateral canthus of the eye. Three milliliters of local anesthetic is injected as the needle is withdrawn to the entry point. The needle is left in the skin and redirected inferiorly and anteriorly, with a similar injection of 3 mL on withdrawal. The two injections should produce a “V” bordering the eye. An additional 2 mL can be injected deeper at the apex of the “V” to provide anesthesia of deeper fibers.
4. O’Brien described a more proximal block of the facial nerve (near the ear). A needle is inserted 1 cm (0.4 in.) anterior to the tragus of the ear, and 2 mL of local anesthetic is deposited subcutaneously. The advantages of this block include producing paresis of the orbicularis oculi and having a less likelihood of producing periorbital ecchymoses, which are disturbing to the patient and family.
5. The Nadbath-Rehman block (Figure 20.3) anesthetizes the facial nerve even more proximally. It is performed by inserting a 16-mm (5/8-in.) needle anterior to the mastoid process at the base of the skull, and directing it superior and posterior in the direction of the stylomastoid foramen (as if aiming for the top of the opposite ear through the skull). After careful aspiration to avoid the nearby carotid artery, the needle is fixed and 3 mL of local anesthetic is injected.
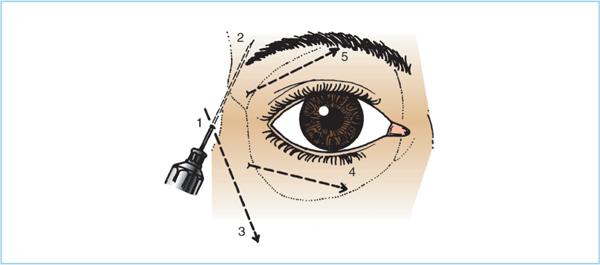
Figure 20.2. Classic van Lint approach to facial blockade. The needle is inserted 2 cm laterally to the lateral canthus of the eye and subcutaneous injection is performed in the superior and inferior borders of the orbit. (From Hersh PS. Ophthalmic surgical procedures. Boston: Little, Brown and Company, 1988:17, with permission.)
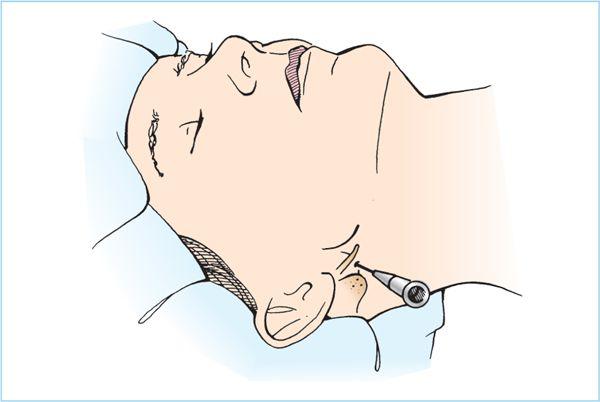
Figure 20.3. Nadbath-Rehman facial nerve block. As most proximal block of the facial nerve, there is often disconcerting facial drooping as a consequence of unneeded sensory and motor blockade of the lower face.
6. Side effects
a. O’Brien and Nadbath techniques produce unneeded sensory and motor blockade of the lower face. The resulting facial drooping may be disconcerting to the patient and family.
b. The more distal techniques, however, carry the risk of ecchymosis (black eye).
c. The choice of injection site is a compromise between these side effects. An alternative is to avoid facial nerve injection by using large volumes of anesthetic with the peribulbar technique.
C. Retrobulbar block is a regional anesthetic technique for ophthalmic surgery that is more commonly practiced by ophthalmologists than anesthesiologists. Placement of the local anesthetic within the muscular cone of the eye can provide faster onset, denser block, and require less anesthetic than other regional techniques such as peribulbar or sub-Tenon blocks.
1. Instillation of topical local anesthetic to the conjunctiva is usually performed as an associated step. Tetracaine 1% or other ophthalmologic preparations are all adequate.
2. The inferior border of the orbital rim is located at a point approximately one-third of the distance from the lateral to the medial canthus. This point is usually directly inferior to the lateral border of the dilated pupil (Figure 20.4). The eye is held in neutral forward gaze; upward medial deviation may rotate the optic nerve and vessels into the intended path of the needle (7).
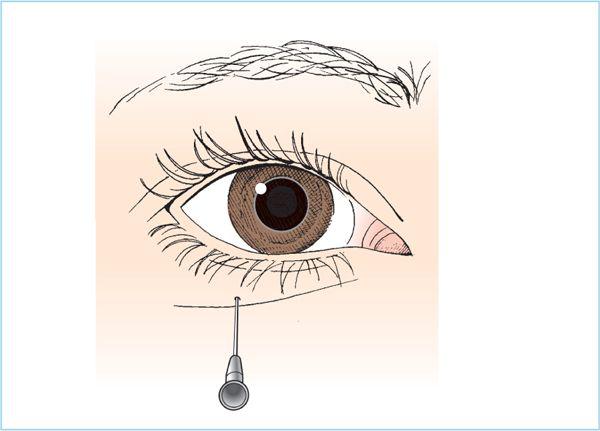
Figure 20.4. Needle placement for retrobulbar block.
3. A 38-mm (1.5-in.) 23-gauge blunt-tipped needle is introduced perpendicularly into the skin and advanced directly posterior parallel to the floor of the orbit (Figures 20.5A and 20.6).
4. After the needle is advanced past the equator of the globe, it is angled superonasally at approximately a 45-degree angle to pass into the muscular cone (Figure 20.5B). Entry into the muscle body will cause the globe to rotate inferiorly, rotating the eye down 15 to 30 degrees. Once the needle passes through the muscle body into the cone, there is an abrupt release of this traction, and the globe springs back to a neutral position (Figure 20.5C). If this release is not obtained, the needle is withdrawn and reinserted.
5. After careful aspiration, 3 to 4 mL of anesthetic is injected slowly. There should be no resistance to injection if the needle is in the cone. Resistance might indicate undesirable intramuscular placement, or entry into the globe, and the needle should be repositioned if it is felt.
6. Scleral perforation should be suspected if the patient complains of pain on injection. Many blocks are performed with sedation, which may mask this sign. Other indications are continued movement of the globe with needle movement once the muscle body is penetrated. Special blunt-tipped needles, which are designed to reduce the chance of perforation of the globe, are available for retrobulbar block, but the best protection is to avoid too shallow an angle when advancing the needle. The greatest risk exists with the myopic patient with an elongated globe. The axial length should be evaluated in all of these patients, and a steeper angle maintained in any patient whose axial length exceeds 25 mm (1 in.). Alternatively, a peribulbar block may reduce the chance of perforation in these patients.
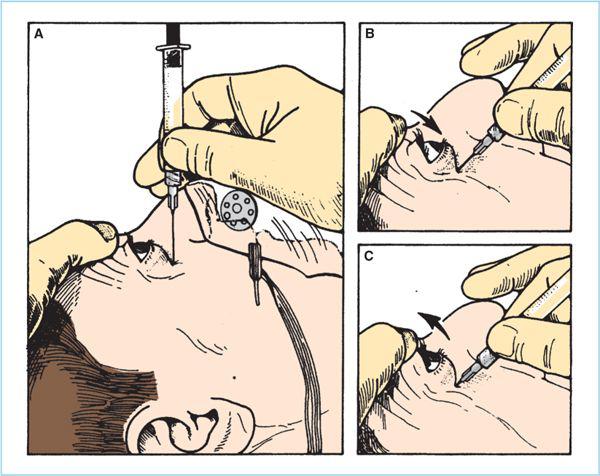
Figure 20.5. Retrobulbar block. A: The needle is inserted perpendicular to the skin at the lateral border of the dilated pupil just above the inferior orbital rim. B: Once the skin is penetrated, the angle of the needle is changed to approximately 45 degrees cephalad and advanced until the globe rotates down as the needle tip enters the muscle cone. C: When the tip penetrates into the central cone, the globe will dramatically rotate back to the neutral position. At this point, 3 mL of the local anesthetic mixture is injected into the retrobulbar area.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


